Ventricular Arrhythmias Jayna GardnerGray 4232020 Abnormal rhythm that

Ventricular Arrhythmias Jayna Gardner-Gray 4/23/2020
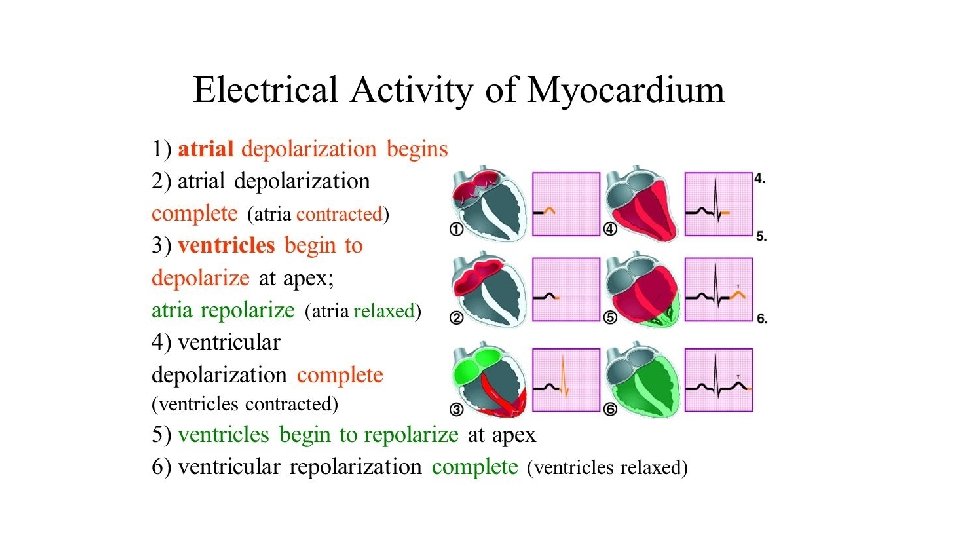

• Abnormal rhythm that originates in the ventricles

• Increased activity of automatic focus in ventricles • Reentry circuit of fast and slow pathway is confined to ventricles
 2) 3) 4) Is my patient in sinus rhythm? Is my patient")
Tachyarrhythmias 1) 2) 3) 4) Is my patient in sinus rhythm? Is my patient stable or unstable? Is my QRS complex narrow or wide? Is my rhythm regular or irregular?

Common Types • Junctional Rhythm • Idioventricular Rhythm • Premature Ventricular Contractions • Ventricular Tachycardia • • Monomorphic Polymorphic Bidirectional LVOT RVOT Fasicular Annular • Ventricular Flutter • Ventricular Fibrillation

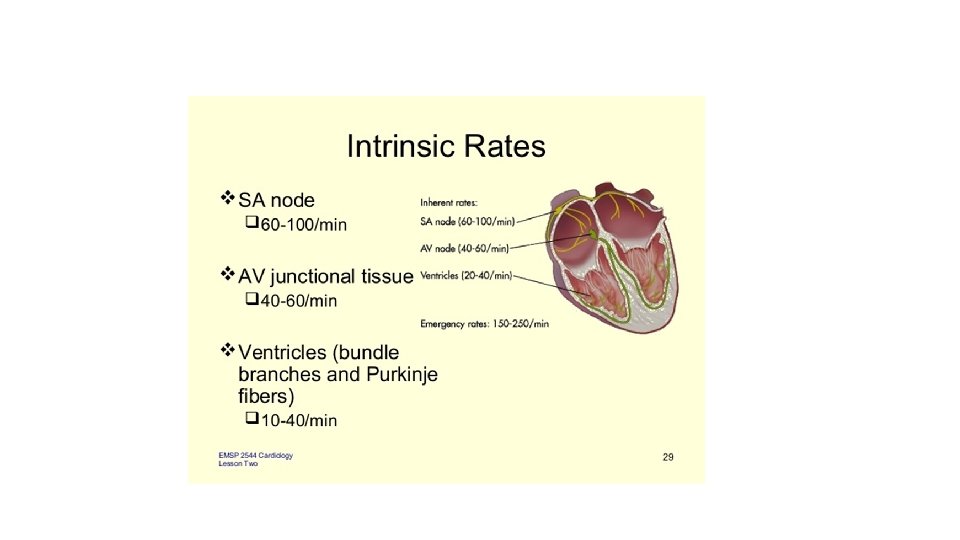
Junctional Rhythm • The electrical activation originates near or within the AV node • Normal His-Purkinje is used, the QRS complex is usually narrow • Rate is 40 -60 beats per minute • P wave is frequently not seen; it can be buried within the QRS complex

Idioventricular rhythm • Originate in the ventricles “slow VT” • All characteristics of VT apply • Heart rate less than 60 bpm idioventricular rhythm • Heart rate between 60 and 120 bpm rhythm accelerated idioventricular

Accelerated Idioventricular rhythm
 with abnormal morphology. •")
Premature Ventricular Contractions • Broad QRS complex (≥ 120 ms) with abnormal morphology. • Caused by electrical irritability • Premature — occurs earlier than would be expected for the next sinus impulse. • Usually followed by a full compensatory pause. • Unifocal or Multifocal • Anxiety, Sympathomimetics, Beta-agonists, Excess caffeine, hypokalemia, hypomagnesemia, digoxin toxicity, myocardial ischemia

• Isolated PVC: no repeating pattern • Bigeminy: every sinus beat followed by a PVC • Trigeminy: Every second sinus beat followed by PVC • Couplet: 2 consecutive PVCs • Triplet: 3 consecutive PVCs • Nonsustained Ventricular Tachycardia: Three or more consecutive PVCs
 • Life threatening")
Ventricular Tachycardia • Most common cause of wide complex tachycardia (80%) • Life threatening arrhythmias that originates in the ventricles • Occurance of 3 or more ventricular beats (100 -250 bpm) • QRS >120 ms • Electrical instability that can cause deterioration to ventricular fibrillation

Ventricular Tachycardias • Until 1961 patients post MI were placed away doctors and nurses to avoid stress and possible arrhythmia • 30% of people with ventricular arrhythmias would die in the hospital post MI • In 1961 the concept of electrical shock to terminate these rhythms was proposed
 vs. non sustained (<30")
Breakdown • Pulseless vs hemodynamically stable • Sustained (>30 sec) vs. non sustained (<30 sec) • Monomorphic vs. polymorphic

Risk of ventricular tachycardia • Acute MI • Electrolyte abnormalities • Post CABG • Dilated cardiomyopathy • Family history: HOCM, congenital long QT syndrome, Brugada syndrome or arrhythmogenic right ventricular dysplasia
 of wide complex tachycardias are VT • SVTs")
SVT vs. VT • Majority (90%) of wide complex tachycardias are VT • SVTs may display widened QRS (BBB, aberration, toxins, hyperkalemia) • SVTs are rarely life threatening • Presence of stability should not be regarded as diagnostic of SVT ***If in doubt treat as VT

SVT vs. VT • The likelihood of SVT with aberrancy is increased if: • Previous ECGs show a bundle branch block pattern • Previous ECGs show evidence of WPW (short PR < 120 ms, broad QRS, delta wave) • The patient has a history of paroxysmal tachycardias that have been successfully terminated with adenosine or vagal maneuvers • Younger patient <35 yo

Brugada Criteria • Most used algorithm • If any of the 5 criteria are met the patient has VT

Brugada Algorithm

1. • Is there concordance present in the precordial leads (leads V 1 -V 6)? "Are all of the QRS complexes completely upright, or downward in the precordial leads? "

2. • Is the R to S interval > 100 ms in any one precordial lead? • Use calibers to measure between the R and S waves in the precordial leads

3. Is AV dissociation present? • AV dissociation occurs when P waves are seen at different rates than the QRS complex.
 • RBBB pattern (upright in")
4. Examine QRS morphology (V 1 -2, V 6) • RBBB pattern (upright in V 1) • LBBB pattern (downward in V 1).
 VT is present if: • A")
If upward in lead V 1 (RBBB pattern) VT is present if: • A monophasic R or biphasic q. R complex in V 1, V 2 • If an RSR' pattern “bunny-ear” is present in V 1 or V 2, with the R peak being higher than the R’ peak • Biphasic r. S complex in V 6

Failed V 1 -2 Brugada criteria
 VT is present if: • A")
If downward in lead V 1 (LBBB pattern) VT is present if: • A wide R wave in lead V 1 or V 2 of >30 ms • Slurred or notched downstroke of the S wave in V 1 or V 2 • Duration of onset of the QRS complex to peak of QS or S >70 ms • QS wave in V 6

• If none of the above criteria are met a diagnosis of SVT can be made

Polymorphic Ventricular Tachycardia • Can cause hemodynamic instability • May degenerate into VF • More likely if HR >220 • QT prolongation: • Medications, electrolyte abnormalities and medical conditions • Bigeminy in a patient with long QT syndrome • PVC occurs during the preceding T wave, known as ‘R on T’ phenomenon. • Abnormal giant T-U waves may precede polymorphic VT

Bidirectional Ventricular Tachycardia • Axis: ? both … QRS axis shifts 180 degrees • Also look like alternating left and right bundle-branch block • Digoxin Toxicity, Long QT syndromes, sarcoidosis, myocarditis, polymorphic VT

Ventricular Flutter • Extreme form of ventricular tachycardia with loss of organized electrical activity • Short lived: swift progression to Ventricular fibrillation • >250 bpm • Treat: standard ACLS

Ventricular Fibrillation • Fatal arrhythmia • Ventricular Rate > 400 bpm • No forward cardiac output • Disorganized activity on ECG
- Slides: 32