Ventilator Associated Pneumonia Linda R Greene Rochester General










: Many studies")
































- Slides: 49
Ventilator Associated Pneumonia Linda R Greene Rochester General Hospital Rochester, NY linda. greene@rochestergeneral. org
Declarations Nothing to Declare
Objectives Describe the epidemiology and pathogenesis of ventilator associated pneumonia Compare and contrast the current definition of ventilator associated pneumonia with the proposed revised definition List at least 3 evidence based practices to preventilator associated pneumonia. Discuss future trends and strategies in prevention ventilator associated pneumonia
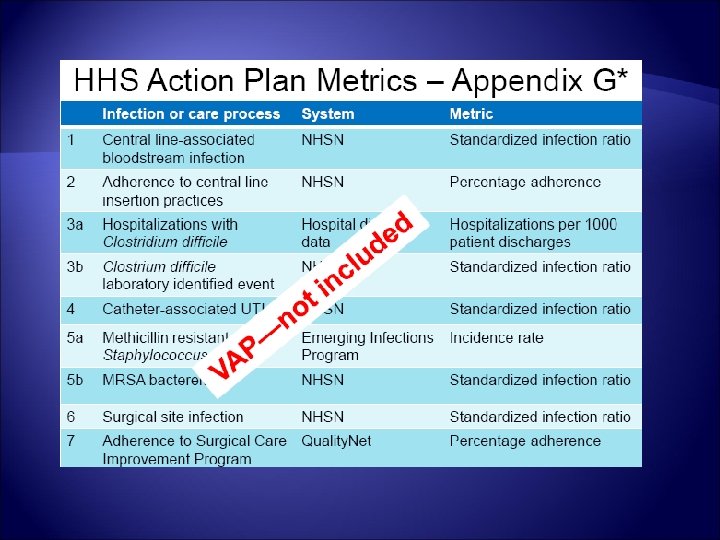
History of VAP tracking
Remember When
Early Work On VAP Prevention
What’s all the fuss about? GAO Report on HAIs in hospitals April 2008
GAO Report on HAIs in hospitals April 2008 Leadership needed from HHS to prioritize preventive practices Improve central coordination Identify priorities Increase reliable estimates of HAIs
The Era of Public Reporting
The Problem
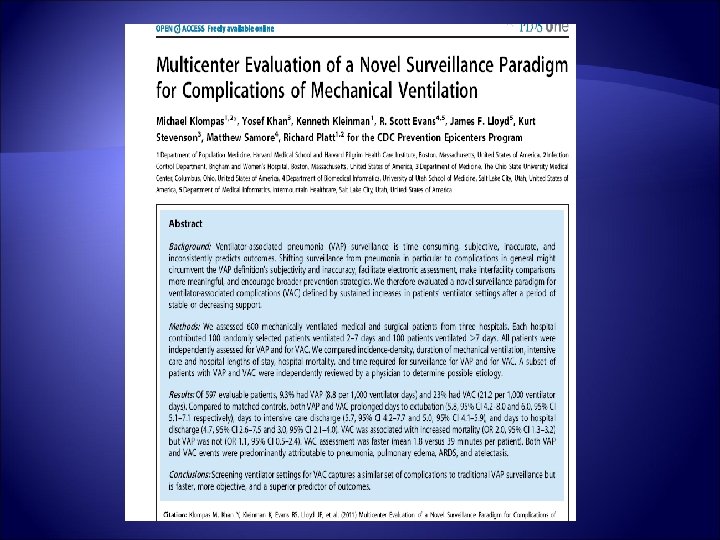
More Importantly The literature supporting high-profile measures to reduce ventilator-associated pneumonia (VAP): Many studies show significant reductions in VAP rates but almost none show any impact on patients' duration of mechanical ventilation, length of stay in the intensive care unit and hospital, or mortalit. Y Klompas M, Platt R. Ventilator-associated pneumonia – the wrong quality measure for benchmarking. Ann Intern Med. 2007; 147: 803 -805
Other Issues Lack of specificity in the VAP definition Array of events from critical to benign Benign events may actually capture colonization
Difficulty in applying the VAP definition consistently Pleural effusion or atelectasis however, pneumonia cannot be rule out Opacities in lower lobe may be atalectasis, pneumonia or emphysematous changes Bibasilar changes which may represent atelectasis , pneumonia or edema
Other Problems Differences in NYS among IPs collecting data Must be vetted with Physicians Start with sputum specimen Daily rounding Daily review of CXR Determination by ICU Staff
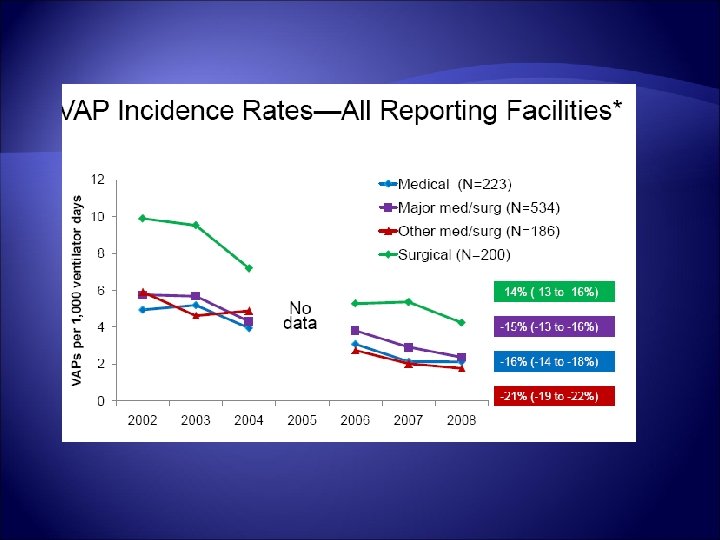
Possible Reasons for Decreases Prevention Strategies Bundles Burden on IP – less time for surveillance
Current Status Pressure to have a VAP outcome measure for public reporting
Where do we go from here Stakeholder meetings VAP working group Objective Definition Clinically relevant
VAP Working Group Representation from all major stakeholder groups: CDC IDSA CSTE APIC SHEA ATS Critical Care Society
What’s In a name? VAP Valori s. VAP VAC
Epidemiology Mechanical ventilation is primary risk factor: The endotrachel tube acts as a conduit from the upper respiratory tract to the lower respiratory tract Secretions collect on and around the cuff causing leakage of fluids into the lower respiratory tract Sedation inhibits the natural ability to clear secretions Patients undergoing mechanical ventilation are frequently fed via nasogastric tubes contributing to aspiration Critically ill patients are often maintained in a supine position Activity is limited
The Endotracheal Tube related issues primarily include aspiration of contaminated secretions from above the cuff Cuffs: current recommendation is that cuff pressure should be maintained at no less than 20 cm H 2 O Some controversy that cuff design may be more important Than cuff pressure
Host Defenses Location Defense Mechanism Upper Airway Nasopharynx Nasal Hairs Turbinates Upper airway anatomy Mucociliary apparatus Ig. A secretions Oropharynx Saliva Sloughing of epithelial cells Bacterial Interference Complement Production
Host Defenses Continued Location Defense Mechanism Conducting Airways Trachea, Brochii Coughing, epiglottic reflexes Airway branching Mucocillary apparatus Immunoglobulin production Airway Surface Liquid Lower Airways Terminal airways Alveoli Alveolar lining fluid Cytokines Alveolar Macrophages Polymorohonuclear Leukocytes Cell- mediated Immunity
What about Prevention Efforts?
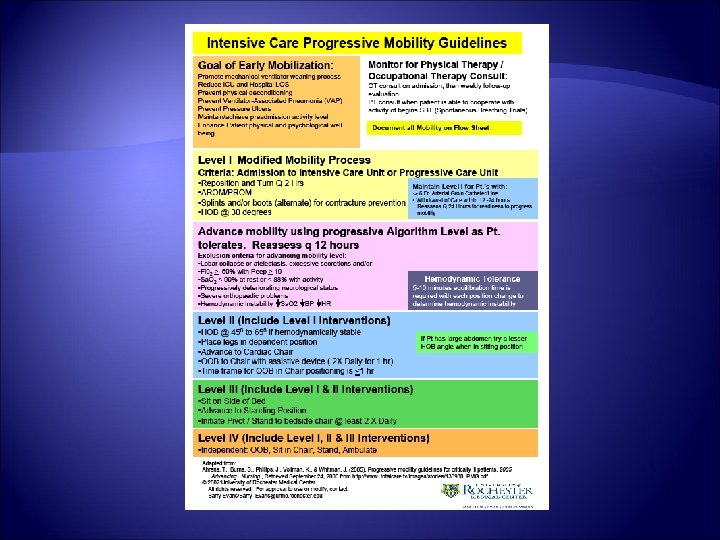
HOB elevated at least 30 degrees at all times If unable to bend at the hip use Reverse Trendelenberg
Head of Bed Monitoring Head of bed elevation: controversial, hard to maintain, but still recommended by most authors. Must be at least 30 degrees, and must measure, not estimate
Early tracheostomy Reduced VAP incidence in some studies but not others, does not hold up in metanalysis Probably good for reducing length of ventilation and ICU stay though
Mouth care Not part of original bundle Chlorohexidine recommended in increasing number of studies: Oral Decontamination with Chlorhexidine Reduces the Incidence of Ventilator-associated Pneumonia Koehman et al. American Journal of Respiratory and Critical Care Medicine Vol 173. pp. 1348 -1355, (2006) © 2006 American Thoracic Society
Chlorohexidine Oral decontamination for prevention of pneumonia in mechanically ventilated adults: systematic review and meta-analysis. Chan et. Al BMJ 2007, 334: 889. Randomized Controlled Trial and Meta-analysis of Oral Decontamination with 2% Chlorhexidine Solution for the Prevention of Ventilator-Associated Pneumonia Tantipong et L infection control and hospital epidemiology february 2008, vol. 29, no. 2
No benefit Effect of oral hygiene with o. 12% chlorohexidine gluconate on the Incidence of Nosocomial Pneumonia in children undergoing cardiac surgery Jacomo et al. ICHE et al. June 2011 vol 3 no 6
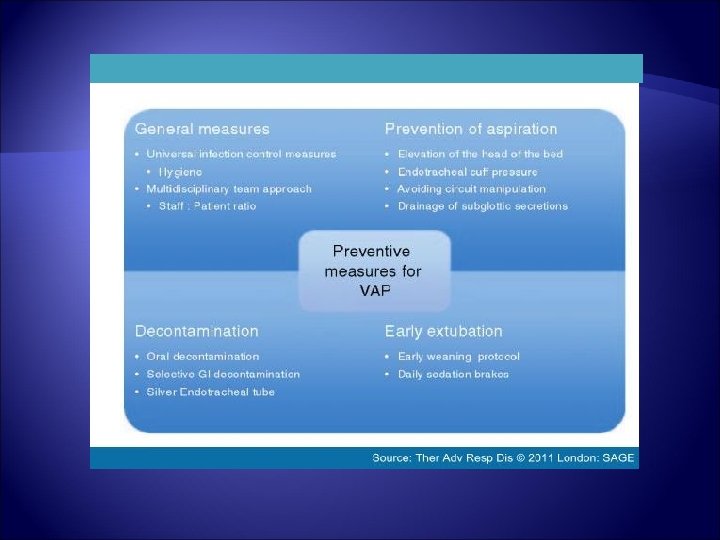
Bundle Elements The Basic Bundle HOB Monitoring Sedation Vacation PUD Prophylaxis DVT prophylaxis Enhanced Bundle Mouth Care- consider chlorohexidine Education and Training Program New Generation ET tubes Oral gastric tubes Ambulation
Silver or antimicrobial coated Tubes. Antimicrobial coating of ET tubes e. g. , silver coating, silver-sulfadiazene, chlorhexidine- recommended by some Rationale BIOFILM - Once microorganisms have made contact and formed an attachment with a living host or non-living surface or object, development of a biofilm can take place. Bacteria living in a biofilm can have significantly different properties from free-floating bacteria, as the dense extracellular matrix of biofilm and the outer layer of cells may protect the bacteria from antibiotics and normal host defense mechanisms of the white blood cells, such as phagocytosis
What are the most important prevention strategies? Avoid Intubation if possible -Non-invasive ventilation: avoiding intubation will avoid VAP, so use NIV whenever possible Weaning: the longer you are on the ventilator, the more likely you are to get VAP. Weaning protocols have been conclusively shown to improve the rate of weaning from the ventilator
What are the take home messages in trying to get there? Implementation Science – How do we get evidence to the bedside ? We have to take a closer look at processes
http: //www. cdc. gov/hicpac/pdf/Nov 12_13_HICPAC_web_slides. pdf
Engage Educate Evaluate Execute
Staff Education & Training!
staff feedback!
Sharing Data Months without a VAP 10 mo 1 mo
Other issues Look at other outcomes Mortality, readmission rates , length of stay Use data to continually evaluate effectiveness of interventions
Key Prevention Strategies v Communicate consistently: disseminate results of process and outcome measures. v Connect to purpose: help staff understand how simple actions connect to outcomes. v Review Deviations: review all cases to identify opportunities and system issues.
Working Together
http: //youtu. be/Pk 7 yql. TMvp 8