Venous Thromboembolism In Cancer Patients VTE Nabeel Rajeh

Venous Thromboembolism In Cancer Patients VTE Nabeel Rajeh, MD

VTE IN CANCER PATIENTS • First described by Trousseau 1865 • Hypercoagulability related to cancer • Procoagulant, vessel wall damage, stasis and immobilization, chemotherapy, surgery, radiation, • Underlying intrinsic hypercoagulability • Factor V leiden, antiphospholipid syndrome • 2 -6 fold increase in risk of

VENOUS THROMBOSIS IN CANCER PATIENTS FRONTLINE SURVEY • • • first comprehensive global survey of thrombosis and cancer 3, 891 completed responses were analyzed Brain and pancreatic tumors were a high risk for VTE 50% surgeons used thromboprophylaxis routinely 5% oncologists used thromboprophylaxis routinely Low molecular weight heparin (LMWH) was the most popular Aspirin for prophylaxis used in 20% • LMWH use by as initial treatment for VTE as outpatient followed by VKA • The results of the FRONTLINE survey demonstrate a need for guidelines to direct clinical practice in line with evidencebased data concerning cancer and VTE

Risk may be 1 -35%
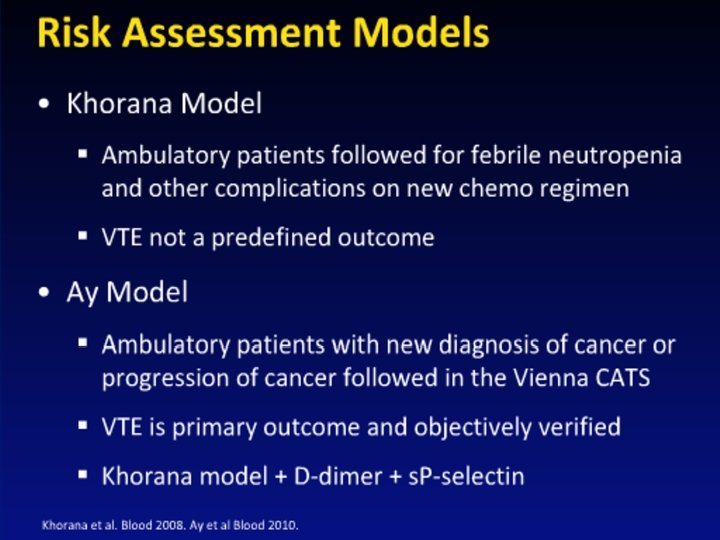
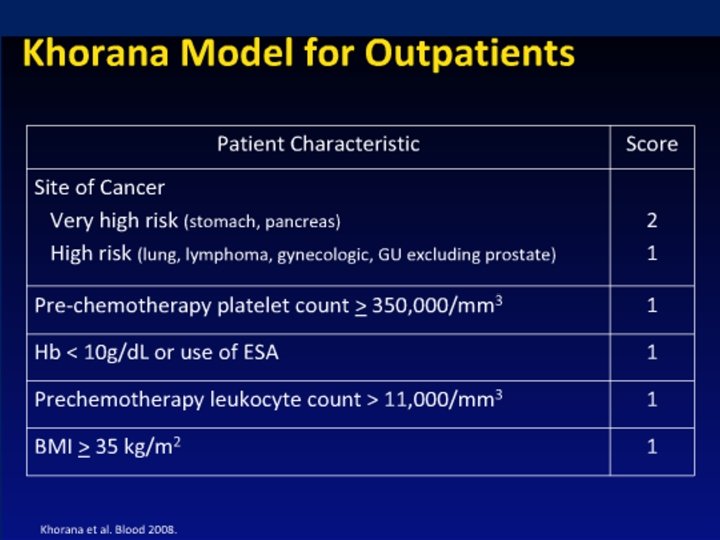
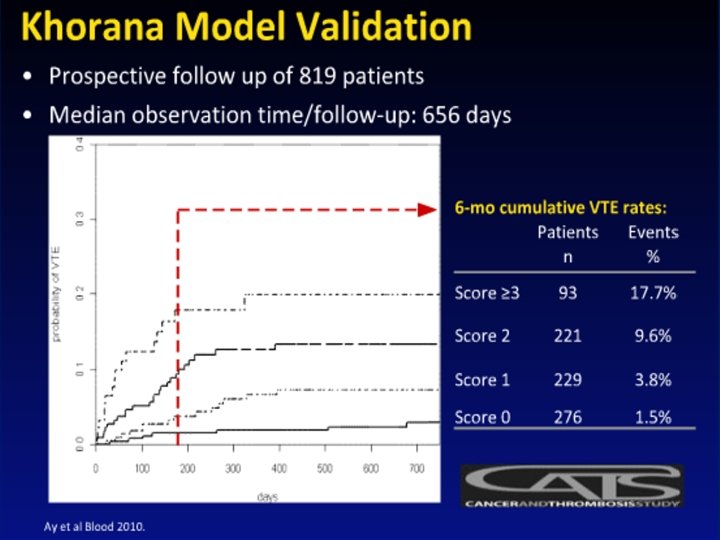
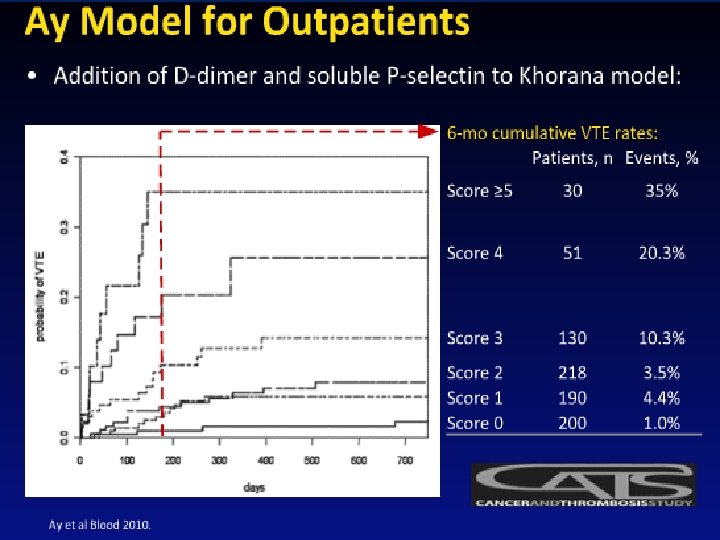

PREDICTORS OF VTE IN CANCER • Anemia , Leukocytosis, Thrombocytosis • History of VTE • Hospitalization • Infections • Immobilization • D-Dimer and P- Selectin

PREDICTORS OF VTE IN CANCER • Adenoca compared to squamous cell ca • Solid tumors as well as liquid tumors • Certain treatment • Thalidomid, lenalidomide, doxorubicin, tamoxifen, oral contraceptive, Dexamethasone erythropoietin, Bevacizumab

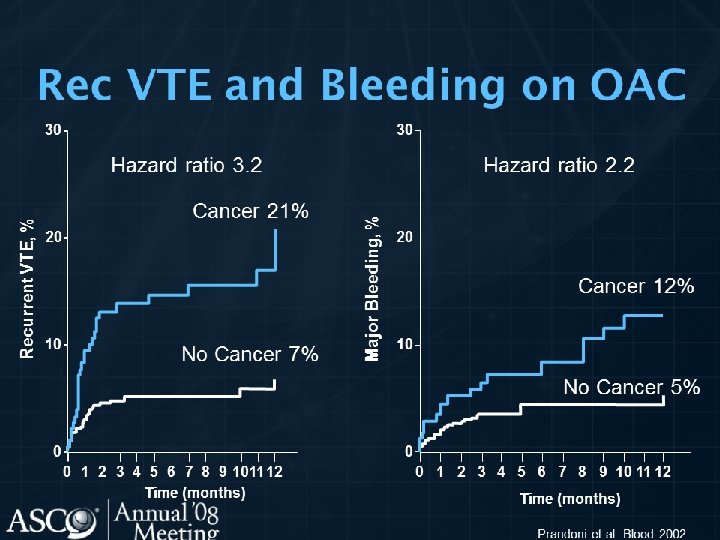
WHY CANCER PATIENT • Patient with solid tumor and distant metastases has 20 fold increase VTE • VTE second leading cause of cancer deaths • Risk of bleeding is 13% compared with 4% in none cancer • Significant early mortality if VTE

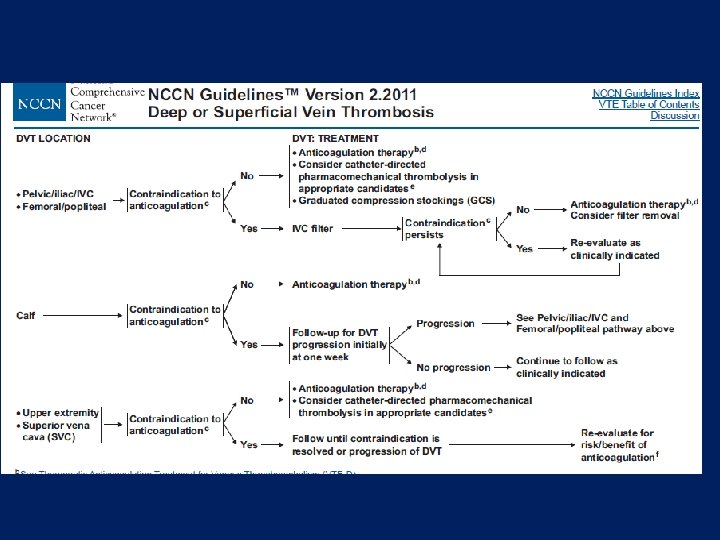
DIAGNOSIS OF VTE • Clinical prediction of risk • Symptoms and signs • D-Dimer testing to diagnose VTE is not recommended • Duplex venous ultrasonography with compressibility and flow • Indirect CT Venography • MRI • CTA for PE • Invasive venography may be outdated

SUPERFICIAL VEIN THROMBOSIS • Clinical diagnosis • Must rule out DVT • Trouseau Syndrome migratory SVT require UFH, or LMWH • Treatment with 4 weeks LMWH if central catheter related • NSAID

LMWH • Dalteparin, Enoxaparin, Tinzaparin • All inhibit Xa • Therapeutically equivalent and Interchangeable • RCT Tinzaparin compared to Dalteparin prove equality • Immediate therapy and prophylaxis is FDA • Continuation therapy require dose reduction? • Concern in renal, obese, elderly, HIT,

FONDAPARINUX • Specific Xa inhibitor • No cross reaction with HIT • Value in renal failure, obese, underweight, elderly is questionable • Dosing once daily

UNFRACTIONATED HEPARIN • • • Do we remember! SQ prophylaxis may be better than LMWH Bid or tid dosing Treatment based on weight 80 u/kg/h Can be used with renal failure (liver metabolism) • Risk of HIT • Resistance

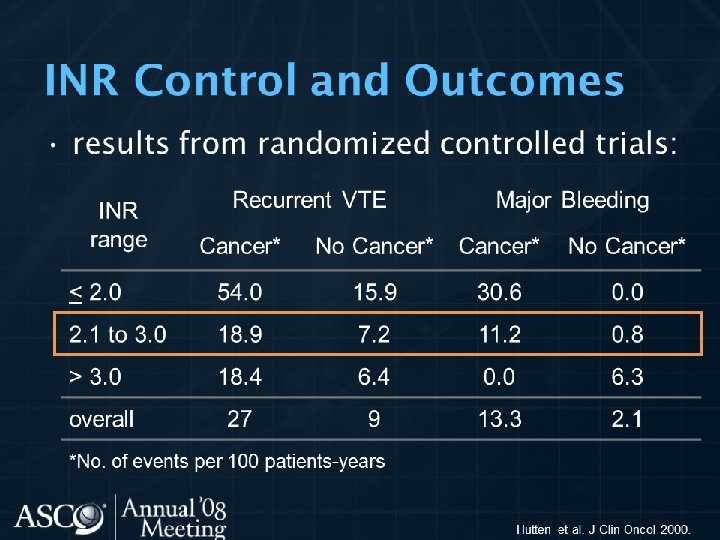
WARFARIN • The advisable chronic therapy • Concomitant with UFH or LMWH for 5 days • PT INR monitoring • Labile INR result • Resistance to therapeutic INR (genetically interaction and none compliance)

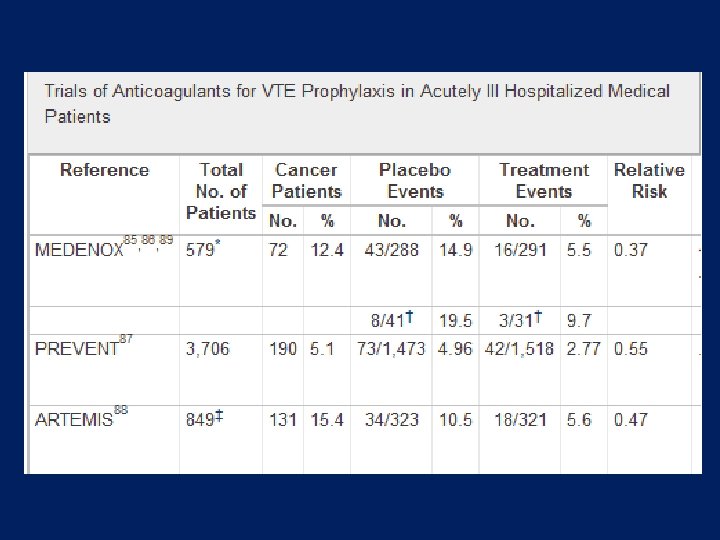
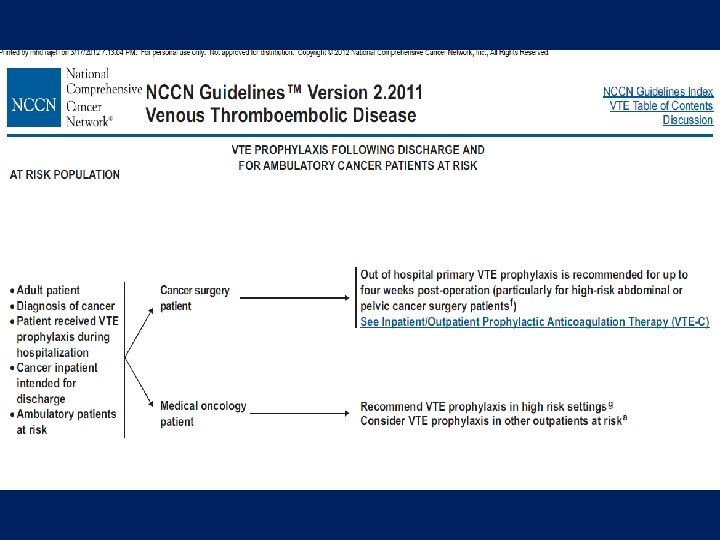
INPATIENT PROPHYLACTIC THERAPY • To all patients hospitalized with active cancer • Or suspicious cancer • Encourage ambulation although it is not enough prophylaxis • LMWH, UFH, Fondaparinux are effective • Low dose warfarin and adjusted to INR 1. 5 -2 for port catheter or chemotherapy catheter are not recommended • May extend for 4 week post discharge in very high risk patient

PROPHYLAXIS • SHOULD AMBULATORY PATIENTS WITH CANCER RECEIVE ANTICOAGULATION FOR VTE PROPHYLAXIS DURING SYSTEMIC CHEMOTHERAPY • Not at this time

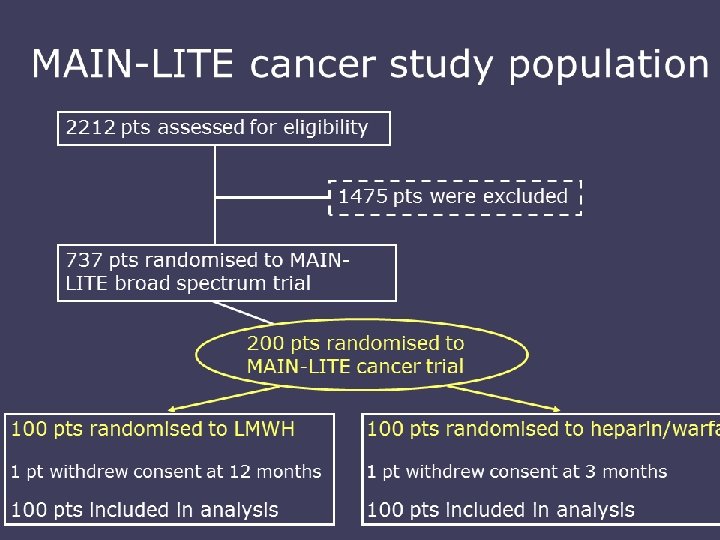
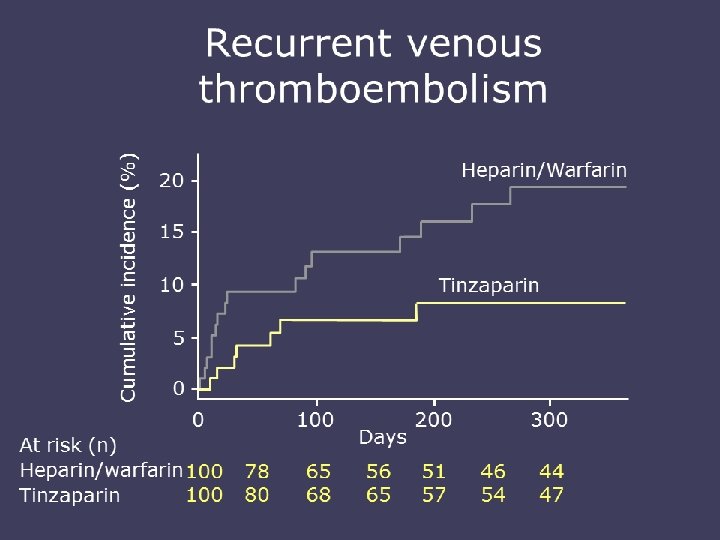
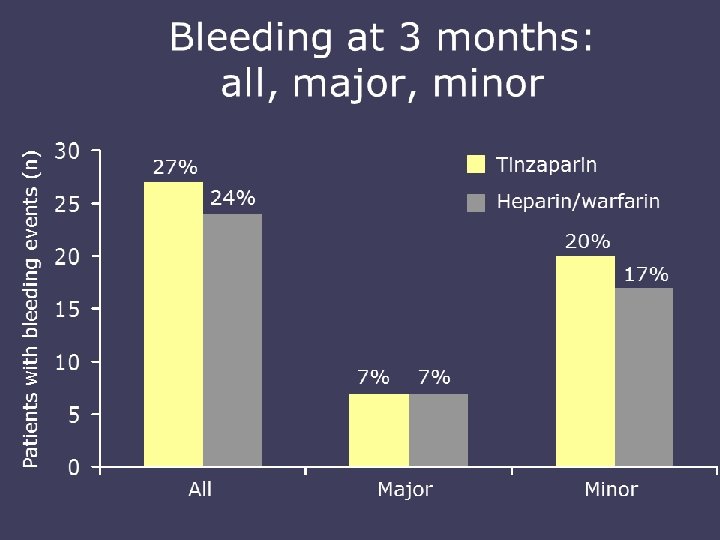
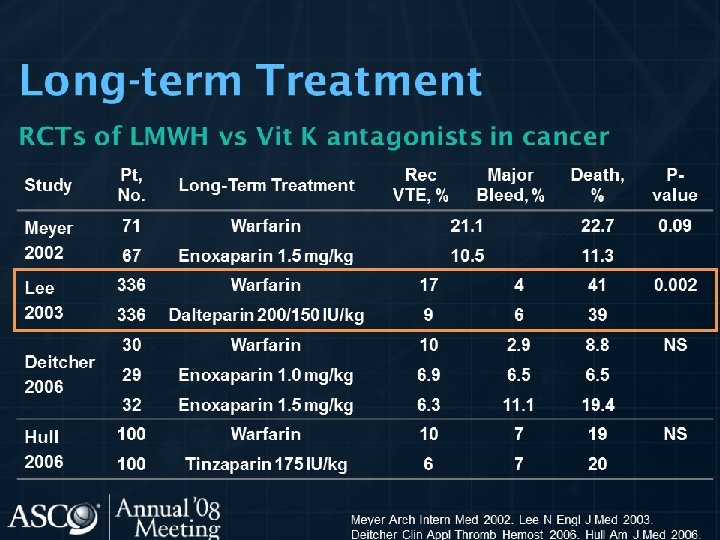
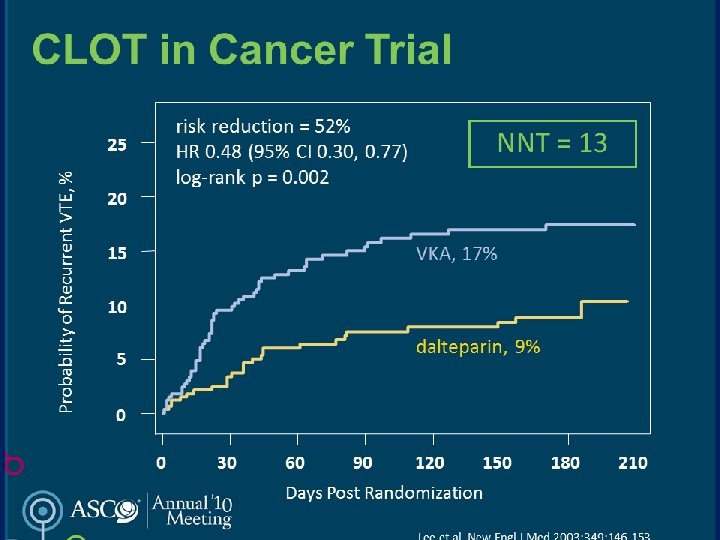
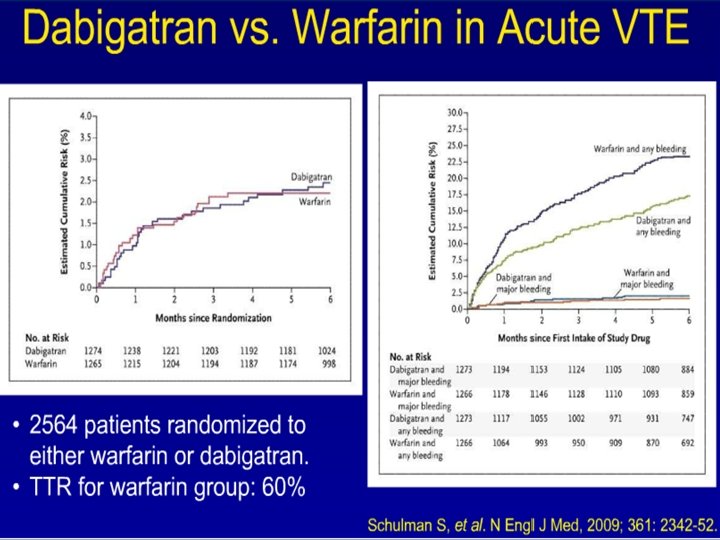
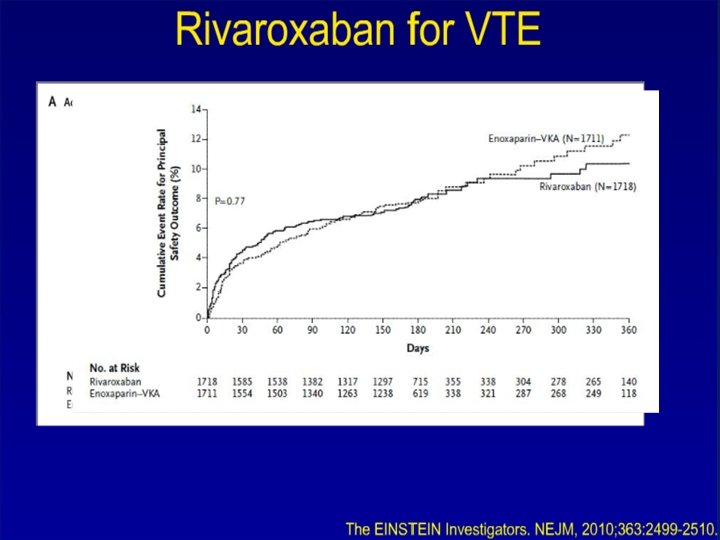
TREATMENT OF VTE • Immediate LMWH, UFH, Fondaparinux for 5 -10 days • Followed by LMWH for 6 m in patient with active cancer • LMWH beyond 6 m is not recommended • Warfarin with close monitoring • Meta-analysis LMWH reduce 3 m mortality comapred to UFH • Recurrence VTE and major bleeding are higher with chronic warfarin compared to LMWH

WHAT IS THE BEST TREATMENT FOR PATIENTS WITH CANCER WITH ESTABLISHED VTE TO PREVENT RECURRENT VTE? • LMWH is the preferred approach for the initial 5 to 10 days of anticoagulant treatment of the cancer patient with established VTE. • LMWH given for at least 6 months is also the preferred approach for longterm anticoagulant therapy. Vitamin K antagonists with a targeted INR of 2 to 3 are acceptable for long-term therapy when LMWH is not available
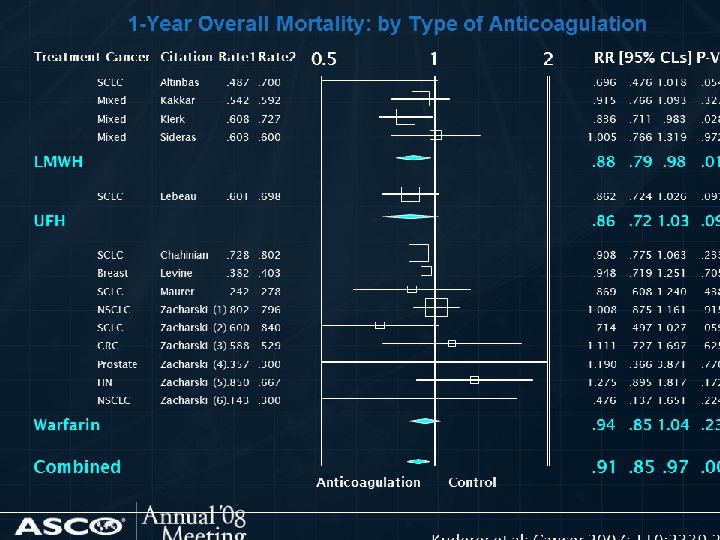

SHOULD PATIENTS WITH CANCER RECEIVE ANTICOAGULANTS IN THE ABSENCE OF ESTABLISHED VTE TO IMPROVE SURVIVAL? • Anticoagulants are not recommended to improve survival in patients with cancer without VTE.

HEPARIN INDUCED THROMBOCYTOPENIA

HIT • Thrombocytopenia Timeing, Thrombosis, o. Thers • PF 4/antibodies detection and serotonin release assay • Stop warfarin stop heparin no platelets • Direct thrombin inhibitors lepirudin argatroban • Fondaparinux

Thank You Nabeel Rajeh, MD www. syriaoncology. com
- Slides: 42