VENOUS INTERVENTIONS IN MENIERES DISEASE ALDO BRUNO MD
 ITALY")
VENOUS INTERVENTIONS IN MENIERE’S DISEASE ALDO BRUNO MD GEPOS CLINIC Telese T. (BN) ITALY

Disclosure Statement of Financial Interest I, Aldo Bruno DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation.

Menière P. : Maladies de l’oreille interne offrant des symptomes de la congestion cerebral apoplectiforme. Gaz Med de Paris. 1861; 16: 88. …if a serious hypacusia happens, then the cause of the vertigo is in the Labyrinth Prospero Menière, 1861 He also was the first to recognise that the function of equilibrium was in the inner ear

Committee on Hearing and Equilibrium guidelines for the diagnosis and therapy in Meniere’s disease AAO 1995 Meniere’s disease is a clinical disorder defined as the idiopathic syndrome of endolymphatic hydrops. … endolymphatic hydrops can only be demonstrated with certainly by histopatholocic study of the temporal bones. … The presence of endolymphatic hydrops can be inferred during life by the presence of the following as further defined below: Recurrent, spontaneous episodic vertigo; Hearing loss; aural fullness; tinnitus. Either tinnitus or aural fullness (or both) must be present on the affected side to make diagnosis for reporting purpose under these guidelines

Journal of Vestibular Research, 2015, 25, 17 ➢ The Classification Committee of the Bárány Society ➢ The Japan Society for Equilibrium Research ➢ The European Academy of Otology and Neurotology (EAONO) ➢ The Equilibrium Committee of the American Academy of Otolaryngology. Head and Neck Surgery (AAO-HNS) ➢ The Korean. Balance Society

Physiopatology of Meniere Disease • Genetic Predisposition • Autoimmunity Hydrops • Inflammation • Blockage of the drainage/increase production of endolinfa • ADH System- Aquaporine Cellular Modification ROS Deposit • Canalopaty of membrane Neuro e Citossicity • Headache Modification of the idroionic omeostasis • Neurovegetaive Modification Endococlear Potential Dizziness Hypoacusis Fullness • Viral Infection • Diet deficiency • Trauma Tinnitus

Epidemiology • Average of onset : 30 -40 years old • Rare in Childood (1 -2%) • There are no significant gender differences

Incidences of Meniere’s Disease The data available is often inconclusive hence not reliable Cases of Meniere’s Disease 200/1. 000 (Giappone, 1997) 75/1. 000 ( Francia) 101/1. 000 (USA) 460/1. 000 (Svezia) 350/ 1. 000 (UK) 43/1. 000 (Finlandia, 2000) 100/1. 000 (Italy)


THERAPY Currently there is no cure for Meniere’s Disease.

CCSVI Chronic Cerebro-Spinal Venous Insufficiency Vascular syndrome characterized by stenosis of the internal jugular veins and / or azygos veins, with opening of collaterals and insufficient cerebrospinal venous drainage Is it possible to hypothesize that CCSVI for congenital anatomical alteration or functional acquired alterations represents a predisposing factor for developing inner ear disorders like MD?

Vascular Findings in MD The stria vascularis plays an important role in the production and absorption of endolymph and consequently on the genesis of hydrops in MD. In literature many studies have been published concerning the vascularization of the stria and the inner ear vascular conditions.

Vascular findings in MD The stria vascularis are severely atrophic and degenerated in patients with MD. (Paparella et al. , 2007) The number of vessels in the stria vascularis in ears with MD are smaller than in normal controls in all cochlear turns. (Paparella et al. , 2009)

VENOUS DRAINAGE Internal auditory vein Vein of cochlear aqueduct Vein of vestibular aqueduct Superior petrosal sinus Inferior petrosal sinus Transverse sinus Sygmoid sinus Internal Jugular Vein

Friberg U, Rask-Andersen H. Vascular occlusion in the en- dolymphatic sac in Meniere’s disease. Ann Otol Rhinol Laryngol 2002; 111: 237– 245. The described specimens represent pathologic changes that occur after a prolonged disease. A thrombus may recanalize, lyse, prop- agate, or become organized; accordingly, a reverted flow can be temporary or chronic. In the cases reported here, the thrombus appeared as organized and hence indicates a longstanding process, which is consistent with MD for several years. In theory, repeated microthrombosis could reverse the flow over and cause fluctuating symptoms as seen in MD.
: 194 -8. A potential portal flow in the inner ear.")
Laryngoscope 2007 Feb; 117(2): 194 -8. A potential portal flow in the inner ear. Friis M, Qvortrup K. Source Department of Otolaryngology, Head and Neck Surgery, Unviersity of Copenhagen, Rigshospitalet, Copenhagen, Denmark. morten_friis@hotmail. com Abstract Objectives/Hypothesis: The aim of the present study was to visualize the flow direction of blood in the extraosseous part of the vein of the vestibular aqueduct (VVA) and to explore the effect of an induced obstruction in the distal part of the VVA before it merges with the sigmoid sinus. The endolymphatic sac has been implicated as a potential endocrine gland, which venules drain to the VVA. A reversal of the direction of flow in the VVA toward the inner ear could, through vestibular arteriovenous anastomosis, cause portal circulation in the inner ear. Study Design: The authors conducted an experimental animal study using in vivo fluorescence microscopy. Results: Obstructing the distal part of the VVA just before it empties into the sigmoid sinus immediately reverses the flow of blood in the VVA toward the inner ear. Conclusions: After an obstruction of the VVA, the drained venous blood from the endolymphatic sac may enter a portal circulation in the inner ear, which could cause disturbances in the endolymph homeostasis and potentially symptoms as seen in Meniere disease

Conclusions: After an obstruction of the VVA, the drained venous blood from the endolymphatic sac may enter a portal circulation in the inner ear, which could cause disturbances in the endolymph homeostasis and potentially symptoms as seen in Meniere disease

Our group worked either on diagnosis and on therapy of CCSVI in MD Benevento: A. O Rummo Audiology Department. Rome: Sapienza University, ENT Department, Bologna: Maggiore Hospital, ENT Department ITALY

Our group are working on diagnosis and therapy of Diagnosis and therapy of CCSVI in Meniere’s Disease ECD, MRI, PTA Clinica Gepos: Vascular Department Neuroradiology Department (Telese Terme Italy)

Ethics The experimental study was approved by the local authority and was in accordance with the guiding principles in the care

• ALL PATIENTS ENROLLED IN THIS STUDY WERE ALREADY IN TREATMENT AT REFERRED ENT DEPARTMENTS AND UNDERWENT ONLY SYNTHOMATIC THERAPY. • SOME OF THEM HAD INTRATHIMPANIC INJECTION OR SURGICAL TREATMENT FOR SYMPTHOMS OF MENIERE DISEASE HOWEVER, NO PATIENTS EXPERIENCED NOTABLE IMPROVEMENT

Neck veins to be examined within the CCSVI Examination Protocol IJVs – Internal Jugular Veins (examined side Left and Right both sitting 90° and supine 0° position) VVs – Vertebral Veins (examined side Left and Right both sitting 90° and supine 0° position)

ECD-TCCS PARAMETERS 1. Bidirectional flow in one or both the IGV and / or the VV in both positions or bi-directional flow in one position with absence of flow in the other (65%) 2. Bidirectional flow in the intracranial veins and sinuses (80%). 3. Intraluminal defects (flaps, septa or valves) associated with hemodynamic changes (blocks, reflux or acceleration) and / or re duction of the area of the IGV in the supine position to 0. 3 cm /sq (90%) 4. Absence of flow in the IGV and / or VV and / or absence of flow in one position and bidirectional flow in the other (45%) 5. IGV DCSA increased or unchanged both at 90 ° to 0 °(3%)

Gadda G, Taibi A, Sisini F, Gambaccini M. , Zamboni P. , Ursino M. : A NEW HEMODYNAMIC MODEL FOR THE STUDY OF CEREBRAL VENOUS OUTFLOW Am. J. Physiol Heart Circ. Physiol 2015 Feb 1; 308(3): H 217 -31

MATERIAL and METHOD 2013 -2016 • 312 PATIENTS WITH DEFINITE MENIERE’S DISEASE • 123 MEN AND 189 WOMEN • Age 58 +/- 18. 3 years Definite Meniere's disease 102 healthy subjects 48 men and 54 women Age 49. 3 +/- 7. 8 • Two or more definitive spontaneous episodes of vertigo 20 minutes or longer • Audiometrically documented hearing loss on at least one occasion • Tinnitus or aural fullness in the treated ear • Other cases excluded
 • 12/102")
CCSVI POSITIVITY in definite Meniere's disease • 277/312 PATIENTS WITH MD (89%) • 12/102 HEALTHY SUBJECTS (12%)

Acta Oto-Laryngologica Chronic cerebrospinal venous insufficiency as a cause of inner ear diseases Giuseppe Attanasio, Laura Cagnoni, Eleonora Masci, Francesco Ciciarello, Francesco Diaferia, Aldo Bruno, Antonio Greco & Marco De Vincentis Pub Online Nov. 2016

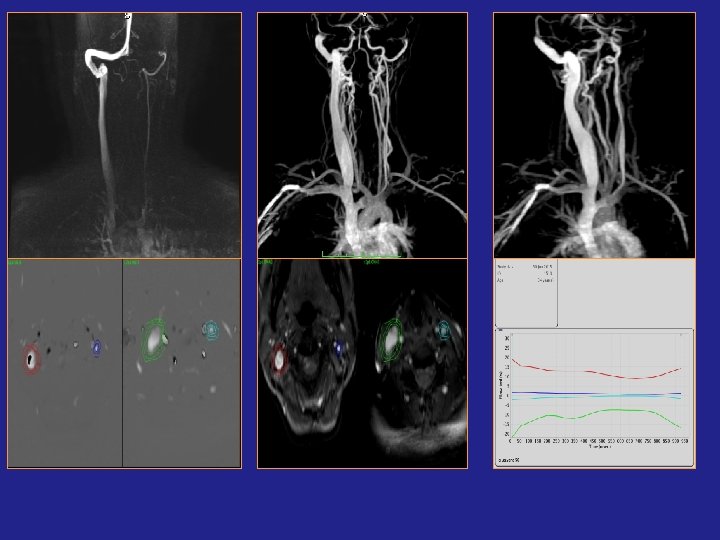
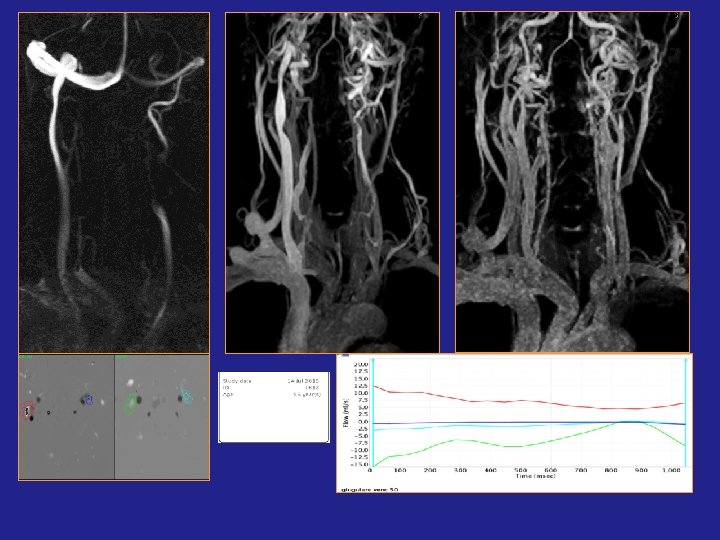
ANGIO-MRI and CCSVI

Work in progress
")
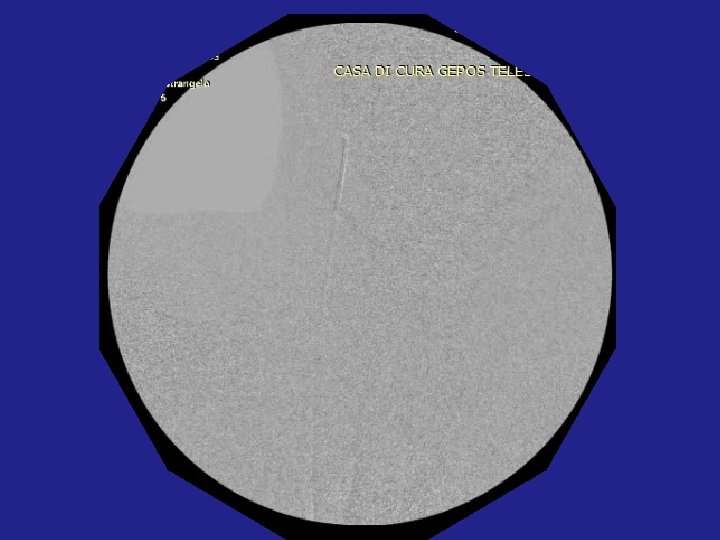
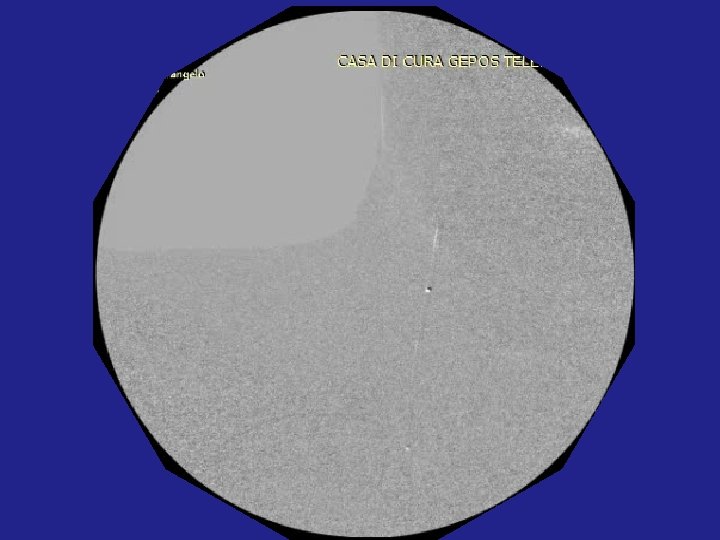
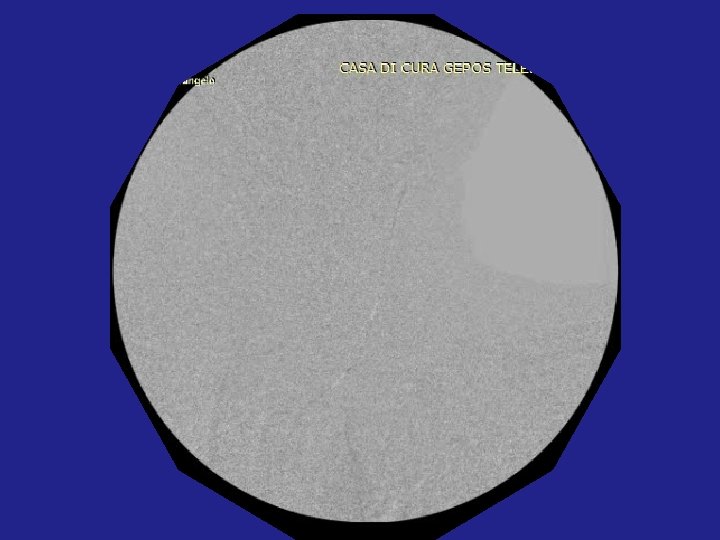
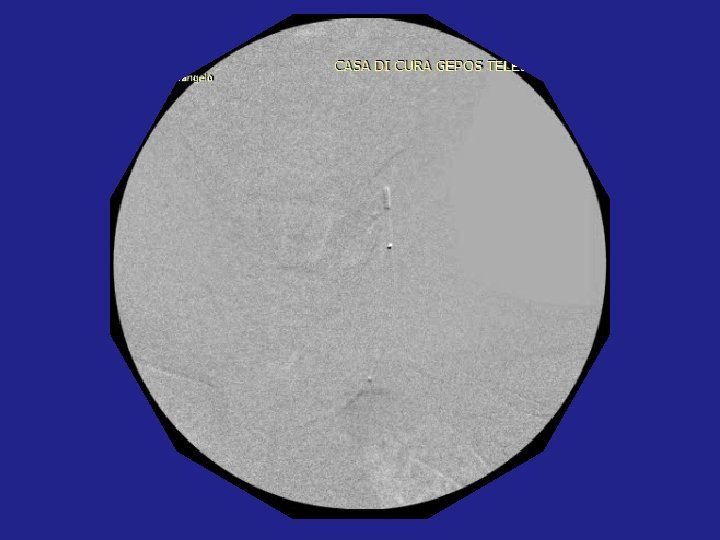
PTA FOR CCSVI: Personal protocol Local anesthesia Percutaneous trans-femoral venous catheterization (sn / dx) Cavography (Lower and Upper) Selective catheterization of the internal jugular veins and of the azygos vein Selective venography in the three projections and assessment of the empty time Sodium heparin 2500 IU PTA balloon noncompliant with Ø 10 -20 mm (routine Ø 14 -16 mm) for IGV and 8 -12 for AV control angiography Manual compression for hemostasis Compressive dressing (no need for percutaneous systems of hemostasis) Bed rest with leg extended for 12 hours Post-operative therapy: LMWH 6000 IU x 20 days Mesoglycan therapy: 100 mg / day for 12 -24 months Clinical monitoring and echocolordoppler at 1, 3, 6, 12, 15, 18, 24 months

The main criteria adopted to define stenosis of the IJV or AV with venography was: • At least 50% stenosis of the vein compared with the diameter of an adjacent segment of the vein. • Emptying time of over 6 seconds in all vein projections. • Intraluminal abnormalities (web, septa, valvular ). • Collateral veins with a faster emptying time compared with IJV or AV.
 stenosis of both proximal segments of the Azygos vein and the")
Type A (4%) stenosis of both proximal segments of the Azygos vein and the IJV with a contralateral IJV size increased (> cross-sectional area) Type B (35%)hemodynamically significant stenosis of both IJV and proximal Azygos Vein Type C (60%) bilateral stenosis of the IJV with normal azygos Type D (1%) multiple azygos and lumbar system lesions. In Meniere’s Disease I have observed mainly Type C and Type B of CCSVI The collateral circulations that occur most frequently are those of the condylar system, pterygoid plexus and thyroid veins


Post-operative therapy: • LMWH 6000 IU x 20 days • Mesoglycan therapy: 100 mg / day for 12 -24 months • Clinical monitoring by ENT and echocolordoppler at 1, 3, 6, 12, 15, 18, 24 months, • Dosage: Vit. B 12 , Folic Acid, Vit. D, Homocysteine
 From April 2013 to December")
OUR CLINICAL SERIES Vascular Surgeon: Aldo BRUNO, Benevento (Italy) From April 2013 to December 2016 N. 105 PROCEDURES - 53 Male - 52 Female Age: average 47 years. Unilateral Meniere’s Disease : 70 cases Bilateral Meniere's disease: 35 cases Onset of the disease from 28 years to 2 years before All patients with positivity for two/five parameters according to Zamboni Protocol for CCSVI
 Major complications: 0% (DVT,")
RESULTS Angiographic success v / s Intention-To-Treat: 103/105 (98. 5%) Major complications: 0% (DVT, rupture, hemorrhage) Minor complications: five patients 5% (Fibrosis IGV by sonography after one month and one case of inguinal hematoma) Unchanged: 6% (Seven Patients) Secondary Clinical deterioration : Nine Patients (9%) Restenosis: Twelve Patients (Doppler ultrasound each three months after PTA): 11%, Six of which had a secondary clinical deterioration

Results on Meniere's disease symptoms ONLY BY ENT EVALUTATION

In 3 -6 -12 month post PTA follow-up we have observed Improved hearing, reduction or disappearance of tinnitus, disappearance or reduction of dizziness, decreased sensation of fullness in about 80% of cases, improvement of QOL But: • in a short time follow up the placebo effect could act on results • AAO 1995 -2015 guidelines recommended the evaluation of therapy after a 24 month follow up

Article Published February 2017 J. V. I. R. The Prevalence of Chronic Cerebrospinal Venous Insufficiency in Meniere Disease: 24 -Month Follow-up after Angioplasty Aldo Bruno, MD, Marisanta Napolitano, MD, Ph. D, Luigi Califano, MD, Giuseppe Attanasio, MD, Vincenzo Giugliano, MD, Pier Paolo Cavazzuti, MD, Marika Viccaro, MD, Eleonora Masci, MD, Diego Mastrangelo, MD, Francesca Salafia, MD, Salvatore Mazzone, MD, Benedetto Bernardo, MD, Laura Cagnoni, MD, Roberto Filipo, MD, Ph. D, Marco De Vincentis, MD, Antonio Greco Ph. D ,
 From April 2013 to December")
OUR CLINICAL SERIES Vascular Surgeon: Aldo BRUNO, Benevento (Italy) From April 2013 to December 2015 N. 69 PROCEDURES - 32 Male - 37 Female Age: average 47 years. Unilateral Meniere’s Disease : 45 cases Bilateral Meniere's disease: 24 cases Onset of the disease from 28 years to 2 years before All patients with positivity for two/five parameters for CCSVI

24 MONTH FOLLOW-UP Expected benefits on MD symptoms were: • Improvement of hearing • Reduction of the number and degree of spells of vertigo. • Reduction of tinnitus and fullness • Improvement of Quality of Life, measured by DHI
 Side 40 16(40%)")
24 MONTH FOLLOW-UP patients Male Female Mean duration of MD (months) Side 40 16(40%) 24 (60%) 74 R: 12 } 70% L: 16 Bil: 12 (30%)
* * In")
HEARING LOSS PTA 0. 5 -3 k. Hz Improved (>10 d. B)* * In 5/10 Patients 25 -40 d. B 20 (50%) Unchanged (± 10 d. B) 16 (40%) Worsened (>10 d. B) 4 (10%) Pure Tone Average is considered improved / worsened if a 10 d. B difference is noted Committee on Hearing and Equilibrium AAO-HNS , 1995 Pre- Angioplasty Pure Tone Average: 60. 09 d. B Post- Angioplasty Pure Tone Average: 50. 55 d. B P=0. 0031 In 10/20 patients improvement was 25 -40 d. B
 Vertigo spells Avg spells/month pre-treatment (6 mon recommended)")
Avg spells/month post-treatment (24 mon recommended) Vertigo spells Avg spells/month pre-treatment (6 mon recommended) x 100 = Control Level AAO-HNS CHE, 1995 AVG/month pre ± SD 11. 9± 14. 3 AVG/month post±SD 0. 97± 1. 3 A 0 = complete control B 1 -40 = substantial control C 41 -80 = limited control D 81 -120 = insignificant control E > 120 = worse F Secondary treatment required due to disabling vertigo Control level N° Patients % A B C D E F 22 12 2 0 2 2 55% 30% 5% 5% 5% 34 (85%) 6 (15%)

TINNITUS AND FULLNESS: a «brute» subjective evaluation TINNITUS FULLNESS Disappeared 0 0 Improved 14 (35%) 52 (70%) Unchanged 22 (55%) 12 (30%) Worse 4 (10%) 0

Clinicians measure, patients feel What happened by a very simply patient-oriented assessment? Better or worse? This is the question Better 30/40 Unchanged 6/20 Worse 4/20

We can affirm that: ➢ CCSVI and MD are frequently associated conditions ➢ PTA procedure cures anatomic and functional CCSVI anomalies ➢ PTA procedure gives a good control of MD symptoms in a two year follow up We cannot affirm that: ➢ CCSVI is the major cause of MD ➢ PTA “cures” MD

The venous stasis of the head and neck veins may be considered a further etiopathogenetic mechanism which adds to many other already known mechanisms that define MD as a multifactorial disease


Research and Knowledge never ends. There are very few certainties to build on our weak knowledge
- Slides: 60