Venous Ablation Therapy When and How Keith M

Venous Ablation Therapy: When and How? Keith M Horton, MD Medstar Washington Hospital Center Clinical Assistant Professor Radiology, Georgetown University Hospital

Keith M. Horton, MD I/we have no real or apparent conflicts of interest to report. Off-Label: Foam Sclerotherapy: can be produced only with detergents: sodium tetradecyl sulfate (STS) which is FDA-approved as Sotradecol™, and polidocanol ( POL) which is not yet FDA-approved.

Journal of Vascular and Interventional Radiology, January 2010 Vol. 21, Issue 1, Pages 1431

U. S. Epidemiology and Prevalence Venous reflux disease is 2 x more prevalent than coronary heart disease (CHD) and 5 x more prevalent than peripheral arterial disease (PAD)1 Of the estimated 25 million people with symptomatic superficial venous reflux 1: – Only 1. 7 million seek treatment annually 2 – Over 23 million go untreated 1. 2. Sources: American Heart Association, SIR, Brand et al. “The Epidemiology of Varicose Veins: The Framingham Study” US Markets for Varicose Vein Treatment Devices 2006, Millennium Research Group 2005.

Prevalence by Age and Gender Age Female Male 20 - 29 8% 1% 40 - 49 41% 24% 60 - 69 72% 43% Coon WW, Willis PW, Keller JB: Venous thromboembolism and other venous disease in the Tecumseh Community Health Study Circulation 1973; 48: 839 -846.

Risk Factors Gender Age Heredity Pregnancy Standing occupation Obesity Prior injury or surgery Sedentary lifestyle http: //www. venarin. com/varicose-veins-treatment/varicose-vein-causes. htm

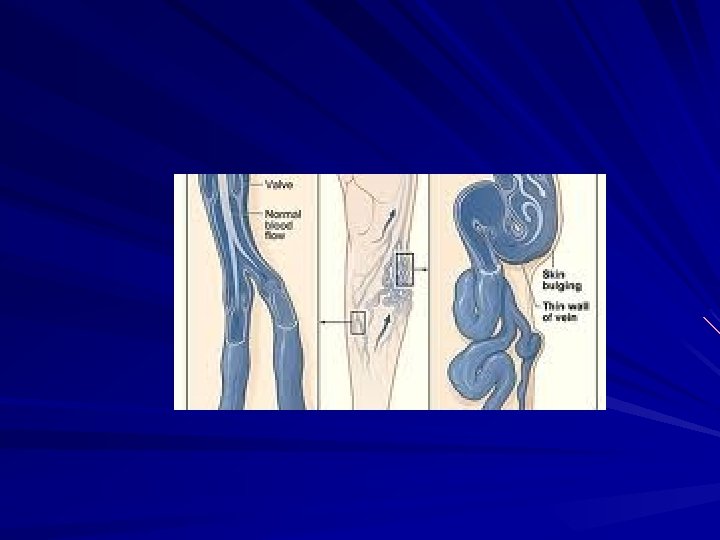
Vein Valves Blood propelled by calf muscle pump opens the valve in one direction Blood moving with gravity closes the normal valve Image source: http: //www. veininnovations. com/varicose_veins_faqs. html

Vein Valve Failure Normal vein: valve open and closed Dilated vein with nonfunctioning valve
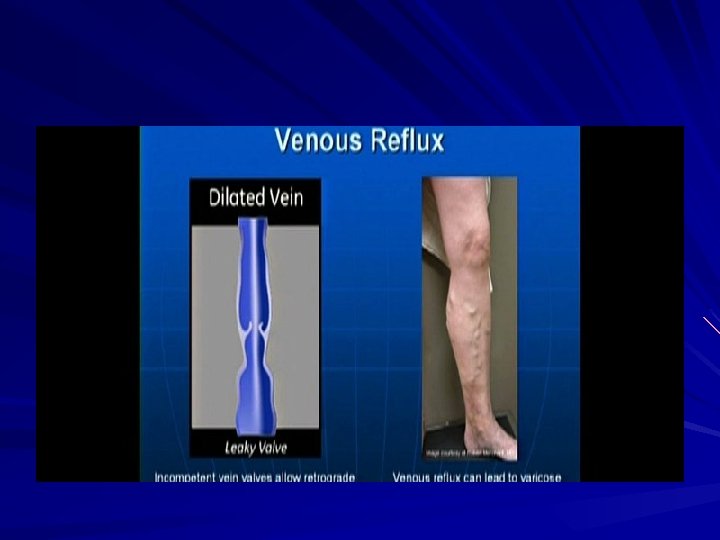

Venous Reflux: A Serious Progressive Disease Symptomatic Patients 1 Varicose Veins Leg Swelling 20 Million Skin Damage Skin Ulcers 2 -6 Million 500 K Increased pain and reduced quality of life 1 White JV, Ryjewski C. Chronic venous insufficiency. Perspect Vasc Surg Endovasc Ther 2005; 17: 319 -27 2 Image courtesy of Paul Mc. Neill, MD 3 Image courtesy of Rajabrata Sarkar, MD 4 Photo source: missinglink. ucsf. edu/. . . /stasis_dermatitis. html 5 Photo source: Amor Khachemoune, Catharine Lisa Kauffman: Management Of Leg Ulcers. The Internet Journal of Dermatology. 2002. Volume 1 Number 2.

Duplex Ultrasound § All patients should have Clinical and US § Must be familiar with Duplex US § Knowledge can be Acquired in many ways

The Great Saphenous Vein § GSV within the fascial envelope • Note the superficial or saphenous fascia above the vessel and the deep or muscular fascia below the vessel Images courtesy of Olivier Pichot, MD

Saphenofemoral Junction Image courtesy of Gerald Niedzwiecki, MD SFJ image source: Chandler JG et al. Defining the role of extended saphenofemoral junction ligation: A prospective comparative study. JVS 2000; 32: 941 -53

Superficial System Exam: Great Saphenous Vein Image courtesy of Gerald Niedzwiecki, MD Normal valve closure time of <0. 5 sec Image courtesy of Gerald Niedzwiecki, MD Reflux of approximately 1. 5 seconds

Reflux Assessment: Deep System Exam Assess deep venous system and rule out DVT using compression, color flow and augmentation Note areas of deep system incompetence at this time Image courtesy of Gerald Niedzwiecki, MD Vein in compression Normal flow in deep vein after augmentation

Treatment for Venous Insufficiency 1 First line is conservative management What patient can do – Exercise daily – Elevate legs often – Wear medical grade compression stockings 2 3 Image sources: 1: http: //medicalimages. allrefer. com/large/walking-for-health. jpg 2: http: //mikesbikes. com/images/library/site/stretching_after_15_ap_03. gif 3: www. vascularweb. org/_CONTRIBUTION_PAGES/Patient_Information/North. Point/Pulmonary_Embolism. html

Compression Therapy for Venous Insufficiency First step in management of SVI – Payors usually require several weeks or even months Doesn’t alter anatomy of venous insufficiency patient; treats symptoms but is not curative – Accelerates venous return – Compression reduces lumen diameter of superficial and deep veins – Helps calf muscle pump work more effectively Underlying cause must still be addressed Very useful in post-treatment regimens

Indications For Endovenous Procedure Failed conservative therapy Signs and symptoms of venous insufficiency – Impact of symptoms on ADLs often not realized until after problem corrected Reflux proven by duplex scan – Anatomic defect that will lead to worsening of natural history Should be corrected on its own merit

Traditional Therapy For SVI GSV stripping and ligation – Groin incision to ligate and divide GSV tributaries and SFJ at CFV – Stripper passed through GSV at groin, retrieved at knee incision – Stripper pulled from groin to knee, stripping vein and avulsing branches – Significant morbidity associated with vein avulsion Image source: Goldman MP, et al eds. Varicose veins and telangiectasias: Diagnosis and treatment. 2 nd ed. St. Louis: Quality Medical Publishing, Inc. ; 1999.

Modern Therapy For SVI Endovenous ablation – Radiofrequency or laser • Great and small saphenous veins • Accessory saphenous veins • Giacomini or Thigh Extension veins • Perforators

Radiofrequency Ablation RF generator heats catheter tip coil, which conducts heat into vein wall – Denudes intimal lining – Collagen molecules contract – Acute inflammatory response leads to eventual fibrotic occlusion of vessel Treatment temperature at 120 C – System uses least amount of energy necessary to maintain temperature – Continuous system feedback ensures adequate thermal dose

Endovenous Laser generator and generic diode laser fiber Peak treatment temperature reaches ~700 C – Heated blood in vein generates steam bubble which indirectly heats vein wall, causing thrombotic occlusion Image source: www. shh. org/program/evlt. asp

Anatomy GSV 70 -80% SSV 10 -20% Non Saph 10 -15%

Pre-op Mapping & Marking Significant anatomy to note: – – Depth of vein from skin surface Maximum vein diameter Duplicate saphenous system Areas with: Tortuous and aneurysmal segments Tributaries, branches and perforators – Potential vein access sites – Nitropaste Image courtesy of Joseph Smith, MD



Vein Access Treatment vein accessed percutaneously under ultrasound guidance or with small cut down Needle Image courtesy of Darcy Kessler, RVT

Vein Access § Vein access achieved percutaneously or through small cutdown § An introducer sheath is placed in vein Image courtesy of Joseph Smith, MD

Catheter Tip Position Catheter tip is positioned 2. 0 cm distal to the SFJ to – Avoid heating too close to deep venous system – Preserve epigastric vein patency Catheter SEV SFJ CFV Image courtesy of Thomas Proebstle, MD

Indexing and Treatment 1. Apply external compression and deliver energy to vein segment; two 20 -second RF cycles delivered at segment closest to SFJ 2. Withdraw catheter to next shaft marker, apply compression and deliver energy 3. Repeat withdrawal, compression and treatments until desired length treated Note: Aneurysmal segments and areas with large tributaries or perforators may benefit from two treatment cycles
 using duplex imaging")
Perivenous Tumescent Infiltration Dilute local anesthetic infiltrated into saphenous compartment (perivenously) using duplex imaging Perivenous infiltration technique: note 360 “halo” of fluid around vein

Tumescent Infiltration Catheter Image courtesy of Michael Vasquez, MD Note fluid encircling vein Dilute local anesthetic infiltrated around treatment vein under ultrasound imaging

Tip Position Verification § Catheter tip is positioned 2. 0 cm distal to SFJ under ultrasound guidance Image courtesy of Joseph Smith, MD

Compression and Exsanguination Just prior to treatment, vein is compressed around catheter using combination of: – Tumescent infiltration – Trendelenburg position – External compression

Radiofrequency Ablation Procedure Video

Post-Ablation US Follow-up Follow duplex performed w/in 72 hours – Rule out DVT – Assess vessel occlusion Periodic duplex follow up of the patient recommended

Post-Ablation Duplex Assessment • No flow present • Thickened vein walls Image courtesy of Michael Vasquez, MD

Summary Can’t underestimate the value of Duplex WHEN is much more important than HOW!!

Summary Anyone can drill a Well It’s where you drill it that makes the difference!!!
- Slides: 41