Velamentous Umbilical Cord Insertion Case 1 Pathology No

Velamentous Umbilical Cord Insertion • Case 1: Pathology No. 1594480 • 32 -year-old female • Case 2: Pathology No. 1601851 • 40 -year-old female

Pathology No. 1594480 l Placenta ¡ 17 x 3 cm in size, 567 gm in weight ¡ A retroplacental hematoma l 5 x 2. 2 x 0. 4 cm in size l Loosely adherent to basal plate, with focal hemorrhage into placenta parenchyma ¡ A subamniotic hematoma l 2. 5 cm ¡ Umbilical cord l Two segments, 22 cm and 11 cm in length l Velamentous insertion l The length of intramembranous vessel: 9 cm

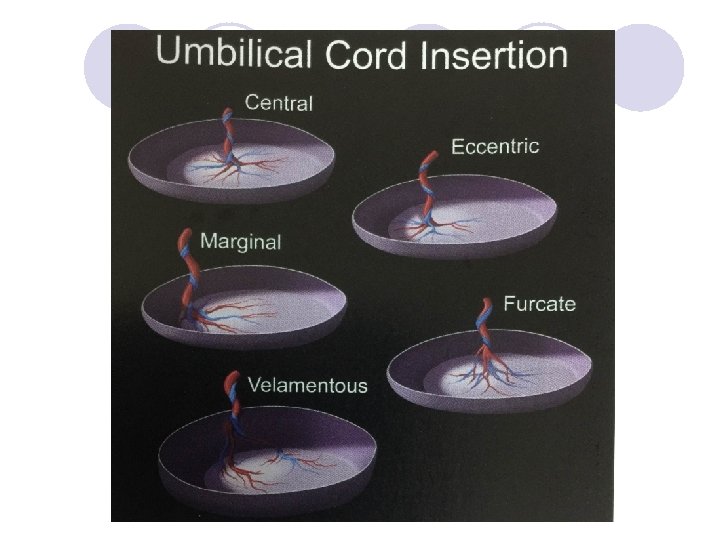
Umbilical Cord Insertion l Definition ¡Point where cord branches and its vessels are no longer covered with Wharton jelly l “Normal” umbilical cord insertion ¡Insertion in center of disc or off center but within central 2/3 of disc (paracentral or eccentric insertion) l Marginal umbilical cord insertion ¡Insertion within 1 cm of disc edge ¡Less efficient for perfusion of placenta l Furcate umbilical cord insertion ¡Umbilical vessels branch before cord inserts l No protection by Wharton jelly along branched segments l Increased risk of compression, tearing, thrombi

Umbilical Cord Insertion l Velamentous umbilical cord insertion ¡Insertion into membranes of placenta l Unprotected umbilical vessels run for some distance between the amnion and chorion before passing on to the placenta surface ¡Vessels coursing through membranes to disc are at risk for compression or injury l No protection from compression by Wharton jelly • Bleeding during the antepartum period l Can tear if near or across the site of membrane rupture (vasa previa) • Serous or fatal fetal bleeding • Fetal mortality rate: 50 %

Marginal insertion
 Chorion Stroma Intermediate Trophoblast")
Fetal membrane- Chorion laeve Amnion Epithelium Amnion Stroma (Chorion Epithelium) Chorion Stroma Intermediate Trophoblast Decidua (parietal layer)

Umbilical cord 20 X

Insertion site-20 X

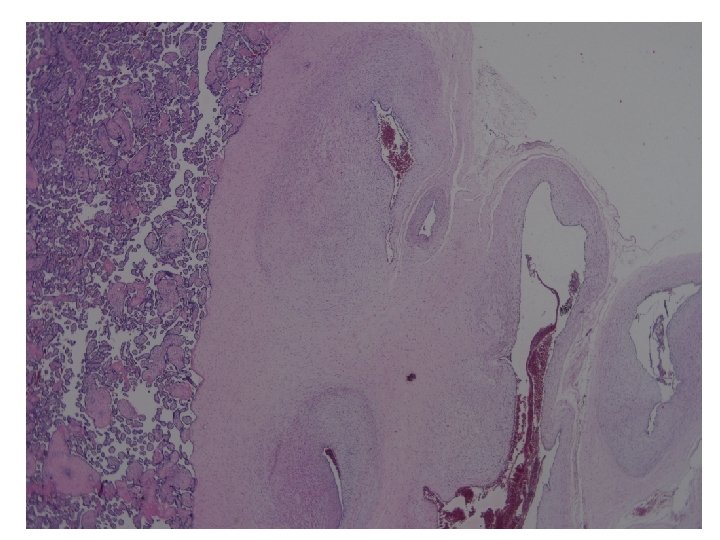
Velamentous insertion-20 X chorion amnion

Velamentous insertion-40 X chorion amnion

Insertion to placenta-20 X

Subamniotic hematoma-20 X

Pathology No. 1594480 l Diagnosis ¡Placenta l. Retroplacental hematoma, compatible with abruptio placenta ¡Umbilical cord l. Velamentous umbilical cord insertion, with subamniotic hematoma

Velamentous Insertion l Incidence: ¡About 1% of singleton pregnancies, but varies quite strikingly in literatures ¡Increase: l. Multiple pregnancies l. Single umbilical artery l. In vitro fertilization l. Malformed infants l. Etc.

Velamentous Insertion l Association with: ¡Intrauterine growth restriction ¡Preterm delivery ¡Abnormal intrapartum fetal heart rate patterns ¡Low Apgar scores at birth ¡Risk of damage to the exposed and unprotected fetal vessels during labor and delivery
: l Abdominal pedicle (umbilical cord anlage) normally")
Velamentous Insertion l Pathogenesis ¡von Franque (1900): l Abdominal pedicle (umbilical cord anlage) normally arises from most richly vascularized chorion (decidua basalis) and extends to fetus l Occasionally, the decidua capsularis may be the maximally vascularized during the first few days of pregnancy abdominal pedicle will take origin from here l As pregnancy progresses, maximal vascularity will shift to decidua basalis from which defintie placenta will develop l Abdominal pedicle retains its original position
; Benirschke and Driscoll(1967); Robinson et al (1983): “Trophotropism” l.")
Velamentous Insertion l Pathogenesis ¡Strausman(1902); Benirschke and Driscoll(1967); Robinson et al (1983): “Trophotropism” l. Cord is originally normally inserted l. During placental expansion, central atrophy and unidirectional lateral growth of the chorion frondosum • Placenta bilobata: a cord is velamentously inserted between the two lobes ¡Monie (1965): l An oblique implantation of the blastocyst

Velamentous Insertion l There may be no single pathogenesis for production of this anomaly l The vast majority of infants whose cords are velamentously inserted pass through labor and delivery without hemorrhage, it being estimated that this complication occurs in only 2% of such cases (Quek, SP and Tan, KL. Vasa pravia. Australian and New Zealand Journal of Obstetrics and Gynaecology. 1972; 12: 206)

Velamentous Insertion l Velamentous or marginal cord insertion and the risk of spontaneous preterm birth, prelabor rupture of the membranes, and anomalous cord length, a population based study. (Ebbing C, Johnsen SL, et. Acta Obstet Gynecol Scand. 2016 Oct 3. . [Epub ahead of print]) ¡Velamentous insertion of cord was associated with an increased risk of PROM, p. PROM, SPTB, and a short cord. ¡Marginal insertion was to a lesser extent associated with these complications
- Slides: 21