Vectorborne Infections Allison Liddell M D Infectious Diseases

Vector-borne Infections Allison Liddell, M. D. Infectious Diseases September 25 th, 2006

Clinical Vignette w 28 yo FBI agent on temporary assignment in the Nantahala forest in Western North Carolina presents with acute onset fever, chills, headache 3 days after Memorial Day. w Exam: confused, ill appearing, a few petechiae present on wrists and ankles w Labs: platelets=75 K, mild leukocytosis, mildly elevated transaminase w LP with 75 WBC, mostly lymphocyes with protein=154

Tick-Borne Infections in the U. S. w Lyme disease w Rocky Mountain spotted fever w Ehrlichiosis w Tularemia w Babesiosis w Colorado tick fever w Tick-borne relapsing fever w Tick-borne encephalitis w Tick paralysis w Q Fever

Ticks as Effective Disease Vectors: w Feed on blood w Wide host range w Persistent attachment (painless)- wide dispersal w Longevity w Transovarial transmission (RMSF, tularemia, Babesia) w Few natural enemies w Resistant to environmental stresses w High reproductive potential

Questing tick

Rocky Mountain Spotted Fever w Described in late 1900’s in Bitter Root Valley w Caused by infection with Rickettsia rickettsii w Obligate intracellular, requires cell culture to cultivate

RMSF transmission w Maintained transovarially in ticks w Tick vectors are hard ticks: n Dermacentor variabilis (eastern US) n D. andersoni (western US) n A. americanum (southwestern US)
: 897 -928")
Parola, Clin Infect Dis 2001 Mar 15; 32(6): 897 -928

RMSF epidemiology w Most cases occur May – September w Highest rate in children 5 - 9 years w Exposure to dogs, grassy areas risk factor w 8. 5% mortality (Billings et al)

TDH Website

TDH Website

RMSF Clinical Manifestations w w w w Incubation period 2 - 14 days Onset with fever, myalgias, headache GI findings may mimic an acute abdomen Rash appears 3 - 5 days after onset of fever Meningismus and CSF pleocytosis may occur WBC usually normal, platelets often decreased Hyponatremia occurs in 50%


RMSF Diagnosis w Serology w IF staining of tissue specimen w PCR under development

RMSF Outcome w N=6388 over 1981 -1998 w Annual case-fatality rate 3. 3% w Risk factors for mortality: n n Old age Chloramphenicol only Tetracycline not primary therapy Treatment delayed > 5 days Holman et al JID 2001

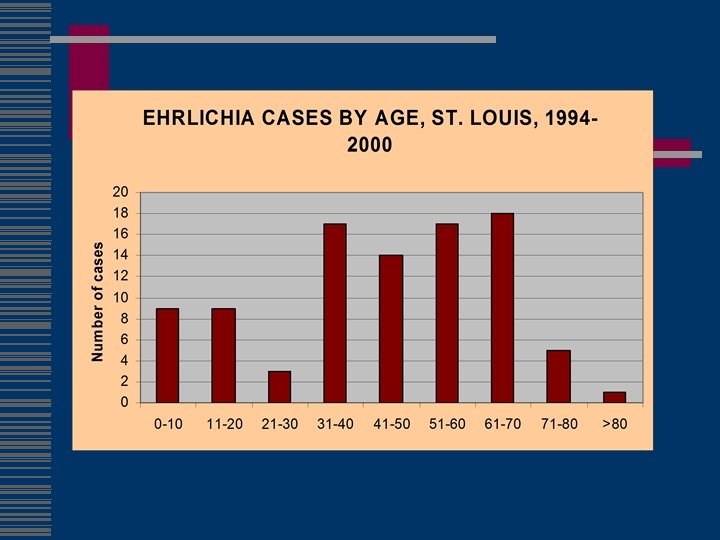
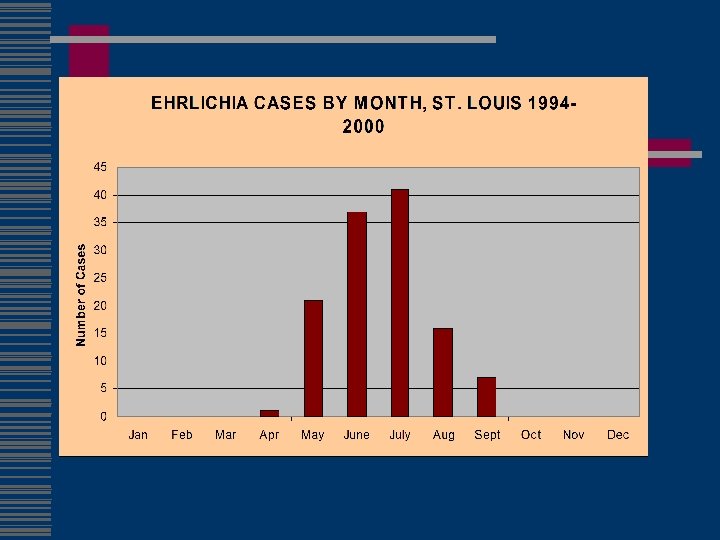
Clinical Vignette w 54 yo WM farmer in Missouri presents with 3 day h/o high fevers, chills, headache and marked malaise in June w Exam notes a confused, ill-appearing man but is otherwise unremarkable w Labs note transaminases 3 x normal, platelets 115 K, WBC 2. 1, CSF 32 WBC, protein 127

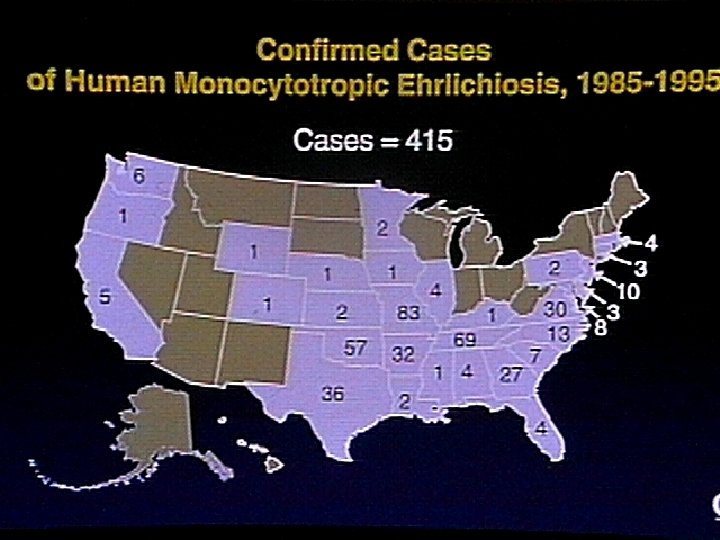
History of Ehrlichiosis w 1935 - E. canis-hemorrhagic illness in Algerian dogs w 1950 s – E. sennetsumononucleosis-like illness in Japan w 1986 – Ehrlichiosis-patient in Detroit after tick bites in Arkansas w 1991 - E. chaffeensis cultured from patient at Fort Chaffee in Arkansas
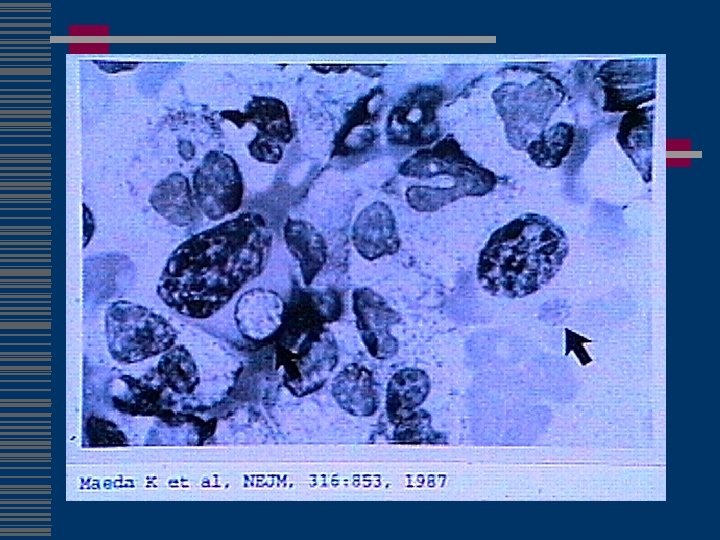

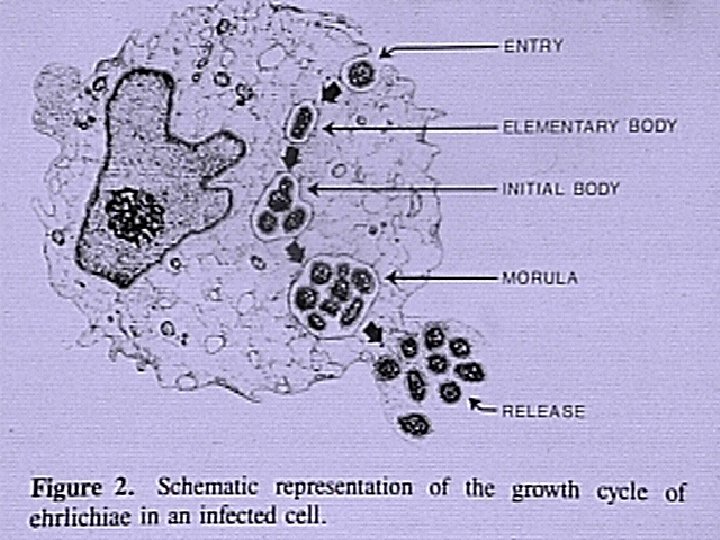
Genus Ehrlichia Small gram-negative bacteria closely related to Rickettsiae n n Obligate intracellular parasites Infect circulating blood elements Reside and replicate within membrane-bound cytoplasmic vacuoles Vertebrate reservoirs and arthropod vectors

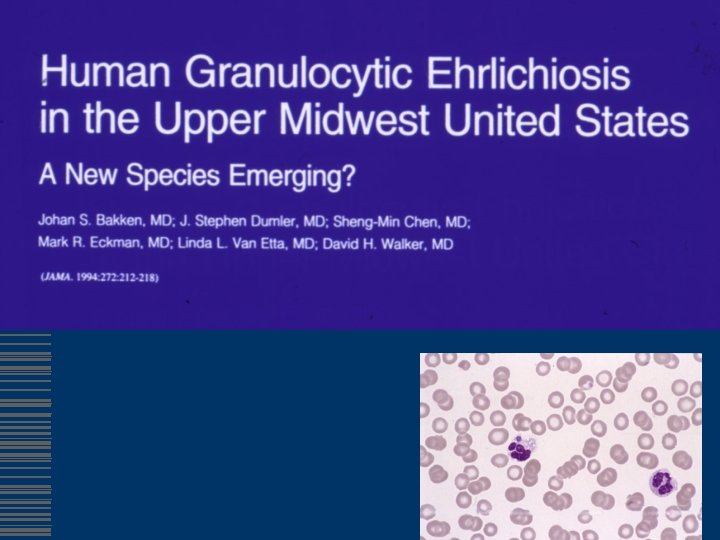
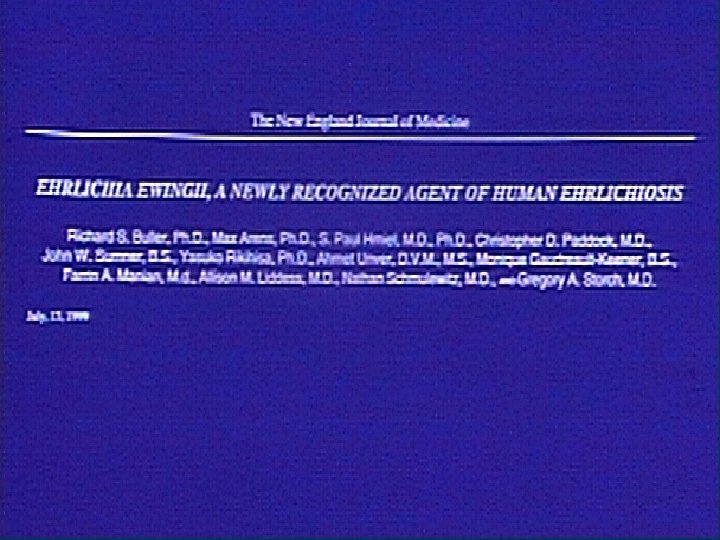
Ehrlichia ewingii w First discovered in dogs with granulocytic ehrlichiosis, 1992 w Disease is milder than E. canis infection w Manifestations include fever, lethargy and polyarthritis w Found to date in dogs in Missouri, Arkansas, Oklahoma and N. Carolina w Member of E. canis genogroup (cross-reactivity) w Experimental transmission by A. americanum

Ehrlichiae Causing Human & Veterinary Disease

Day of Treatment & Risk of Complications/Death Ehrlichiosis Fishbein DB et al, Annals Intern Med, 1994

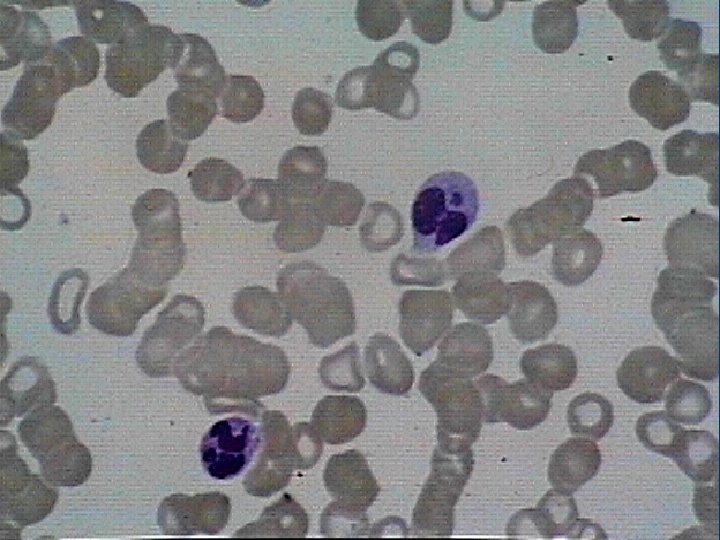
Human Ehrlichiosis Symptoms Fever Headache Myalgia HME 97 81 68 HGE 94 -100 61 -85 78 -98 Malaise Rash Confusion 84 36 20 98 2 -11 17 Dumler et al, Annu. Rev. Med. 1998. 49: 201 -213

Human Ehrlichiosis Clinical Spectrum w w DIC Pancytopenia Encephalitis/Meningitis Pulmonary infiltrates/Respiratory failure w Gastrointestinal bleeding w Renal Failure

Human Ehrlichiosis Laboratory Findings w Leukopenia w Thrombocytopenia w Elevated transaminases w Hyponatremia w >4 -fold elevation in IFA w PCR

RMSF/Ehrlichiosis Treatment w Adults: w Children: in Doxycycline 100 mg bid Doxycycline 3 mg/kg/day 2 divided doses Duration: 3 days after defervescence, minimum 5 -7 days

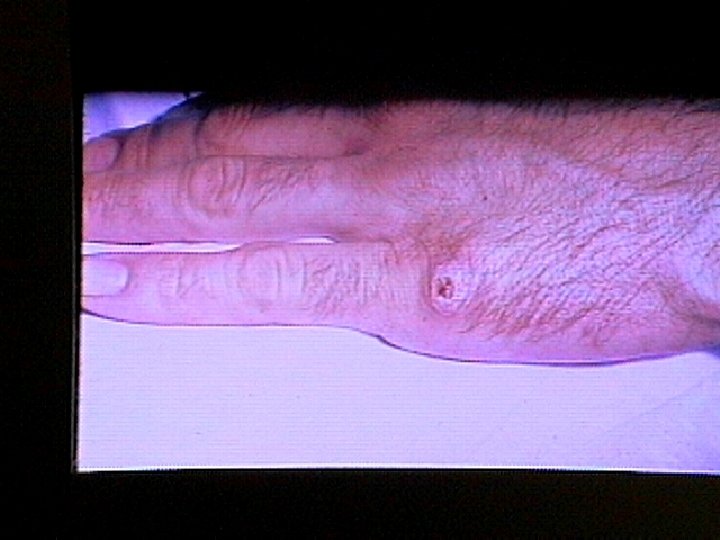
Clinical Vignette w 34 yo WF owner of a campground presents with a nonhealing lesion on the right index finger for 2 weeks, adjacent to the nail bed. w Failed Augmentin and acyclovir by PCP for “infected paronychia” w Exam notes an ulcerated lesion and regional adenopathy

Tularemia History w Mc. Coy & Chapin 1910 n “plague-like disease” of rodents in Tulare Co. CA n Bacterium Tularense w Edwards Francis n 1928 - 800 cases n isolated organism n proved vector §named the disease §developed culture and serology methods §noted risk to workers
: 897 -928")
Parola, Clin Infect Dis 2001 Mar 15; 32(6): 897 -928

Tularemia Epidemiology w 1368 cases 1990 -2000 w All states except Hawaii, but predominately MO, AK, OK & SD w Reinstated on nationally notifiable list 2000 (n=142) w Type A (biogroup tularensis) w Multiple vectors (tick, deerfly) w >250 animal species n n n rabbits hares muskrats w Other transmission n carnivores direct contact inhalation/ingestion w Peak incidence 1939

Outbreak 2001 Pneumonic Tularemia w 15 patients w 11 primary pulmonary w 1 death

Outbreak 2001 Pneumonic Tularemia Figure 1. Cases of Primary Pneumonic Tularemia, Tularemia with No Localizing Signs, and Ulceroglandular Tularemia on Martha's Vineyard, May 21 through October 28, 2000, According to the Week of Onset of Illness. Feldman et al, N Engl J Med 2001 Nov 29; 345(22): 1601 -6

Tularemia Clinical Manifestations w Ulceroglandular n n black based ulcer tender regional lymphadenopathy bubo w Typhoidal w Oculoglandular w Primary pulmonary


Tularemia Diagnosis w Titers n 4 -fold increase n single > 1: 160 w Skin test w Culture – notify laboratory

Tularemia Treatment w w Streptomycin 1 gm iv q 12 h for 10 days Gentamicin 5 mg/kg/d for 10 days w Tetracycline/chloramphenicol n associated with 15 -20% relapse w Quinolones n Excellent in vitro activity n Limited data, anecdotal experience suggests efficacy w Live attenuated vaccine for high risk groups

Tularemia Complications w Pneumonia abscess, effusion w Rhabdomyolysis w Acute renal failure w Meningitis w Pericarditis

Clinical vignette w 27 yo WM hiker spends a week in the Rocky Mtns in a cabin. w Last day of trip develops fever, chills, HA, myalgias w Resolves in 3 days, then recurs 7 days later

Tick-borne Relapsing Fever w Dutton et al- Described tick relapsing fever, caused by Borrelia duttonii and transmitted by Ornithodoros moubata in W. Africa w 13 species of Borrelia w genus Ornithodoros n n n Noctural feeder Short attachment Usual hosts small mammals w Worldwide, but only Western US w Occurs in cabin-dwellers
: 897 -928")
Parola, Clin Infect Dis 2001 Mar 15; 32(6): 897 -928

Tick-borne Relapsing Fever w acute onset of high fever with chills, headache, myalgia, arthralgia, and coughing w Hemorrhage, iritis or iridocyclitis, hepatomegaly, or splenomegaly w rash at the end of the first febrile episode • neurological findings • B. turicatae (U. S. ) • B. duttonii (Africa) • Jaundice ( 7%) • case-fatality rate 2%-5% • Primary episode 3 days • Mean period between episodes 8 days

Tick-borne Relapsing Fever w Borreliae in peripheral blood of febrile patients. Sensitivity 70% (darkfield microscopy or Giemsa or Wright's stain). w Quantitative buffy coat w Serology not useful w PCR w Jarisch-Herxheimer reaction • doxycycline (Penicillin, erythromycin, or ceftriaxone)

Clinical vignette w 23 yo WF vacationer on Long Island develops fever, malaise, and circular rash on her arm

Lyme w Most commonly reported tick-borne infection in U. S. w 1993 -1997, mean 12, 451 annual cases (CDC)

Lyme History w Cluster of cases near Lyme, CT 1975 w Johnson RC, Schmid GP, Hyde FW, Steigerwalt AG, Brenner DJ. Borrelia burgdorferi sp. nov. : etiological agent of Lyme disease. Int J Syst Bacteriol 1984; 34: 496 7.

Lyme epidemiology w B. burgdorferi sensu lato w Tick vector w Black-footed mouse reservoir w White-tailed deer host w Birds and mammals implicated in Europe
 n n Occurs 8 -14 days")
Lyme Disease Early Manifestations w Erythema migrans (90%) n n Occurs 8 -14 days after bite Single lesion, average size 15 cm Systemic symptoms may be present Secondary lesions may occur w Carditis w Aseptic meningitis w Bell’s palsy

Lyme Disease Late Manifestations w Arthritis n Knees involved in 90% n Usually resolves, 1 -2 weeks n May recur w CNS disease (rare in children)

Lyme Disease Diagnosis w Serology n ELISA n Western blot w Culture on BSK-II media n n 57 -85% sensitive skin Blood, CSF, synovial fluid w w Warthin-Starry stain PCR
 w")
Lyme Disease Treatment of Early Disease w Doxycycline ( 8 years of age) w Ampicillin n Penicillin allergic: cefuroxime axetil or erythromycin w Duration 14 - 21 days

Lyme Disease Treatment-Disseminated & Late Disease w Multiple skin lesions Oral, 21 days w Isolated facial palsy Oral, 21 -28 days w Arthritis Oral, 28 days w Persistent arthritis Parenteral, 14 - 21 days w Carditis Parenteral, 14 - 21 days w CNS Parenteral, 14 - 21 days

Does Lyme Disease Exist in Texas?
 w Similar EM rash w Long-term and serious complications")
Southern Tick-Associated Rash Illness (STARI) w Similar EM rash w Long-term and serious complications not reported w Responds to doxycycline w Organism by PCR B. lonestari w No culture w 639 cases in Texas 19861996

Lyme-Like Disease in Missouri w ECM - Yes w Serology - usually negative w Complications - Rare w Vector - Lone star tick w Etiologic agent - variant Borrelia species (? ) w Protection from vaccine Unknown

Tick-Transmitted Diseases Prevention w Avoid tick-infested areas w Wear protective clothing that covers exposed areas w Use DEET - containing insect repellants w Spray permethrin on clothes w Remove attached ticks promptly Do not squeeze

Clinical Vignette w 47 yo outdoor construction worker in Massachusetts presents with 1 week of fever, chills, DOE in June. w PMH is significant for splenectomy due to trauma. w Lab calls reporting strange finding on blood smear.
 w Worldwide distribution w Primary host white-footed")
Babesiosis w Babesia microti (Europe B. divergens) w Worldwide distribution w Primary host white-footed mouse n Peromyscus leucopus w Usually tick-borne w Can be transfusion-related

Babesiosis w Clinical Features: n n n Most infections asymptomatic fever, chills, sweating, myalgias, fatigue, hepatosplenomegaly, and hemolytic anemia. incubation period of 1 to 4 weeks more severe in immunosuppressed, splenectomized, and/or elderly. B. divergens tend to be more severe usually occurs. w Laboratory Diagnosis: thick and thin blood smears (Giemsa) w Treatment: n n clindamycin plus quinine or atovaquone plus azithromycin exchange transfusion has been used in severely ill patients with high parasitemias.

Infection with Babesia. Giemsa-stained thin smears. Note in B the tetrad (left side of the image), a dividing form pathognomonic for Babesia. Note also the variation in size and shape of the ring stage parasites and the absence of pigment.

Babesia microti infection, Giemsa-stained thin smear. The organisms resemble Plasmodium falciparum; however Babesia parasites present several distinguishing features: they vary more in shape and in size; and they do not produce pigment.

Clinical Vignette w 48 yo male presents with acute onset episodic fever abdominal pain, headache, myalgias and nausea/vomiting, then profuse sweats. w Recent trip to Thailand looking for exotic bird species. w Exam notes tender right and left upper quadrant and splenomegaly w Labs note pancytopenia
")
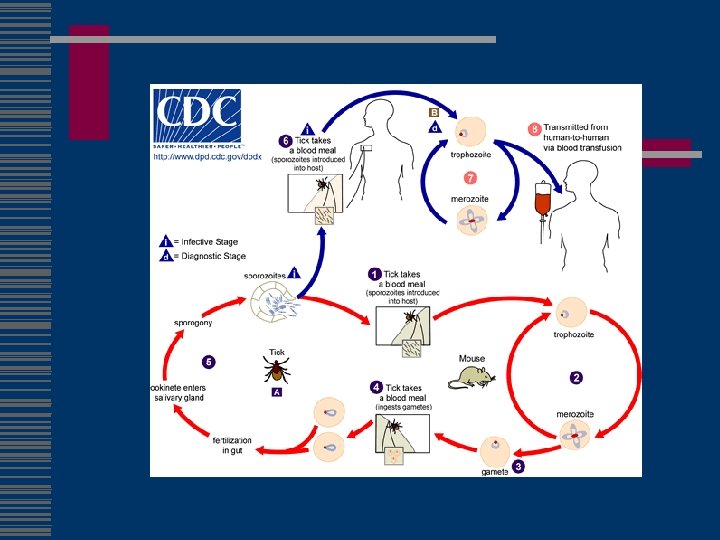
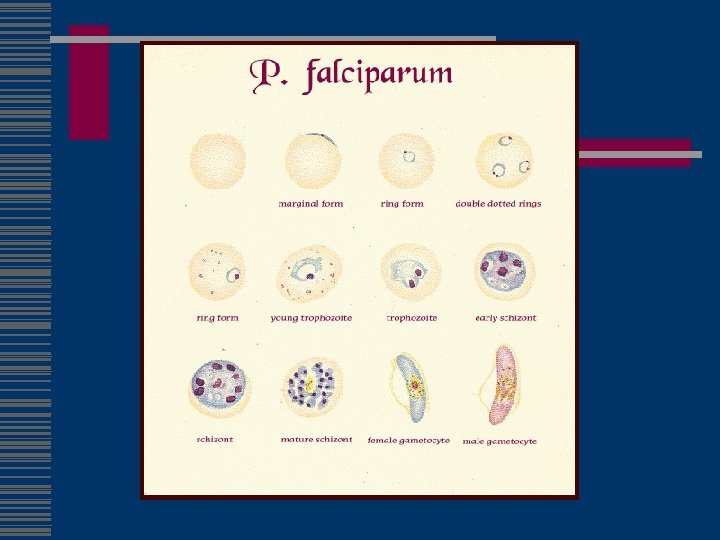
Malaria w 300– 500 million infections worldwide and approximately 1 million deaths annually (CDC) w Plasmodium falciparum, P. vivax, P. ovale, or P. malariae w infected female Anopheles mosquito w blood transfusion or congenital w Fatal cases are due to falciparum (“knobs”) w P. vivax and P. ovale parasites can persist in the liver (natural infection only) w P. malariae acute illness rare in normal hosts, causes chronic infection (GN)
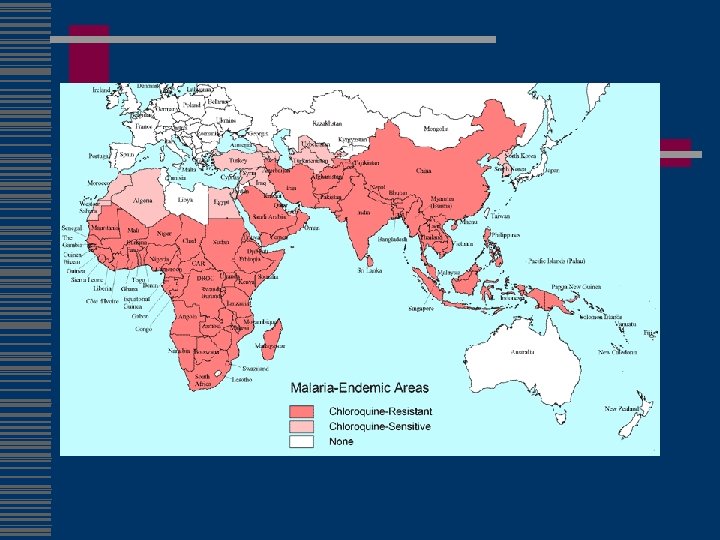


Malaria w Chloroquine-susc n n Dominican Republic, Haiti Central America west of the former Panama Canal Zone Egypt some countries in the Middle East w mefloquine resistance n n n borders of Thailand with Burma (Myanmar) and Cambodia western provinces of Cambodia eastern states of Burma (Myanmar) w Fansidar resistance n n Amazon River Basin area of South America, Southeast Asia other parts of Asia large parts of Africa

Malaria w fever and influenzalike symptoms n n chills, headache, myalgias, and malaise Classic paroxysm l l l Chill Spike Sweat n n n can occur at intervals l Falciparum less exact l Vivax/ovale tertian l Malariae quartian anemia and jaundice, seizures, mental confusion kidney failure, coma, and death 6 days after initial exposure to several months after chemoprophylaxis

Malaria Diagnosis w Peripheral smear n n Vivax/ovale Falciparum l l No mature forms High parasitemia (directly related to mortality in nonimmune) Multiple ring forms/cell Infects all ages w w w Hypoglycemia Lactic acidosis Hemolysis Acute renal failure Pancytopenia

Malaria Treatment w Hospitalize if nonimmune and suspect falciparum w Different drug than prophylaxis w Halofantine cross resistant w/mefloquine w Start 2 nd drug later w If vivax/ovale need Primaquine w Artemisin if mefloquin/cholorquine resistance w Exchange transfusion if parasitemia >15% in nonimmune

Malaria Prevention w transmission occurs w pyrethroid-containing primarily between dusk flying-insect spray in and dawn living and sleeping areas w well-screened areas, mosquito nets, clothes that cover w DEET (N, Ndiethylmetatoluamide)

Chemoprophylaxis w mefloquine or chloroquine 1– 2 weeks before w doxycycline and atovaquone/proguanil 1– 2 days before w continuously while in malaria-endemic areas w 4 weeks (chloroquine, doxycycline, or mefloquine) after w 7 days (atovaquone/proguanil) after w Terminal prophylaxis with Primaquine final 14 days n fatal hemolysis in those who are G 6 PD deficient

Chemoprophylaxis pregnancy w Long history of chloroquine and quinine use w Data supports safety of mefloquine in 2 nd an 3 rd trimester w Data in first trimester sketchy, patient must weigh risks w No Doxycycline or Primaquine w No data for Malarone

Malaria w Persons who have been in a malaria risk area, either during daytime or nighttime hours, are not allowed to donate blood for a period of time after returning from the malarious area. n n n Residents of nonmalarious countries are not allowed to donate blood for 1 year after they have returned from a malarious area. Persons who are residents of malarious countries are not allowed to donate blood for 3 years after leaving a malarious area. Persons who have had malaria are not allowed to donate blood for 3 years after treatment for malaria.

Malaria Information w http: //www. cdc. gov/travel w Voice information service 1 -877 -FYI-TRIP w CDC Malaria Hotline (770 -488 -7788) from 8: 00 a. m. to 4: 30 p. m. Eastern time w CDC Emergency Operation Center at 770 -488 -7100 n page person on call for the Malaria Epidemiology Branch.

Clinical Vignette w 72 yo WM alcoholic with CAD presents with 3 day h/o fever, myalgias, headache followed by acute onset confusion and tremulousness w Works as a nursery sales rep and travels frequently to East Texas w No improvement on levaquin w EKG afib w CSF notes elevated protein and lymphocytic pleiocytosis

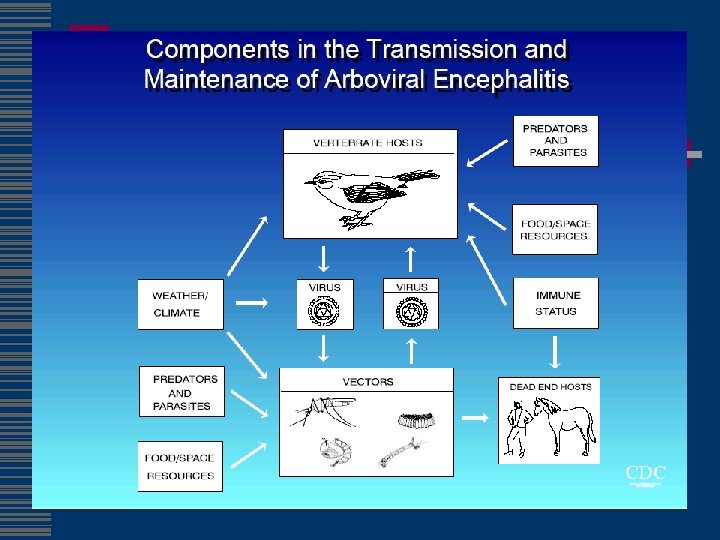
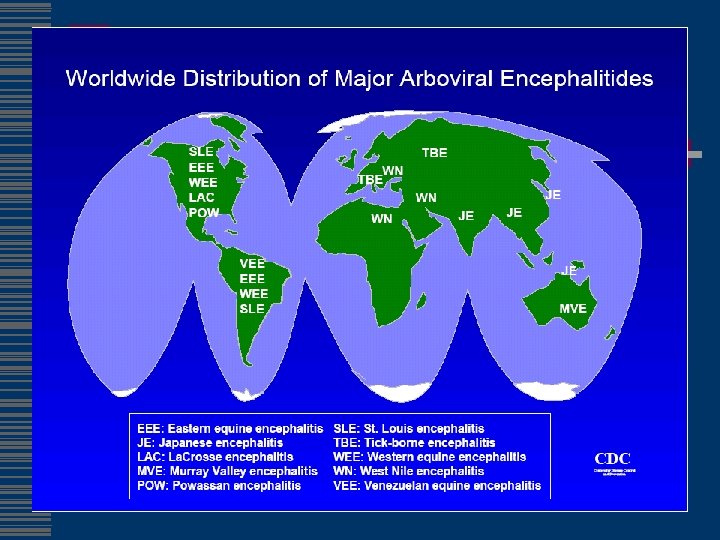
Viral Encephalitis arthropod-borne w. Bunyaviridae w Alphaviridae n n Eastern Equine Western Equine n La. Crosse w. Flaviviridae n St. Louis n Powassan (ticks) n Japanese n Tick-borne (ticks) w. West Nile Culex

Arboviral Activity Louisiana 2001 SLE Human Cases SLE 5 Human Cases EEE Equine Cases EEE Human Cases SLE Avian Cases EEE Mosquito Pools WNV Equine Cases WNV Human Cases WNV Avian Cases Outbreak or Cluster with Human Case(s)

Eastern Equine w Eastern US w Ave. 4 cases/year w Togaviridae, genus Alphavirus w 35% mortality w 35% permanent neuro defect

St. Louis Encephalitis w Aseptic meningitis or encephalitis w Majority subclinical or mild illness w Intermittent epidemic transmission - up to 3, 000 cases per year (1975) w Culex mosquitoes w Elderly - biological risk factor w Low SES areas - environmental risk factor w Outdoor occupation - exposure risk factor

St. Louis Encephalitis w Largest outbreaks in 15 years occurred in 1990 w Urban transmission in west first recognized in 1987 w Deterioration of inner cities, global warming may increase vector abundance and transmission w Unpredictable and intermittent occurrences of outbreaks w Multiple environmental, biological and social factors contributing to disease occurrence w Virus maintenance and overwintering cycle

La Crosse Encephalitis w w w Frank encephalitis progressing to seizures, coma majority subclinical or mild 70 cases/year Case-fatality ratio <1% Social costs from adverse effects on IQ and school performance w woodland habitats in treehole mosquito (Aedes triseriatus) and vertebrate hosts (chipmunks, squirrels); survives winter in mosquito w Vector uses artificial containers (tires, buckets, etc. ) in addition to treeholes

La Crosse Encephalitis w Children <16 years old: biological risk factor w Residence in woodland habitats environmental risk factor w Containers at residence environmental risk factor w Outdoor activities: behavioral risk factor w Traditional endemic foci in the great-Lakes states w Increased case incidence in mid-Atlantic states w Rural poor most affected w Disease is considerably under-reported

West Nile Virus • First isolated from a febrile adult woman in the West Nile District of Uganda in 1937 • Ecology was characterized in Egypt in the 1950 s. • Cause of severe human meningoencephalitis in elderly patients during an outbreak in Israel in 1957 • Equine disease first noted in Egypt and France in early 1960 s. • Outbreak of West Nile. Like Viral Encephalitis -New York, 1999. MMWR, 1999: 48(38); 845 -9 • Update: West Nile-Like Viral Encephalitis -- New York, 1999. MMWR, 1999: 48(39); 890 -2

West Nile Virus in the U. S. 2005

Clinical Epidemiology w w Incubation period 3 - 14 days 20% develop “West Nile fever” 2006 to date: 2171 cases, 74 deaths in U. S. 1 in 150 develop meningoencephalitis n Advanced age primary risk factor for severe neurological disease and death

West Nile Fever: Classic Clinical Description • Mild dengue-like illness of sudden onset • Duration 3 - 6 days • Fever, lymphadenopathy, headache, abdominal pain, vomiting, rash, conjunctivitis, eye pain, anorexia • Symptoms of West Nile fever in contemporary outbreaks not fully studied

Symptoms of Hospitalized Patients with West Nile Virus, New York City, 1999 Fever Weakness Nausea Vomiting Headache Change in mental status Diarrhea Rash Lymphadenopathy 90% 56% 53% 51% 47% 46% 27% 19% 2%

Neurological Presentations of West Nile Virus Infection w New York City 1999 n n n Encephalitis/meningoencephalitis 62% Meningitis 32% Complete flaccid paralysis 10% l l Confused with Guillain-Barre syndrome EMG and nerve conduction velocity-both axonal and demyelinating lesions, with axonal lesions most prominent w Preliminary data 2002 n n n Complaints of weakness out of proportion to exam Myoclonus nearly a universal finding Some patients have Parkinsonian w Previous series n Ataxia, extrapyramidal signs, cranial nerve abnormalities, myelitis, optic neuritis, seizures

West Nile Virus w 489 WNV-viremic donors as of 9/16/03 w two cases of blood transfusion-associated WNV in 2003, (TX and Nebraska). Both encephalitis and are recovering. w In 2003, all blood banks started screening for West Nile virus and will not take donations from people w/fever and headache in the week prior
 NYC 1999 Queens 677")
1999 and 2000 Serosurvey Results Location Participants Positives Seroprevalence (%) NYC 1999 Queens 677 19 2. 6 NYC 2000 Staten Is. 871 4 0. 46 NYS 2000 Suffolk Co. 834 1 0. 12 CT 2000 Fairfield Co. 731 0 0. 0

Clinical Vignette w 59 yo Mexican immigrant admit with 3 month history of progressive shortness of breath, PND, orthopnea, LE edema
 w 16 -18 million people are infected")
Chagas’ Disease w American trypanosomiasis (Trypanosoma cruzi) w 16 -18 million people are infected w 50, 000 will die each year. w poorly constructed houses found in the rural areas of the above-mentioned countries are at elevated risk of infection. Houses constructed from mud, adobe, or thatch present the greatest risk.

Chagas’ Disease w Reduviid bugs, or w "kissing bugs" w w South and Central America w w deposits feces on a person's skin at night w rubs the feces into the bite wound, an open cut, the eyes, or mouth. w w Transplacental, congenital or breastfeeding. w By blood transfusion By eating uncooked food contaminated feces of "kissing bugs. " early stage of infection (acute Chagas disease) usually is not severe, but can be fatal in infants. 1/3 chronic after 10 -20 years. average life expectancy decreases 9 years.

Chagas’ Disease w Acute: n n n 1% of cases. Romaña's sign fatigue, fever, enlarged liver or spleen, and swollen lymph glands. rash, loss of appetite, diarrhea, and vomiting occur. In infants and in very young children cerebral edema symptoms last for 4 -8 weeks. w Indeterminate (asymptomatic) w Chronic: n n n Cardiac problems, including an enlarged heart, altered heart rate or rhythm, heart failure, or cardiac arrest are symptoms of chronic disease. enlargement of parts of the digestive tract, which result in severe constipation or problems with swallowing. immune compromised, including persons with HIV/AIDS, Chagas disease can be severe.

Clinical Vignette w September 9, 1981, a 72 -year-old male from Edinburg, Texas, developed fever and weakness 16 days after being bitten by tsetse flies during a hunting trip in northwest Tanzania. Several days after onset of fever, he noticed a raised, tender, erythematous nodule (6 -8 cm in diameter) on the posterior aspect of his right arm.

East African Trypanosomiasis w six patients have shared several characteristics: n n n exposure to infected tsetse flies while visiting game parks in eastern or southern Africa, development of acute, febrile illness consistent with Trypanosoma brucei rhodesiense infection 1 -21 days after visiting detectable typanosomes on peripheral blood smears, and recovery after appropriate therapy. Only two of the five earlier cases showed clear evidence of central nervous system (CNS) involvement; both patients had elevated CSF protein, increased CSF cell count, and trypanosomes in the CSF.

East African Trypanosomiasis w Suramin is recommended for hemolymphatic stage n n does not cross the blood-brain barrier, Melarsoprol, (relatively toxic) +/- suramin when infection involves the CNS w trypanosomes are observed in the CSF w morula cells of Mott or an elevated CSF Ig. M is strongly suggest CNS involvement w elevated CSF cell count usually w should be monitored for CNS involvement during treatment and at regular intervals for 1 -2 years thereafter

Clinical Vignette w 36 yo WF presents with nonhealing lesions on face for several months w Frequent travel to Caribbean and Mexico w Recent pregnancy complicated post-partum by acute cholecystitis

Leishmaniasis w Sand fly vector w factors determining the form : species, geographic location, and immune response of the host. w Cutaneous leishmaniasis n n one or more lesions raised edge and central crater. painless or painful. Regional lymphadenopathy w visceral leishmaniasis n n fever, weight loss, and an enlarged spleen and liver (usually the spleen is bigger than the liver). lymphadenopathy. pancytopenia opportunistic infection in areas where it coexists with HIV.

Leishmaniasis
 (see Medical Letter)")
Leishmaniasis w Diagnosis: biopsy w Treatment: stibogluconate (per CDC) (see Medical Letter)

Don’t forget w w w Dengue Plague Yellow fever Onchocerciasis Loaiasis West African Trypanosomiasis w Typhus n n Endemic Scrub
- Slides: 118