Vector Borne Diseases State Conclave Igatpuri 23 24

Vector Borne Diseases State Conclave Igatpuri 23 - 24 May 2014 Joint Director of Health Services

WORLD HEALTH DAY 2014

Dengue in Maharashtra 6000 160 5610 140 138 5000 4305 4000 120 118 100 3000 80 2255 2000 60 1574 40 1138 1000 0 618 24 743 25 22 20 9 Yr 2007 Yr 2008 Yr 2009 Yr 2010 Yr 2011 Cases Deaths Yr 2012 Yr 2013 359 20 0 Yr 2014 0

Health Circle Wise Dengue Deaths 2013 Nagpur, 32, 23% Akola, 6, 4% Thane, 32, 23% Nashik, 33, 24% Latur, 11, 8% Aurangabad, 4, 3% Kolhapur, 6, 4% Pune, 14, 10%

2 2 10 2 2 1 8 4 8 2 3 8 3 4 4 10 2 3 1 7 1 2 Dengue Deaths from Rural Maharashtra 2013 2 7

INITIATIVES TO CONTAIN DENGUE

‘VBD Free Village’ Scheme ����� ��� Aim • To do fortnightly entomological surveillance of every village. • To submit its’ report to VHNSC. • To take appropriate action based on this report. Current Situation MPW submits monthly village wise report to District level but its’ authenticity is doubtful. Planning • Prepare fortnightly surveillance calendar of every MPW ANM & submit it to gram panchayat. • Take help of ASHA & AWW. • Training of student volunteers. ( 2/ Village) • Technical guidance to VHNSC by MO.

ROLE OF VHNSC • 15% of VHNSC untied funds can be utilized for source reduction of VBD vectors • Activities to be carried out by utilizing this fund – Minor engineering – Application of temephos in water containers – Human Resource required for source reduction & cleaning – IEC – Construction of Guppy fish hatchery

VBD Free Health Institutions PHC Chincholi Chandrapur • Study PHC Shevgaon Ahmadnagar by Dr Kharat ADHS & Dr. Kambale DD Thane is an eye opener. • 5 doctors among deceased in 2013 Dengue Mortality List.

Coordination With Urban Counterpart Urban verses Rural Dengue Cases Rural, 2715, 48% Urban, 2895, 52% Role of DD & CS • Review of urban areas in every monthly meeting. • Special focus on ü Surveillance ü Vector management ü Lab facilities ü Implementation of civic bye laws ü Technical inputs wherever needed.

Dengue Active Search

Dengue – Active Case Search • Develop SURVEILLANCE NETWORK for Dengue. • Block level workshop for Private Medical Practitioners for reporting Suspected/ Confirmed Dengue cases to Public Health authority. • Disseminating Suspected Case definition • Displaying request for Dengue reporting with contact numbers of DHO & DMO in every clinic, hospital & labs. • Weekly visit to Private Medical Practitioners by MPW/ HA/HS & all other officers during field visits.

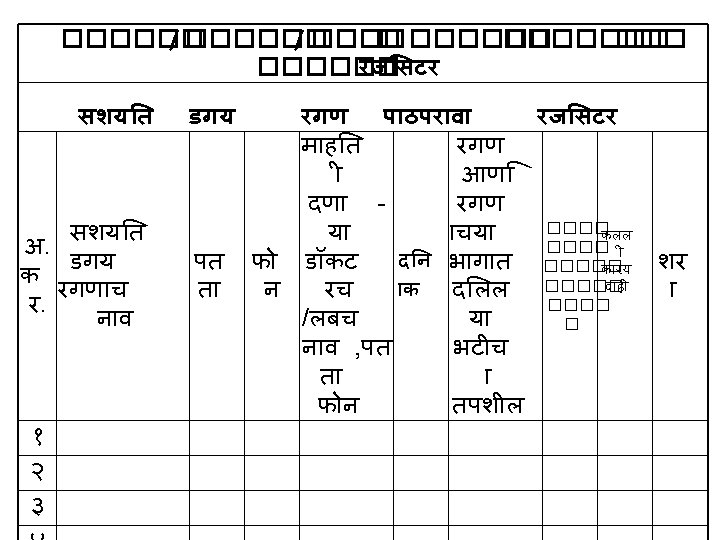
Actions after Dengue case get reported • Visit to suspected case & serum sample collection. • Entomological surveillance of work place & home of suspected case along with adjacent 100 houses. • Rapid Fever Survey of adjacent 100 houses. • If required collection of 5 -10% sample collection. • Emptying positive container, use of antilarval. • Necessary vector management actions with people’s support – Cleanliness Drive, Dry day, Fogging etc • Appropriate treatment to affected • IEC

Sentinel Surveillance Hospitals Dengue, CHK & JE • Monthly visit to these centers by District level officers. • Review inventory & address other issues, if any. • Representatives of SSH should attend monthly review meetings at district & divisional level.

Dengue Case Management • Role of CS – 1. Plan on job training for all clinicians working at public hospitals. 2. Guidance from DMER faculties. 3. One half day workshop per 2 -3 blocks 4. Use of clinical management booklet available on NVBDCP website. www. nvbdcp. gov. in Dengue Deaths Urban, 40, 29% Rural, 98, 71%

ELIMINATION OF LYMPHATIC FILARIA 2015

Neglected Tropical Diseases • 66 th World Health Assembly last year declared 17 diseases as NEGLECTED TROPICAL DISEASES. • FILARIA is one of them…. !

FILARIA ENDEMIC DISTRICTS OF MAHARASHTRA

High Endemic district for Filaria Sr No Region No. of District Name of District under M. D. A 1 Thane 2 Nashik 2 Nandurbar, Jalgaon 3 Pune 1 Solapur 4 Kolhapur 1 Sindhudurg 5 Latur 3 Latur, Nanded, Osmanabad 6 Akola 3 Akola, Amrawati, Yeotmal 7 Nagpur 6 Nagpur, Wardha, Bhandara, Gondia, Chandrapur, Gadchiroli Total 17
 • Goal : To eliminate lymphatic filariasis from India by")
National Health Policy (2002) • Goal : To eliminate lymphatic filariasis from India by the year 2015. • Objectives: (i) To reduce and eliminate transmission of LF by Mass Drug Administration of Diethycarbamazine Citrate (DEC). (ii) To reduce and prevent morbidity in affected persons, and (iii) To strengthen the existing health care services.

NATIONAL FILARIA CONTROL PROGRAMME Launched in 1955. Elimination of LF means LF ceases be public health problem when mf rate is less than 1 % & the children borne after initiation of ELF are free from ciculating antigenemia. Vector to Control Detection & t/t of Filaria Cases Delimitation of endemic areas WHA 50. 29 in 1997 – ELF by 2020. q National Health Policy (2002) – ELF by 2015. q

TWIN PILLARS OF ELF 1 Transmission Control Annual MDA 2 Disability Prevention & Management * Home Based management for limb lymhodema * Hospital Based Surgical Management for Hydrocele.

Mass Drug Administration -2004 l l Interruption of transmission of filariasis by Annual MDA for 5 years or more to the population except: - children below 2 years - pregnant women - seriously ill persons DEC + Albendazole in selected districts 17 districts. 27. 5 million population

Morbidity Management Home based management of lymphoedema cases and l Up-scaling of hydrocele operations in the identified CHCs / District hospitals/ medical colleges. l

FILARIA CONTROL STRATEGIES Surveillance Vector Control Diagnosis & Treatment Morbidity Management Mass Drug Administration • Base Line • Disease • Larvicides • Minor engineering • 34 Night Clinics • 16 control units • Elephantisis • Hydrocele Operation • DEC& Albendazole to all population SINCE 2004

INFRASTRUCTURE UNDER NATIONAL FILARIA CONTROL PROGRAMME FILARIA SURVEY UNIT 1. 2. 3. 4. 5. 6. Aurangabad, Thane, Nasik, Pune, Akola, Nagpur FILARIA CONTROL UNIT 1. 2. 3. 4. 5. 6. 7. 8. Vasai, Palghar Akkalkot Nanded A’vati Rajura Chandrapur Gadchiroli 9. 10. 11. 12. 13. 14. 15. 16. Dhanora Bhandara Pawani Nagpur(R) Umred Nagpur corp Wardha, Thane corp
 Amravati (N.")
Name of District & Controlling Night Clinic Nagpur (N. F. C. U) Amravati (N. F. C. U) Chandrapur (N. F. C. U) Wardha (N. F. C. U) Bhandara (N. F. C. U) Sr. No 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Name of the Night Clinic Gumthala Mandhal Bhivapur Kanholibara Talwel Walgaon Nandgaon Maushi Warora Sawali Chimur Seloo Wardha Karanja Karadi Palandur Lakhandur
 Sindhudurg (DMO)")
Name of District & Controlling Night Clinic Nanded (N. F. C. U) Sindhudurg (DMO) Solapur Akkalkot (NFCU) Osmanabad (DMO) Akola (DMO) Yeotmal (DMO) Gondia (D. M. O) Nandurbar (D. M. O) Jalgaon (D. M. O) Latur (D. M. O) Sr. No 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 Name of the Night Clinic Pethwadaj Jaldhara Malvan Vairag Valsang Umraga Murum Mahan Babhulgaon Vani Ghatanji Tiroda Navapur Borad Parola Jalkote Devani

Activities under NFCP I National Filaria Control units : 16 • Night blood surveillance in jurisdiction – 10% Popln • B. S. Coll by F. I. – 600 B. S. / F. I. • Examination of blood slides by L. T. • Treatment • Weekly Anti larval measures • Morbidity management • Hydrocelctomy

Activities under NFCP II • Survey Units : 6 ü Regional night blood surveillance – 10% popln ü Entomological surveillance ü B. S. coll by F. I. – 3000 B. S. /Mnth by 2 F. I. ü Examination of blood slides by L. T. ü Treatment • Night Clinics : 34 ü Night blood surveillance in jurisdiction – 100% popln in 2 -3 years ü B. S. coll by F. I. - 1500 B. S. / F. I. /Mnth ü Examination of blood slides by L. T. ü Treatment ü Morbidity management

TOWARDS ELIMINATION OF FILARIA MF% TREND 2, 86 1, 43 1, 13 20 12 - 20 11 - 0, 43 13 0, 54 12 0, 51 11 10 0, 46 20 09 - 09 20 08 - 08 20 07 - 07 20 06 - 06 20 05 - 20 04 - 05 0, 44 20 10 - 1, 23

Base Line Data Districts with > 1 mf rate 2011 -12 Fixed • O’bad • Nanded • Gadchiroli • Gondia Random 2012 -13 Fixed • Nagpur • Nanded Random 2013 -14 Fixed Random • Nagpur • Nanded • Ch’pur • Nanded • Gadchiroli • Gondia • Ch’pur
 – Validation of Elimination Status • Criteria to go for")
Transmission Assessment Survey (TAS) – Validation of Elimination Status • Criteria to go for TAS – ü 5 MDA rounds with 65 % consumption rate. ü Mf rate < 1% in last 3 years at every spot in Base line survey. • Such districts will undergo ADDITIONAL MF SURVEY…! If mf < 1 at all 10 spots of survey…. • TAS – Survey of school children of 1 & 2 Standard. If TAS succeeds – ELF validated. • In 2013 -14 – Districts selected – Thane, Akola, Jalgaon & Sindhudurg. Thane failed in ADD SURVEY • Jalgaon & Sindhudurg completed TAS in April. Akola will do it in JUNE.

• Coordination with NFCU, NFSU & Night clinics in their jurisdiction. • Monthly review of Filaria units. • Field visits by DHO, ADHO, THO & MO to different Filaria Units • Planning & Monitoring – Filaria Surveillance activity from 16 -31 August 13. • Active role in MDA planning & implementation. • Validation of elephantiasis & hydrocele cases from MO PHC. • Line listing of cases from SC to district level. (New/Old) • Morbidity management Clinics at SC, PHC & RH/SDH. • Planning of Hydrocelectomy Camps at RH/SDH/DH as per line list of cases 37

Weekly Morbidity Management Clinic at every SC/PHC/RH

Role of CS in VBD Control • Focus on Passive surveillance of Hospitals – Review of hospitals with poor passive surveillance. • Establish Sentinel Hospitals for Malaria to reduce malaria mortality. • Assure functional SSH for Dengue, CHK, JE. • On job case management trainings for all clinicians. • Planning of Hydrocelectomy Camps at RH/SDH/DH as per line list of cases. • Regular IDSP reporting. 39

MALARIA

MALARIA TREND IN STATE 160000 250 140000 200 120000 100000 150 80000 100 60000 40000 50 20000 0 2007 2008 Positive 67850 PF 22691 Death 182 67333 22257 148 2009 2010 2011 2012 2013 93818 139198 96584 24962 32391 21405 227 200 118 58499 11854 96 43676 9197 80 2013 upto APR 10747 2499 17 2014 upto APR 8418 2583 3 0

API range MAP of the State API less than 1 API 1 -5 API more than 5
 2013 NIL Collection Villages ( Average) 2014")
Active Surveillance NIL Collection MPWs ( Average) 2013 NIL Collection Villages ( Average) 2014 2013 11 12 6 7 3 5 1 Satara Beed ia nd Go g ur ud dh Na Be Thane 3 3 Sin 4 7 4 ed 4 7 ed 6 nd 8 Parbhani 2014

Passive Surveillance – Districts with > 30 % PHCs with < 15 % BS Collection 64 60 50 47 32 30 dh ud ur g d ba A' ed ra da an Bh 34 Sin 37 a dh ar W ed Be ia nd Go iga d ba d O' Ra Ra tn ag ir i 38 Na nd 68

Passive Surveillance – Districts with > 30 % Hospitals with < 15 % BS Collection 58 62 65 69 70 Y'mal Jalna Buldhana Thane 38 Washim Gondia Ch'pur Bhandara Hingoli Wardha O'bad Sindhudurg Nanded Parbhani Beed Akola Gadchiroli Ratnagiri Latur 38 33 39 40 40 42 42 43 43 44 50

MPW – BACKBONE OF VBD CONTROL ACTIVITY Ask every MPW to prepare his ATP ( Fortnightly Surveillance Programme) based on SF 1 Register. Ensure his field visits by cross checking ATP with his daily diary. Stenciling will help to cross check his visits in field. Check time lag between BS Collection & Transportation to lab. Check line list of Breeding sites & action taken by MPW. Vacant area should be given to adjacent MPW. New & untrained MPWs need mentoring & on job training.

MPWs Surveillance Calender PHC Murumgaon Gadchiroli

11 THINGS MPW SHOULD DO DURING HIS FIELD VISITS. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. H-t-H survey of 100 houses daily for fever cases. Entomological survey of 10 % houses daily. Necessary action & reporting of villages with > than normal entomological indices. Visit to migrated population/ labours on development project. Enumeration & visit to breeding sites & guppy fish hatcheries. Introduction of Guppy fishes in appropriate breeding sites Visit to ASHA – RDK use, RT verification of pts treated by ASHA. School visit – especially ASHRAM SHALA – Surveillance & IEC. Water Quality related work – storage facility of TCL , Regularity of water purification Visit to Private doctors & labs for malaria, Dengue cases information Meeting with VHNSC members & seek necessary help in vector control.

Laboratory Issues • Quality of BS. • Hospital based LTs are not regular in submitting their positive & negative slides for cross checking. • Time lag • Need of integration & combined meetings of all LTs working under different schemes. • Functional Malaria Clinics

TIME LAG BSC & EXAMINE- Dist: Buldhana – Antrikhedekar PHC 1 MONTH, 21 DAYS, 19 DAYS, 18 DAYS, 17 DAYS, 10 DAYS,

MALARIA CLINIC Concept of Malaria Clinic – BS Collection of Fever cases in OPD Ø Immediate BS Examination & Ø Delivering of first dose of RT in OPD itself. Ø Malaria clinic should be functional in all PHCs & RH/SDH where LT for Malaria diagnosis. Keep separate register for cases treated in Malaria Clinic. Maintain quality of diagnosis, staining with the help of Malaria Supervisor & DMO. Within 2 hrs of BS collection result should be communicated to patient & treatment should be started. Display Malaria treatment guidelines in OPD. BS Examination procedure & different stages of Malaria Parasite should be displayed in every Lab.

SENTINEL HOSPITAL FOR MALARIA Two hospitals should be identified in every district as Sentinel Hospital for Malaria. Aim – 1) Assess number & reasons of severe malaria cases. 2) Improve referral of severe Malaria Cases. 3) Improve management of severe malaria cases. Medical & paramedical staff should be well trained about diagnosis & management of severe malaria cases. Lab should be well equipped. Essential medicine stock & other facilities to treat severe malaria cases. These hospitals should be known to all health staff for appropriate referral.

Drug Policy for Malaria • Every Medical Officer should be well verse with Drug Policy for Malaria. • It’s freely available on NVBDCP website www. nvbdcp. gov. in • Copy of this drug policy should be available with every MO.

Treatment of P. vivax Malaria Day 1 Age CQ Day 2 PQ (2. 5 mg) CQ Day 3 PQ (2. 5 mg) CQ tabl et Days 4 to 14 PQ (2. 5 mg) Less than 1 yr ½ 0 ¼ 0 0 1 -4 years 1 1 ½ 1 1 5 -8 years 2 2 1 2 2 9 -14 years 3 4 1½ 4 4 15 yrs or more* 4 6 2 6 6 Pregnancy 4 0 2 0 0
 FOR PF TREATMENT Blister Infant (< 1 year)")
Age Wise Co-blister ACT Packs (ACT-SP) FOR PF TREATMENT Blister Infant (< 1 year) 1 -4 Years 5 -8 Years 9 -14 Years Adults Colour PINK YELLOW GREEN RED WHITE No. of tablets Day 1 One tablet of Artesunate (25 mg) and One tablet of Suphadoxine. Pyremethamin e ((250 mg + 12. 5 mg) One tablet of Artesunate (50 mg) and One tablet of Sulphadoxine Pyremethamin e (500+25)mg One tablet of Artesunate (100 mg) and One tablet of sulphadoxine Pyremethami ne (750 mg+ 37. 5) mg One tablets of Artesunate (150 mg) and Two tablets of Sulphadoxine Pyremethamine 500+25 mg) mg each One tablet of Artesunate (200 mg) and Two tablets of Sulphadoxine pyremethamine (750+37. 5) mg each or three tablets of Sulphadoxine Pyremethamine (500+25) mg each Day 2 One tablet of Artesunate (25 mg) One tablet of Artesunate (50 mg) One tablet of Artesunate (100 mg) One tablet of Artesunate (150 mg) One tablet of Artesunate (200 mg) Day 3 One tablet of Artesunate (25 mg) One tablet of Artesunate (50 mg) One tablet of Artesunate (100 mg) One tablet of Artesunate (150 mg) One tablet of Artesunate (200 mg)

VBD Outbreaks…

Districts with Major VBD Outbreaks 2014 13 8 districts with single outbreak. 11 8 8 2 Ratnagiri Latur Nanded Amaravati Chandrapur A'nagar Thane Dhule Gadchiroli Beed Akola Gondia Satara 2 Jalgaon 2 3 4 5 5 6

Timeliness of OB Reporting 2014 > 20 days, 6, 7% Within 2 days, 9, 11% 2 -4 days, 23, 28% 5 -19 days, 44, 54% Most delayed OB reporting by – Chandrapur (3) & one each from Thane, Satara & Akola

Disease Wise Outbreaks 2014 Fever, 44, 52% Malaria, 9, 11% Dengue, 25, 30% Undiagnosed OBs • Lab support • Support of different specialities Chikungunya, 6, 7%

Division Wise OBs Pune, 4, 5%A'bad, 1, 1% Latur, 9, 11% Nagpur, 25, 30% Akola, 9, 11% Thane, 11, 13% Nashik, 23, 28%

Monsoon Preparedness 10 Point Programme Activity Responsible Officer Malaria Awareness Month DHO, CS, DMO & MOH June month Dengue Awareness Month DHO, CS, DMO & MOH July month Workshop for Private Doctors – BLOCK LEVEL DHO CS DMO THO By 15 June ASHA Training – RDK use & Malaria treatment DHO, THO, DMO First week of June Review meeting of Block & District level Supervisors DHO, DMO First Week of June Interdepartmental Coordination CEO, DHO, CS, DMO 1 -15 June Meeting of Sentinel Surveillance Hospitals of Dengue, CHK AND Malaria DHO, CS, DMO 1 -15 June Workshop on Clinical Management – RH/SDH CS, DMO MOs Timeline 1 -15 June Press Conference & Dissemination of key messages through Print & electronic media DHO, CS, DMO & MOH June & July AND as per local need Meeting of VHNSC members at PHC DHO, DMO, THO, MO 1 -30 June

Surveillance Community Mobilization Entomological Surveillance Octagon of VBD Containm ent IEC Outbreak Response Integrated Vector Control Laboratory Support Case Manage ment

No one in the 21 st century should die from the bite of a mosquito, a sand fly, a black fly or a tick. Margaret Chan Director General World Health Orgnization
- Slides: 63