Vasodilators Dr S Parthasarathy MD DA DNB MD
, Dip. Diab. DCA,")
Vasodilators Dr. S. Parthasarathy MD. , DA. , DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics. Ph. D ( physiology), IDRA, FICA

Nicorandil Alliskrein Prazocin

Sodium nitroprusside • SNP is a direct-acting, • nonselective peripheral vasodilator that causes relaxation of arterial and venous vascular smooth muscle. • Its onset of action is almost immediate, and its duration of action is transient, requiring continuous intravenous infusion to maintain a therapeutic effect.

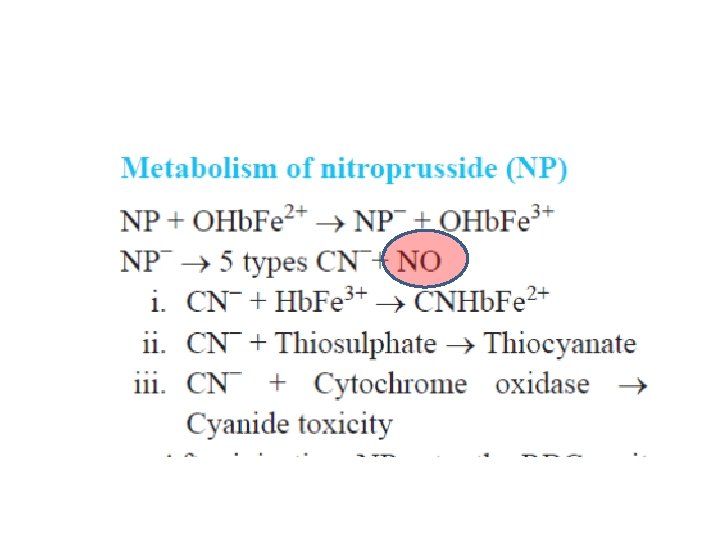
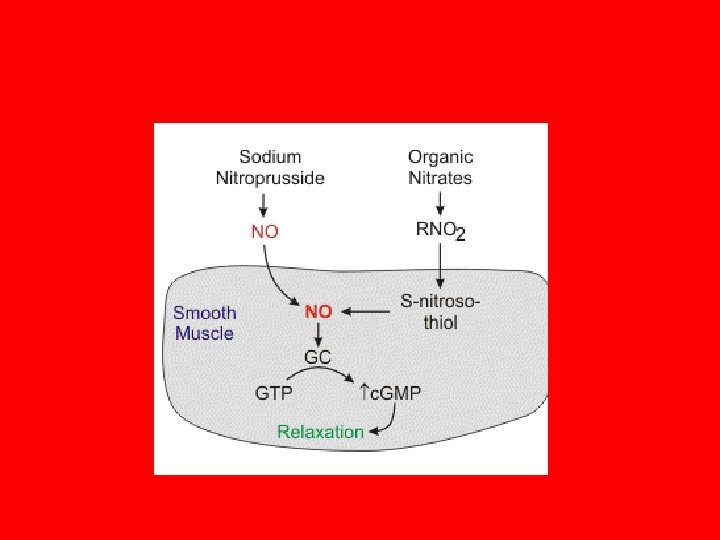
Mechanism • SNP interacts with oxyhemoglobin, dissociating immediately and forming methemoglobin while releasing cyanide and NO. • NO is the active mediator responsible for the direct vasodilating effect of SNP. • Methemoglobinemia is unlikely

Dosage Initial dose 0. 3 to 0. 5 µg/kg/min IV titrated to the desired systemic blood pressure (should not exceed 2 µg/kg/min or a maximum rate of 10 µg/kg/min for no longer than 10 minutes) Immediate onset and short duration of action Continuous infusion required to produce sustained pharmacologic effect Continuous monitoring of systemic blood pressure recommended (indwelling arterial catheter a consideration) Infusion protected from light by aluminum foil

• Arterial dilator • Decreased afterload • Also a venous dilator • Reflex tachycardia • Coronary steal Duration of action: 1 to 10 minutes Onset of action: nearly immediate

• Increased cerebral blood flow • Possible patients with ? Decreased intracranial compliance • The effect may increased ICP

Others • Decreased renal perfusion • Blunted HPV – beware of Fi. O 2 ! • Inhibits platelet aggregation • Each 2 m. L vial contains the equivalent of 50 mg sodium nitroprusside dihydrate in sterile water • In 500 ml of 5 % dextrose • • Cover with aluminum foil Not necessary to cover the iv set

Metabolism • Metabolism of SNP begins with the transfer of an electron from the iron of oxyhemoglobin to SNP, yielding methemoglobin and an unstable SNP radical. • The unstable SNP radical breaks down, resulting in the nonenzymatic release of all five cyanide ions, one of which reacts with methemoglobin to form cyanmethemoglobin.

It does not cause hypotension ? • Cyanide toxicity should be suspected in any patient who is resistant to the hypotensive effects of the drug despite maximum infusion rates (>2 µg/kg/minute or 10 µg/kg/minute for longer than 10 minutes) or in a previously responsive patient

Treatment • • • Stop SNP ABG – metabolic acidosis Sodium bicarbonate Sodium thio sulfate Or Sodium nitrite • Last hemodialysis

Indications • • • Controlled hypotension Hypertensive emergencies CCF and LV failure Aortic surgery Rewarming from bypass Kids – ok Pregnancy ? Lactation ? ? Think of anemia and hypotension !!

Contraindications of SNP ? ? • Secondary hypertension / coarctation • Impaired cerebral circulation • When the CCF is high output failure like sepsis ?

NITROGLYCERIN • Sobrero taste in 1846 to get intense headache ! • Mainly venous capacitance • Less arterial vasodilation • Sublingual 0. 3 mg • Oral ( 10 mg tds ) • Buccal( 2. 5 mg ) • Transdermal ( 0. 1 mg/ hour patch)

Mechanism • Nitroglycerin, like SNP, generates NO, which stimulates the production of c. GMP to cause peripheral vasodilation. • In contrast to SNP, which spontaneously produces NO, nitroglycerin requires the presence of NO synthetases 5 – 20 mic/ minute 5 mic spray available

Actions of NTG • Venous dilatation predominant • Relaxation of bronchial smooth muscle • Relaxation of gastrointestinal smooth muscle (sphincter of Oddi) • Relaxation of esophageal and ureteral smooth muscle tone • Cerebral vasodilation (may increase intracranial pressure) • Increased bleeding time

Why NTG veno selective ? • Enzymes which converts nitrates to NO is abundant in venous smooth muscle compared to arterial smooth muscle cells. • This is possible the cause of predominant venoselective properties of nitrates.

Indications of NTG • • • Angina Pectoris Cardiac failure Controlled hypotension Anal fissures Tendinopathies Spasm of sphincter of oddi
 Facial flushing Tolerance Decreased sensitivity")
side effects of NTG headache (dilation of meningeal vessels) Facial flushing Tolerance Decreased sensitivity to heparin • concurrent administration of nitroglycerin and erectile dysfunction drugs within 24 hours is not recommended.

SNP NTG Arterial and venous Predominant venous Aluminium foil No Cyanide poisoning risk No Other uses – no Yes Afterload reduction Preload reduction

Hydralazine • Hydralazine, a direct acting vasodilator, is highly selective for arterial resistance vessels. • Mechanism of action not well known • Possibly affecting calcium movement • Opens potassium channels • • Hypertension also in pregnancy – emergencies 20 mg in 20 ml 1 ml iv boluses – may take ten minutes 25 mg tablets bd – given

Side effects of vasodilators • Tachycardia • Orthostatic hypotension • Sodium and water retention
")
Contraindications to hydralazine • Known hypersensitivity to hydralazine • Idiopathic systemic lupus erythematosus (SLE) • Severe tachycardia and heart failure with a high cardiac output (e. g. thyrotoxicosis) • Myocardial insufficiency due to mechanical obstruction (e. g. aortic or mitral stenosis or constrictive pericarditis) • Isolated right ventricular heart failure due to pulmonary hypertension (cor pulmonale) • Dissecting aortic aneurysm

Mixed ONE Two Arterial Venous One – cardiac function curve Two : vascular function curve Watch for the intercept points with different drugs watch for cardiac output (CO) with drugs Watch for P RA ( right atrial pressure)

Adenosine • Adenosine is a naturally occurring purine nucleoside that forms from the breakdown of adenosine triphosphate (ATP). • Mechanism • Increased camp • Increased potassium channel activation • Inhibits L type calcium channels

Indication of adenosine • Termination of SVT • 6 mg bolus –central line ? • Other wise 60 second interval - 12 mg dose • Action lasts for ten seconds only • The rate of adenosine infusion required to produce controlled hypotension is unlikely to result in plasma concentrations that alter cardiac automaticity or the conduction of cardiac impulses. continuous peripheral intravenous infusion at a dose of 140 µg/kg/min for six minutes using an infusion pump

Adenosine – other • Not effective for atrial flutter or fibrillation • Contraindicated in AV blocks • Theophyllines antagonize the binding of adenosine to purine receptors • Acadesine is a purine nucleoside analog that may decrease myocardial ischemic injury by selectively increasing the availability of adenosine in ischemic tissues.
, headache (2%), sweating, palpitations,")
Side effects of adenosine • Cardiovascular • Facial flushing (18%), headache (2%), sweating, palpitations, chest pain, hypotension (less than 1%). • Respiratory • Shortness of breath/dyspnea (12%), chest pressure (7%), hyperventilation, head pressure (less than 1%). • Central Nervous System • Lightheadedness (2%), dizziness, tingling in arms, numbness (1%), apprehension, blurred vision, burning sensation, heaviness in arms, neck and back pain (less than 1%). • Gastrointestinal • Nausea (3%), metallic taste, tightness in throat, pressure in groin (less than 1%).

• Endothelin receptor antagonist • Sitaxentan, ambrisentan and bosentan are mainly used for the treatment of pulmonary arterial hypertension

Summary • • SNP NTG Hydralazine Adenosine • Thank you
- Slides: 32