VASA PREVIA Clinical Presentations Outcomes and Implications Purpose
















- Slides: 19
VASA PREVIA! Clinical Presentations, Outcomes and Implications
Purpose � Evaluate patients with diagnosis of vasa previa and assess outcomes in order to develop recommendations
Increased risk of Vasa previa
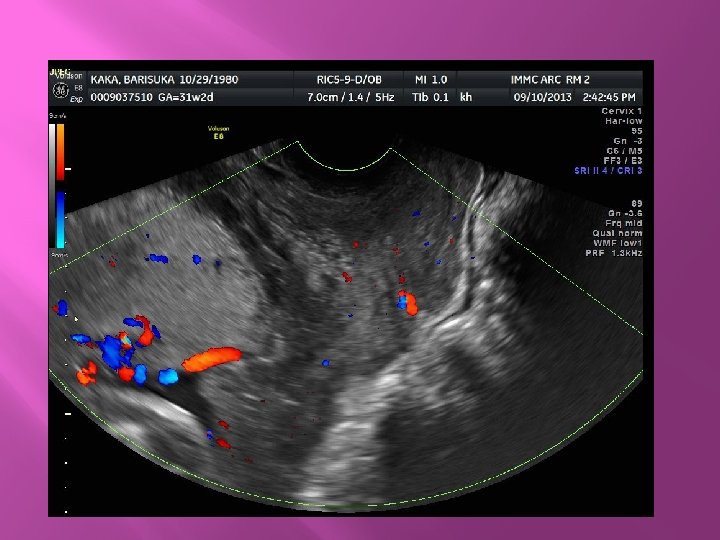
K. B. � � � 32 yo G 3 P 2002 with Di-Di twins and h/o 2 prior c/s Twin A initially noted to have velamentous CI, no vasa previa at 20 wga Presented with VB at 25 w 5 d. Developed/Identified as placenta previa with velamentous CI and vasa previa at 25 w 6 d/c’ed, returned with 2 nd bleed at 26 w 3 d, signed out AMA HD#8 Presented in labor at 32 w 2 d, 2 -3 cm visually dilated with bulging membranes
Pathologic Diagnosis : A. Twin placenta: -Third trimester dichorionic diamniotic twin placenta: -Twin #1 placenta showing intervillous hemorrhage, acute chorioamnionitis and velamentous insertion of cord. -Twin #2 placenta showing velamentous insertion of cord.
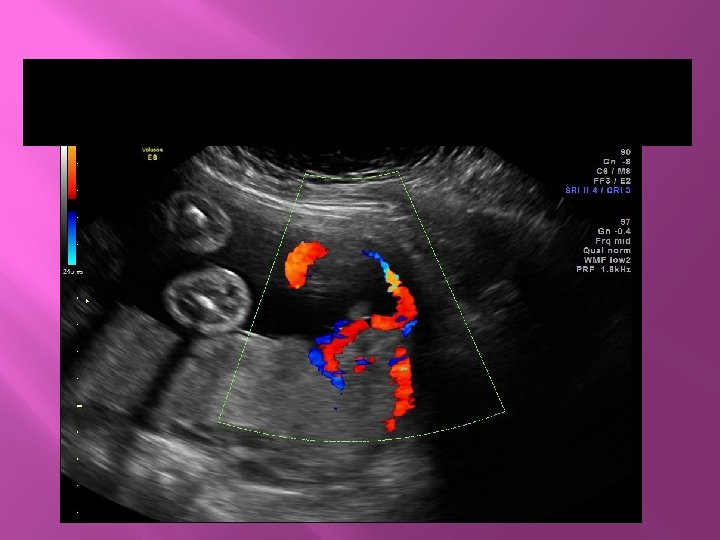
J. B. : � � 20 w US : complete previa with marginal cord insertion Progressed to marginal placenta previa with velamentous cord insertion and vasa previa Plan to admit at 32 wga (tomorrow) Plan for delivery at 34 wga
JB: marginal placenta, velamentous cord insertion
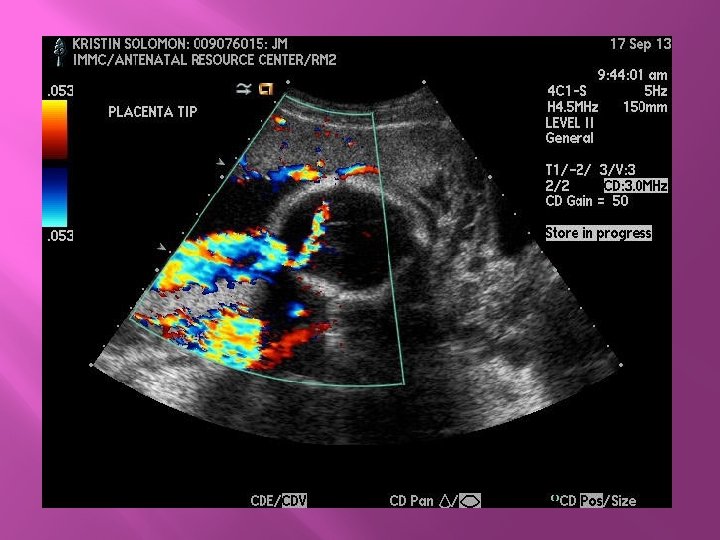
K. S. � � � 33 yo G 1 P 0 with anterior placenta, posterior succenturate lobe, marginal placenta previa, vasa previa. Admitted at 32 wga for surveillance Plan for delivery between 34 and 35 wga
K. D. � � � 41 yo G 1 P 0 with vasa previa, low lying placenta, marginal, possible velamentous C Admit at 32 w 2 d Scheduled delivery at 34 WGA