VALVULAR HEART DISEASE OBJECTIVES To know various risk

VALVULAR HEART DISEASE OBJECTIVES To know various risk factors associated To know pathophysilogy of valvular heart disease 1. 2.
 stenosis i) “narrowing” and failure of forward flow")
VALVULAR HEART DISEASE • Causes a) stenosis i) “narrowing” and failure of forward flow b) insufficiency (regurgitation, incompetence) i) failure of valve to close completely - allowing reverse flow

 Pure i) stenosis or regurgitation d) mixed i) stenosis and regurgitation coexist in")
c) Pure i) stenosis or regurgitation d) mixed i) stenosis and regurgitation coexist in same valve - usually 1 defect predominates e) isolated i) 1 valve f) combined i) more than 1 valve dysfunctional
 flow anomalies through valves produce turbulent flow patterns i) murmurs h) acquired valvular")
g) flow anomalies through valves produce turbulent flow patterns i) murmurs h) acquired valvular heart disease i) see table 12 -7 **ii) students should be able to match various heart valve diseases with both the specific valve involved and whether the disease is a stenosis, regurgitation or both
 most frequent causes: - AS calcification of congenitally deformed valve - AI dilation")
iii) most frequent causes: - AS calcification of congenitally deformed valve - AI dilation of ascending aorta (e. g. , hypertension and aging) - MS RHD - MI mitral valve prolapse (myxomatous degeneration)
 at hinge points of cusps and")
Calcification • valves subjected to repetitive stresses a) at hinge points of cusps and leaflets i) 75 bpm x 60 mins = 4500 bph ii) 4500 bph x 24 hrs = 108, 000 bpd iii) 108, 000 bpd x 365 days = ~40 million bpy iv) 40 million bpy x 75 yrs = 3 billion bp your life !
 deformations during each beat c) pressures on valves in closed phase i) 120")
b) deformations during each beat c) pressures on valves in closed phase i) 120 mm. Hg mitral valve ii) 80 mm. Hg aortic valve d) the factors listed above (a, b, c) contribute to valvular damage seen by calcium deposits (Calcium Phosphate) i) 10 dystrophic calcification (different from atherosclerosis) - calcific AS - mitral annular calcification
 most common of all valvular abnormalities i) geriatric")
• Calcific Aortic Stenosis a) most common of all valvular abnormalities i) geriatric (“wear and tear”) of normal valve or congenital bicuspid aortic valve b) incidence due to age c) incidence of RF in No. America i) < 10% of acquired stenosis d) 6 -7 th decades (bicuspid valve) e) 8 -9 th decades (normal valve) i) “senile calcific aortic stenosis”
 Clinical: i) LV outflow obstruction - LV compensates by LVP to ~ 200")
f) Clinical: i) LV outflow obstruction - LV compensates by LVP to ~ 200 Hg develops - LV concentric hypertrophy (pressure overload !!): CHF - ischemic myocardium - angina may appear - systolic and diastolic impairment (e. g. , syncope) ii) the S & S above indicate decompensation (poor progno. )
 50% die within 5 yrs with angina h) 50% die within")
• g) 50% die within 5 yrs with angina h) 50% die within 2 years with CHF i) patients w/out symptoms have excellent outcome i) symptoms are critical factors in management and outcome !! Calcific stenosis of Congenitally Bicuspid Aortic Valve a) frequency ~ 1. 5% live births b) NOT symptomatic at birth or through early life c) 2 leaflets. 1 is larger
 larger leaflet increases calcification ii) once stenosis occurs, progression is similar to normal")
i) larger leaflet increases calcification ii) once stenosis occurs, progression is similar to normal aortic valve d) bicuspid aortic valves may be acquired (RHD) fused leaflets e) other causes of bicuspid aortic valve incompetence i) aortic dilation ii) cusp prolapse iii) infective endocarditis

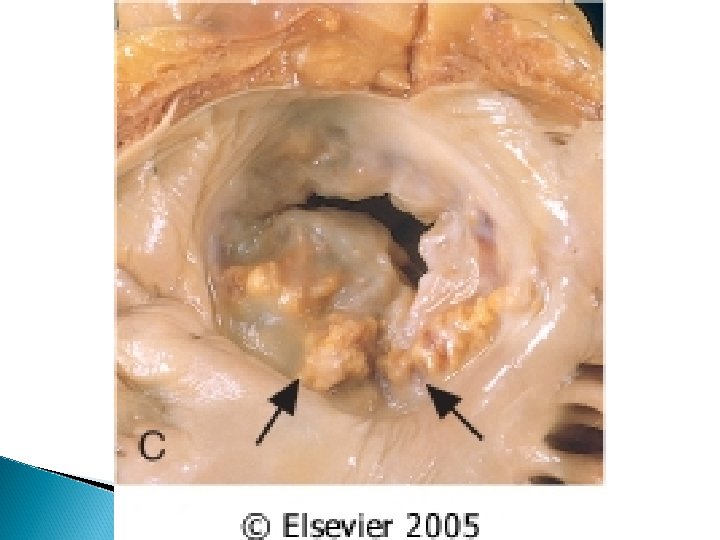
A. Acquired bicuspid aortic valve with secondary calcification. At the center of the conjoined cusp (lower center) are elements of two preexisting cusps, now fused. B. Congenital bicuspid valve. The characteristic raphe of the congenital bicuspid aortic valve appears at the lower portion of the figure. C. Senile type. None of the commissures is fused, but there is a major intrinsic calcification of the three cusps. D. Unicuspid, unicommissural congenital aortic stenosis with secondary calcification. A C B D

Calcific aortic stenosis occurring on a congenitally bicuspid valve. One cusp has a partial fusion at its center, called a raphe (arrow).
 calcific nodules arounf fibrous annular ring of mitral")
• Mitral Annular Calcification a) calcific nodules arounf fibrous annular ring of mitral valve b) usually does not affect valvular function i) rare cases: - stenosis - regurgitation - sudden death (Ca++ dependent) - thrombus formation (stroke) and infections
 women > 60 yrs, LVP, mitral valve prolapse, hypertrophic cardiomyopathy Myxomatous Degeneration of")
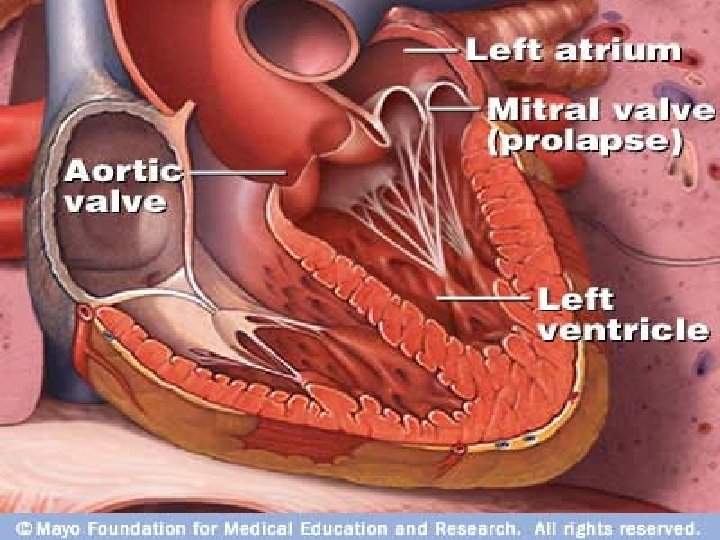
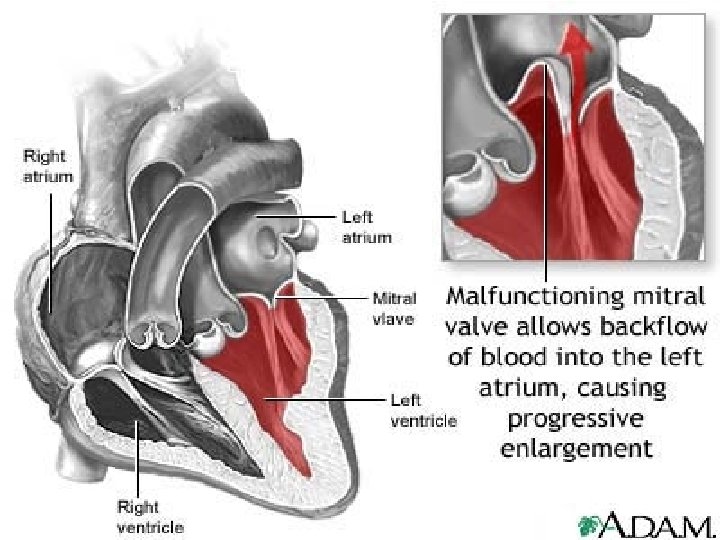
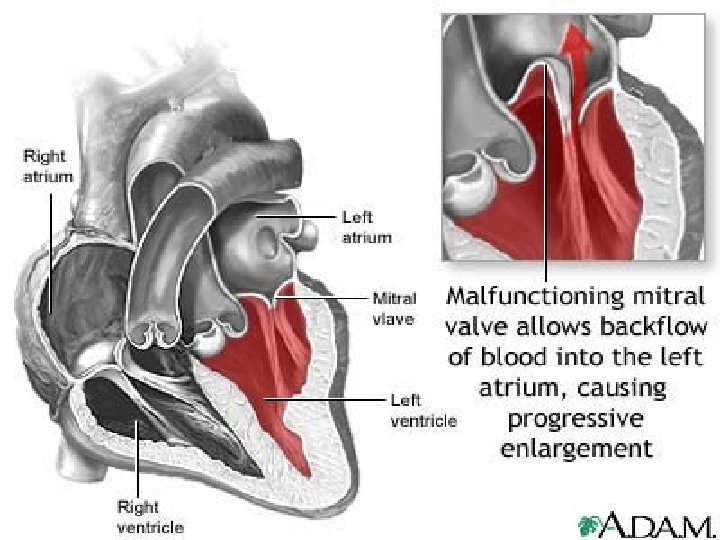
c) women > 60 yrs, LVP, mitral valve prolapse, hypertrophic cardiomyopathy Myxomatous Degeneration of Mitral Valve (Mitral Valve Prolapse) ballooning back during systole one of most common valvular heart diseases a) incidence in women b) usually presents as incidental finding on physical exam • •
 affected leaflets are thickened i) due to mucoid deposits (“Myxomatous”) Myxomatous ii) cords")
c) affected leaflets are thickened i) due to mucoid deposits (“Myxomatous”) Myxomatous ii) cords are usually elongated thinned and often ruptured iii) annular dilation characteristic - leaflets balloon - rare in other mitral insufficiencies iv) thrombi formation - behind ballooned cusps (on leaflets)
 clinical: i) most asymptomatic - midsystolic “click” ii) ~3 % develop complications: -")
d) clinical: i) most asymptomatic - midsystolic “click” ii) ~3 % develop complications: - infective endocarditis - mitral insufficiency (requiring surgery) - stroke - arrhythmias (atria & ventricular - - “sudden death”) iii) if complications surgery
 within weeks following")
Rheumatic Fever and Heart Disease • RF is acute inflammation a) within weeks following group A streptococcal pharyngitis i) cross reaction of Ab directed at M proteins of Strep. proteins with glycoprotein Ag in heart, etc. b) acute carditis (RF) may develop to chronic RHD
 consequence of RF is chronic valvular deformities (fibrosis) i) mitral and aortic -")
c) consequence of RF is chronic valvular deformities (fibrosis) i) mitral and aortic - mainly mitral stenosis - permanent
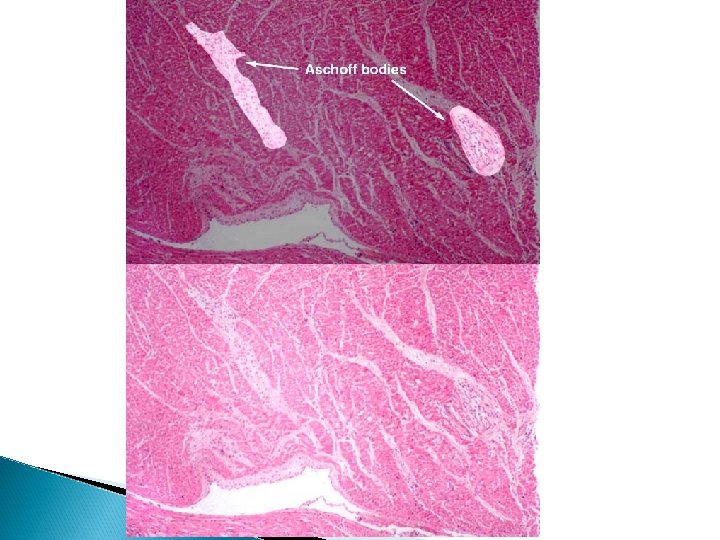
 RF focal inflammatory lesions i) “Aschoff” bodies - swollen eosinophilic")
• Pathology: a) RF focal inflammatory lesions i) “Aschoff” bodies - swollen eosinophilic collegen - found is any layer of the heart (“pancarditis” - in pericardium fibrinous or serofibrinous exudate ii) “Anitschkow” cells - swollen macrophages and/or plasma cells
 RHD – chronic i) organized acute inflammation - fibrosis ii) leaflet thickening iii)")
b) RHD – chronic i) organized acute inflammation - fibrosis ii) leaflet thickening iii) commissure fusion (stenosis) - “buttonhole” or “fishmouth” stenoses iv) cord fusion / thickening v) Aschoff bodies replaced with fibrous scar

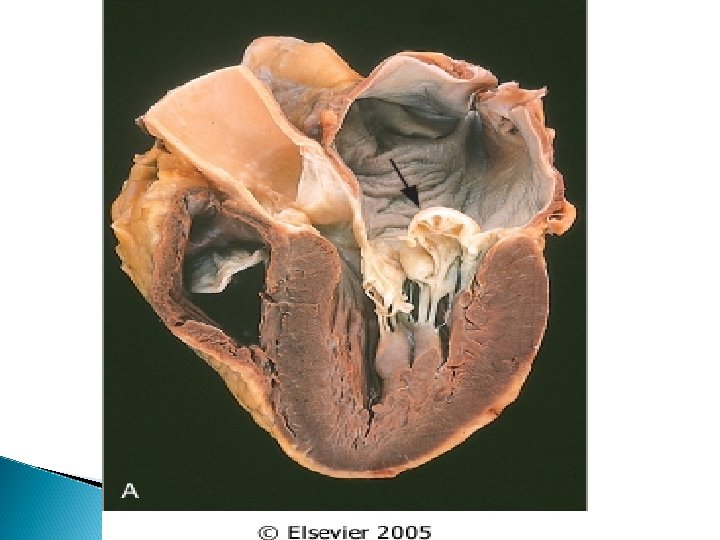
Stenotic mitral Valve seen from left atrium. Both commissures are fused; the cusps Are severely thickened. The left atrium is huge. The valve is both incompetent and stenotic


Opened stenotic mitral valve showing thickening distorted cusps, adherent commissures with calcification and thrombus deposition, and thickening, fusion and shortening of chordae tendinae
 major cause of mitral stenosis - ~ 99% - mitral valve alone ~")
vi) major cause of mitral stenosis - ~ 99% - mitral valve alone ~ 70% - mitral / aortic valve ~ 25% c) etiology unknown i) believed to result from connective tissue defects - in Marfan Syndrome
 migratory polyarthritis i) large joints b) carditis c) s. c.")
• Clinical: a) migratory polyarthritis i) large joints b) carditis c) s. c. nodules d) erythema marginatum e) Chorea movements (CNS) (Sydenham Chorea) (“St. Vitus Dance”)

s. c. nodule
")
Infective Endocarditis • Most cases are bacterial • Classification based on clinical grounds a) acute i) destructive (necrotic, ulcerative) valvular infections ii) highly virulent iii) frequently of healthy valve iv) ~ 50% lethal: days to weeks - despite antibiotics/surgery
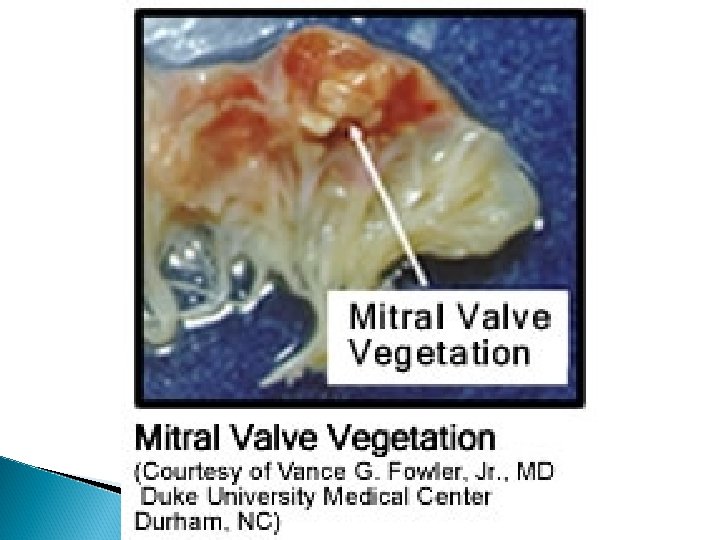
 Subacute i) low virulence ii) recovery with antibiotic Tx iii) vegetative growths show")
b) Subacute i) low virulence ii) recovery with antibiotic Tx iii) vegetative growths show signs of healing • Etiology and Pathogenesis a) may develop on normal valves b) most develop as result of: i) RHD ii) myxomatous mitral valve - most common today
 other factors - calcific stenosis - prosthetic valves - bicuspid aortic valve -")
iii) other factors - calcific stenosis - prosthetic valves - bicuspid aortic valve - immunodeficiency - neutropenia - diabetes - alcohol c) causative organisms i) Strep viridans (50 -60%) - previously damaged native valve
 Staph aureus (10 -20%) - found on skin - virulence - attack normal")
ii) Staph aureus (10 -20%) - found on skin - virulence - attack normal or damaged valves - i. v. drug users !! iii) HACEK group - Haemophilus - Actinobacillus - Cardiobacterium - Eikenella - Kingella
 Prosthetic valves - Staph epidermidis - Staph aureus v) gram (-) bacilli and")
iv) Prosthetic valves - Staph epidermidis - Staph aureus v) gram (-) bacilli and fungi Seeding of blood with microbes main cause a) dental or surgical procedures, etc Aortic and mitral valves most common a) right sided valves in i. v. drug abusers Clinical: a) rapid fever (acute IE) • •
 chills ii) weakness iv) immune mediated GN v) murmurs (~90%) - left side")
i) chills ii) weakness iv) immune mediated GN v) murmurs (~90%) - left side lesions b) subacute (mild or absent To) - fatigue - flu-like symptoms - weight loss
 are normally seen under the")
Common Manifestations of Infective Endocarditis. Splinter hemorrhages (Panel A) are normally seen under the fingernails. Panel B shows conjunctival petechiae. Osler's nodes (Panel C) are tender, subcutaneous nodules, often in the pulp of the digits or thenar eminence. Janeway's lesions (Panel D) are nontender, erythematous, hemorrhagic, or pustular lesions, often on the palms or soles.
 a) sterile, nondestructive b) small masses")
Non Infective Endocarditis • Nonbacterial Thrombotic Endocarditis (NBTE) a) sterile, nondestructive b) small masses of fibrin, platelets, etc. i) on leaflets of cardiac valves c) often seen in debilitated pts i) cancer d) may produce emboli i) stroke in brain, heart, etc.
 frequently occur with DVT and PE i) common origin with hypercoagulable states -")
e) frequently occur with DVT and PE i) common origin with hypercoagulable states - may be related to some underlying disease, such as pancreatic cancer, leukemia, burns and sepsis, DIC - indwelling catheters (SG) induce right valve lesions
 associated with the autoimmune disease SLE i) mitral and")
• Libman-Sacks Disease a) associated with the autoimmune disease SLE i) mitral and aortic valves - mitral more common - underneath valves - on cords b) sterile vegetations c) regurgitation

 associated with systemic syndrome caused by carcinoid tumors")
• Carcinoid Heart Disease a) associated with systemic syndrome caused by carcinoid tumors i) ~ 50% of patients with carcinoid syndrome - flushing of skin - cramps - vomitting - diarrhea i) endocardium ii) valves of right heart (~90%) b) serotonin correlate with severity

Objectives Primary: To assess the risks of adverse outcomes of pregnancy among women with a prosthetic heart valve(s) in the contemporary setting Secondary: To assess the risks and relative risks of adverse outcomes of pregnancy in women with a prosthetic heart valve(s) by prosthesis type or location or both.

Claire M Lawley, Samantha J Lain, Charles S Algert, Jane B Ford, Gemma A Figtree, and Christine L Roberts Syst Rev. 2014 Jan 21; 3: 8. Author Study name , design & LEVEL OF EVIDENCE Claire M Lawley, Samantha J Lain, Charles S Algert, Jane B Ford, Gemma A Figtree, and Christine L Roberts Prosthetic heart valves in pregnancy: a systematic review and meta-analysis protocol AIM Advances in surgical technique, prosthetic heart valve design, and anticoagula tion have contributed to an overall improveme nt in morbidity and mortality in women with heart valve RESULT CONCLUSION Primary outcomes: 1) Maternal mortality 2) Any pregnancy loss a. Any loss of pregnancy, including miscarriage/s tillbirth/termi nation of pregnancy [29] (or as defined by study) 3) Perinatal mortality [ Estimates of the risk of adverse events in recent pregnancies of women with heart valve prosthesis will provide better information for counselling and decision making. Given the improvements in prognosis
 Valvular stenosis refers to one of the following: A. B. C. D.")
MCQs 1) Valvular stenosis refers to one of the following: A. B. C. D. Failure of valve to close completely Reverse blood flow Narrowing and failure of forward flow Mitral valve prolapse
 What is the most frequent cause of Mitral Stenosis: A. B. C.")
2) What is the most frequent cause of Mitral Stenosis: A. B. C. D. Mitral valve prolapse RHD Hypertension and aging Calcification of congenitally deformed valve
 All of the following are common manifestations of infective Endocarditis except: A.")
3) All of the following are common manifestations of infective Endocarditis except: A. Rose spots on abdomen B. Conjunctival petechiae C. Osler’s node D. Janeway’s lesions
 Libman Sacks disease is associated with which disease: A. Rheumatoid Arthritis B.")
4) Libman Sacks disease is associated with which disease: A. Rheumatoid Arthritis B. Infective endocarditis C. SLE D. RHD
 “Aschoff” bodies are seen in A. Rheumatic Fever B. Infective endocarditis C.")
5) “Aschoff” bodies are seen in A. Rheumatic Fever B. Infective endocarditis C. Mitral valve Prolapse D. Carcinoid Heart disease
 Valvular stenosis refers to one of the following: A. B.")
MCQs with Answers 1) Valvular stenosis refers to one of the following: A. B. C. D. Failure of valve to close completely Reverse blood flow Narrowing and failure of forward flow Mitral valve prolapse
 What is the most frequent cause of Mitral Stenosis: A. B. C.")
2) What is the most frequent cause of Mitral Stenosis: A. B. C. D. Mitral valve prolapse RHD Hypertension and aging Calcification of congenitally deformed valve
 All of the following are common manifestations of infective Endocarditis except: A.")
3) All of the following are common manifestations of infective Endocarditis except: A. Rose spots on abdomen B. Conjunctival petechiae C. Osler’s node D. Janeway’s lesions
 Libman Sacks disease is associated with which disease: A. Rheumatoid Arthritis B.")
4) Libman Sacks disease is associated with which disease: A. Rheumatoid Arthritis B. Infective endocarditis C. SLE D. RHD
 “Aschoff” bodies are seen in A. Rheumatic Fever B. Infective endocarditis C.")
5) “Aschoff” bodies are seen in A. Rheumatic Fever B. Infective endocarditis C. Mitral valve Prolapse D. Carcinoid Heart disease

Thank you
- Slides: 60