Valve Surgery V Rohn Valve Surgery History before

Valve Surgery V. Rohn

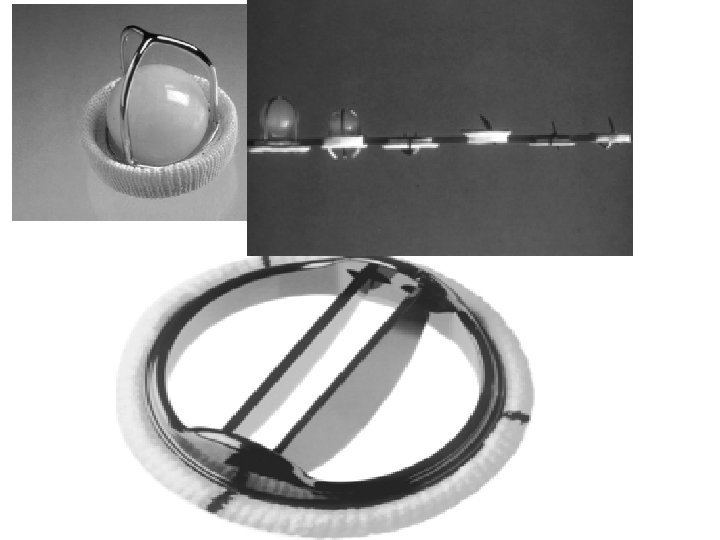
Valve Surgery History before the era of ECC • 1925 – Suttar – first successful digital commisurolysis of mitral valve • 1952 – Hufnagel – first mechanical „ball and cage“ valve implanted to the descending aorta

Valve Surgery History With ECC • 1960 – Harken – aortic valve replacement with the „ball and cage“ valve • 1960 – Starr – replacement of the mitral valve

Valve Surgery • 1962 – Heimbecher – first use of the homograft in the mitral position • 1967 – Ross – autograft of pulmonary valve in the aortic position • 1971 – Carpentier – introduction of „bioprosthesis“, e. g. xenograft as a valve replacement • 1983 – Carpentier –mitral valve plasty (reconstruction) concept
 – rheumatic Symptoms –")
Aortic Valve Stenosis Etiology – degenerative – congenital (bicuspid valve) – rheumatic Symptoms – angina pectoris – syncope – dyspnea

Aortic valve Anatomy
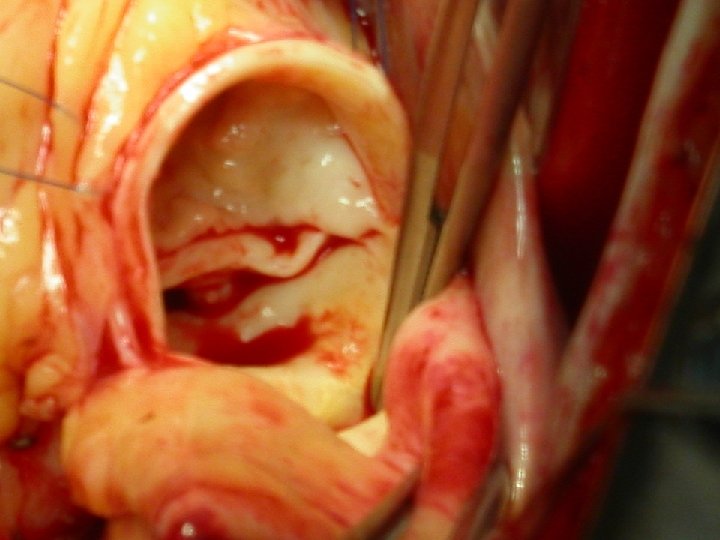

Stenosis of the aortic valve Indications for surgery – symptoms – asymptomatic – AVA 0, 75 cm 2/m 2 and less – pressure gradient 45 – 50 mm. Hg – low EF is not a contraindication Procedure – Aortic valve replacement

Aortic valve regurgitation Etiology – multiple Symptoms – None - very long time – angina pectoris – dyspnea

Aortic valve regurgitation Indication for surgery – Symptoms – or first signs of LV function deterioration • EF < 55 % • Dilatation of LV (EDD > 75 mm, ESD > 50 mm) Procedure – Replacement – Reconstruction

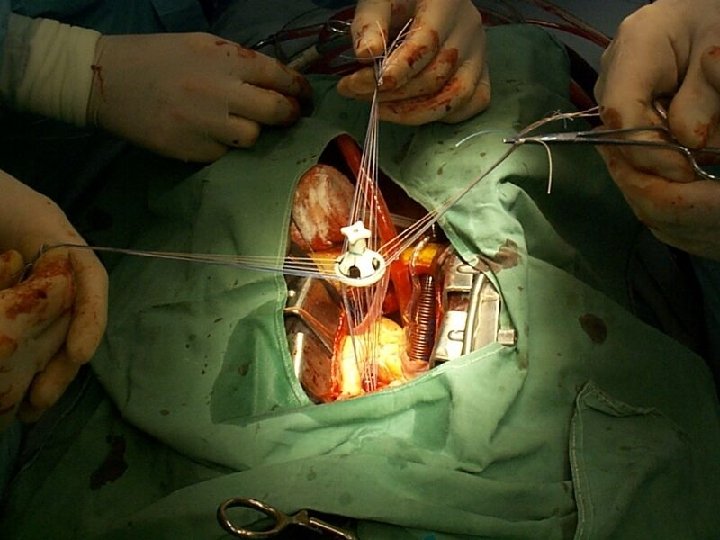
Aortic valve Replacement

Aortic root enlargement – Manougian, Nicks

Allograft, Pulmonary autograft

Percutaneous or transapical implantation – 1965 Davies Lancet 1965; 62: 926— 9.

Endovascular or transapical AVR
 with description of disease mechanisms and repair")
Repair-oriented functional classification of aortic insufficiency (AI) with description of disease mechanisms and repair techniques used Boodhwani M. et al. ; J Thorac Cardiovasc Surg 2009; 137: 286 -294 Copyright © 2009 The American Association for Thoracic Surgery

Aortic Valve Repair

Mitral stenosis Etiology – mostly rheumatic Symptoms – long time asymptomatic – dyspnea – embolization (atrial fib. ) Indication for surgery – valve area less than 0, 8 cm 2/m 2 – pressure gradient above 8 -10 mm. Hg

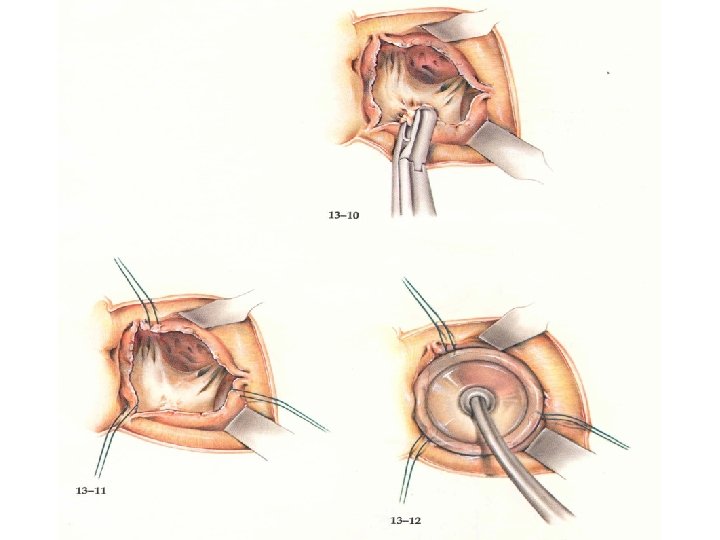
Mitral stenosis ü percutaneous balloon valvuloplasty ü „closed“ commissurotomy ü „open“ commissurotomy ü replacement

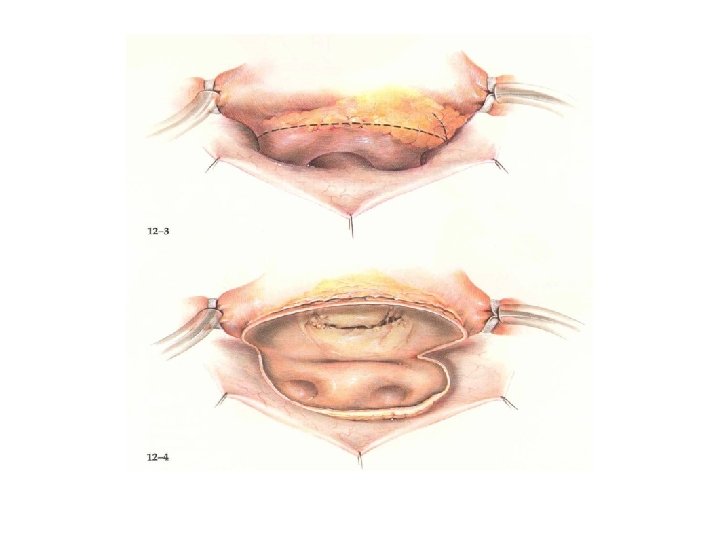
Mitral stenosis – open commissurotomy

Mitral stenosis – closed commissurotomy
 Ischemic symptoms –")
Mitral regurgitation Etiology rheumatic Degenerative mitral regurg. (fibroelastic, myxomatous, Barlow disease) Ischemic symptoms – dyspnea – a. fib. , embolization
 – LV dilatation")
Mitral regurgitation Indication – regurgitation more than 2 -3/5 (echo, ventriculography) – LV dilatation (ESD more than 55 mm) – LV dysfunction, EF decrease Procedure – 90% of degenerative mitral valves are amenable to repair – replacement with preservation of the subvalvular apparatus

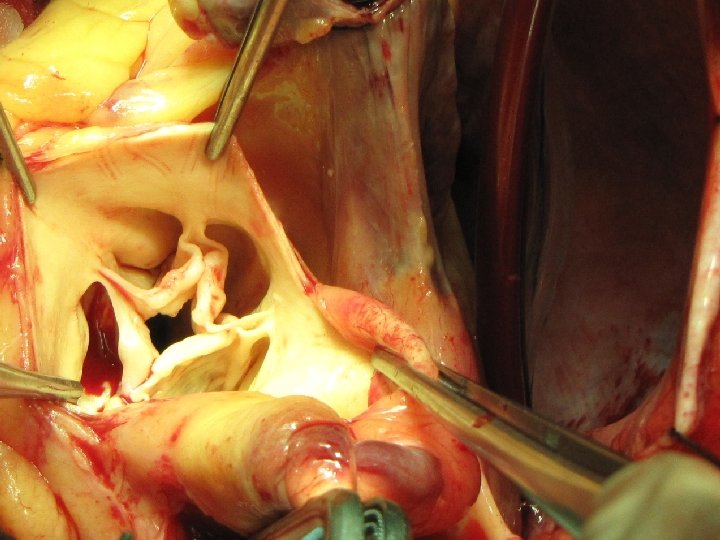
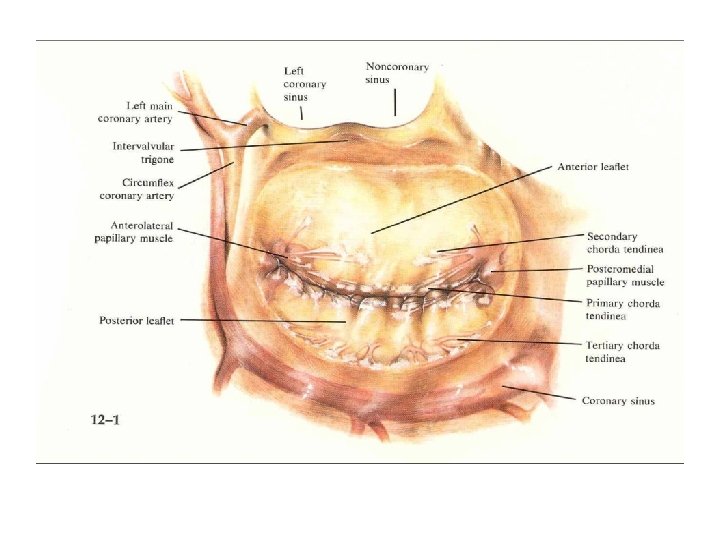
Mitral valve - anatomy

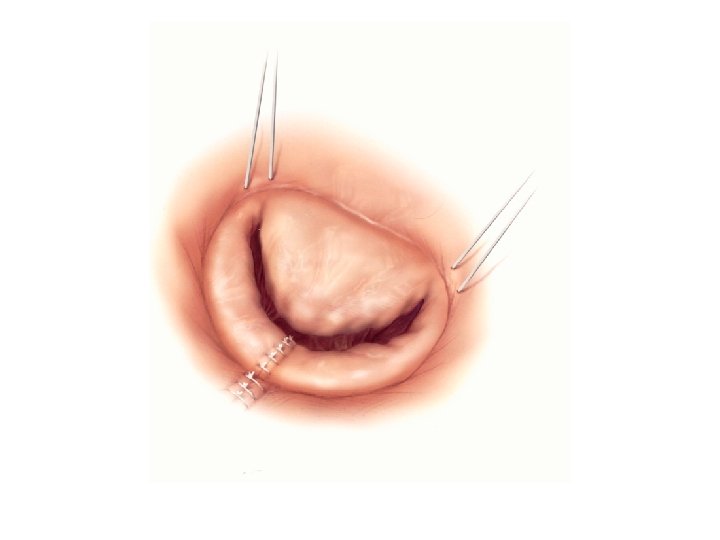
Mitral valve repair – Valve Exposure

Mitral valve repair- quadrangular resection of the posterior leaflet
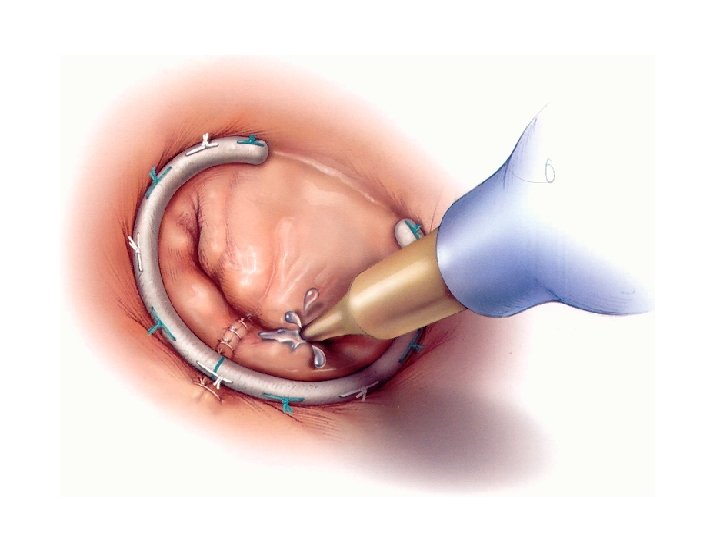

Chordal transfer

Ischemic Mitral Regurgitation

Ischemic Mitral Regurgitation

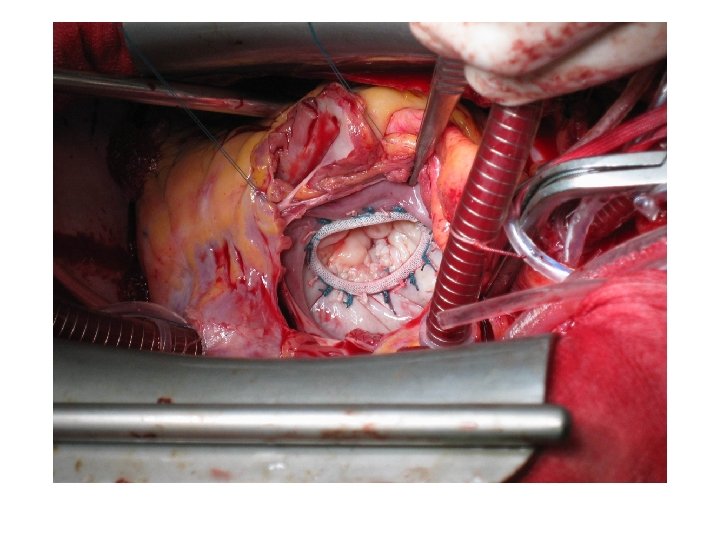
Undersized Annuloplasty

Tricuspid valve

Etiology • Congenital – ASD, VSD, Ebstein disease • pacemaker or automatic internal cardiac defibrillation (AICD) wires • carcinoid • lupus erythematosus, cor pulmonale, inferior myocardial infarction, scleroderma • Functional- secondary to cardiac valvular pathology (mostly mitral valve disease) • up to 20% of patients undergoing mitral valve replacement receive a tricuspid annuloplasty • less than 2% require replacement

Indication to surgery • during left-sided valve surgery when TR annulus is dilated • >21 mm/m 2; >70 mm intra-operatively; >3. 5 cm at TTE • Symptomatic stenosis or regurg.

De Vega plasty

Rings and Bands

Tricuspid valve repalcement

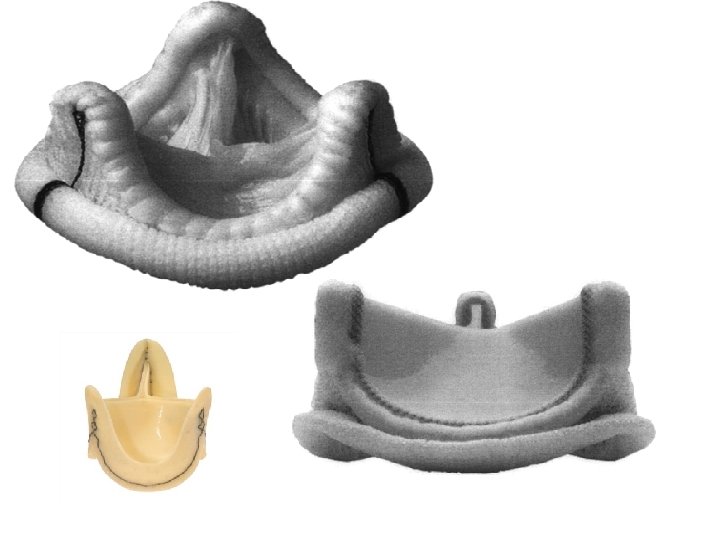
Valve Prosthesis • • biological mechanical homograft autograft

Mechanical vs biological • lifelong anticoagulation therapy • degeneration


ESC guidelines 2007
- Slides: 52