Vaginal Discharge SUDI MAITEH Learning objectives vaginal discharge

Vaginal Discharge SUDI MAITEH

Learning objectives � vaginal discharge definition and what to expect �Medical approach for vaginal discharge complaint �Physiological and pathological causes of abnormal vaginal discharge �Investigations and management of each cause

Vaginal discharge �Vaginal discharge is common to all women �acts as a lubricant for sexual intercourse and as a protective shield to keep infections away (acidic: <4. 5). �it`s a mixture of desquamated epithelial cells �mucus (90% water) �Bacteria (lactobacilli + some anaerobic species ) �Transudate �proteins, polysaccharides, amino acids, enzymes and Igs.

�Normal vaginal discharge : - Consistency : Clear, elastic, mucoid secretions or thick - Transparent or white in color ( yellowish if exposed to air) - Mild odor /odorless - Volume is about 4 ml (can vary from little to quit a lot)
 History taking : Discharge, Timing, duration/ first time and symptoms(pain,")
Medical approach � 1) History taking : Discharge, Timing, duration/ first time and symptoms(pain, itching, fever, bleeding etc. , ) � DDX : cancer, UTI � 2) complete pelvic exam: � External visual exam, Internal visual exam, Pap test , Physical exam � 3) investigations : - Saline Wet Mount - Whiff Test - p. H - Cultures Associated

PHYSIOLOGIC DISCHARGE � is the result of the thin, watery cervical mucus discharge seen with estrogen dominance � Risk factors include chronic anovulatory conditions such as PCOS. � Symptoms: increase in watery vaginal discharge (the most common symptom) with no itching or burning. � Diagnostic tests : 1) Speculum Exam : Vaginal discharge is typically thin and watery. The vaginal epithelium is normal, appearing with no inflammation. Vaginal p. H is normal 2) Wet Mount: absence of WBCs, “clue cells, ” trichomonads, or pseudohyphae. - Management: Steroid contraception with progestins

BACTERIAL VAGINOSIS �Not a true infection, but alteration in concentration of normal vaginal bacteria (anaerobic species >lactobacilli) �Seen commonly in postmenopausal females due to decreased estrogen �Is not a STD but associated with sexual activity. �The most common patient complaint is a fishy odor. Itching and burning are not present.
 1) Speculum Exam : The vaginal discharge")
BACTERIAL VAGINOSIS �Diagnostic tests : (Amsel’s criteria) 1) Speculum Exam : The vaginal discharge is typically thin, grayish-white. No vaginal inflammation is noted. Vaginal p. H is elevated >4. 5. A positive “whiff” test 2) Wet Mount: “clue cells”. WBCs are rarely seen. - Management : Oral or vaginal metronidazole or clindamycin; metronidazole is safe during pregnancy (including first trimester).
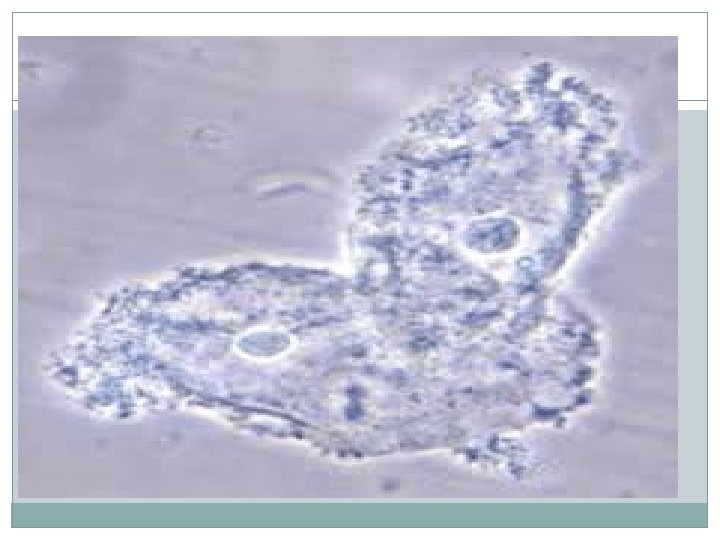

TRICHOMONAS VAGINITIS �is the most common cause of vaginal complaints worldwide. It is sexual transmitted disease �It is caused by a flagellated pear-shaped protozoan that can reside asymptomatically in male seminal fluid. �The most common patient complaint is vaginal discharge associated with itching, burning, and pain with intercourse.
 Speculum Exam : frothy and green. The vaginal")
TRICHOMONAS VAGINITIS �Diagnostic tests : 1) Speculum Exam : frothy and green. The vaginal epithelium is frequently edematous and inflamed. The erythematous cervix may demonstrate the characteristic “strawberry” appearance. Vaginal p. H is elevated >4. 5. 2) Wet Mount: actively motile “trichomonads” on a saline preparation. WBCs are seen. . - Management : Oral metronidazole for both the patient and her sexual partner.
 VAGINITIS �The most common organism is Candida albicans. It is not transmitted")
CANDIDA (YEAST) VAGINITIS �The most common organism is Candida albicans. It is not transmitted sexually �Risk factors include diabetes mellitus, systemic antibiotics, pregnancy, obesity, and decreased immunity. �The most common patient complaint is itching, burning, and pain with intercourse.
 VAGINITIS �Diagnostic tests : 1) Speculum Exam : curdy and white ”cottage")
CANDIDA (YEAST) VAGINITIS �Diagnostic tests : 1) Speculum Exam : curdy and white ”cottage cheese”. The vaginal epithelium is frequently edematous and inflamed. Vaginal p. H is normal <4. 5. 2) Wet Mount: reveals pseudohyphae on a KOH prep. WBCs are frequently seen. - Management : Either a single oral dose of fluconazole or a vaginal “azole” cream.
- Slides: 13