Vaginal breech birth at term the rst stage

Vaginal breech birth at term

• the first stage of labour for women with term pregnancies where the fetus is presenting by the breech. • the knowledge and skills required to e�ectively facilitate planned vaginal breech births at term in both home and hospital settings. • It is important that midwives are conversant with the controversies surrounding the Term Breech find themselves in the situation of diagnosing a breech presentation in transition or the second stage of labour.

• sometimes while attending an out-of-hospital birth. For this reason, all midwives need to have the skills and knowledge to support the woman in this situation, to make decisions, work with the normal physiology of the labour if the birth is proceeding spontaneously, to know how to recognize impending or actual problems, how when to undertake manoeuvres, and/or to transfer the woman to obstetric care in a hospital setting.

Mechanism of right sacro-anterior position • Similar to cephalic presentations that favour the left occipitoanterior position, breech presentations more commonly adopt the right sacro-anterior position, the mechanism of which is described below: • The lie is longitudinal. • The attitude is one of complete flexion. • The presentation is breech. • The position is right sacro-anterior. • The denominator is the sacrum. • The presenting part is the anterior (right) buttock. • The bitrochanteric diameter (10 cm) enters the pelvis in the right oblique diameter of the maternal pelvic brim. • The sacrum points to the right ilio-pectineal eminence.

• Compaction Descent takes place with increasing compaction owing to increased flexion of the limbs. • Internal rotation of the buttocks • The anterior (right) buttock reaches the pelvic floor first and rotates forward of a circle along the left side of the maternal pelvis to lie underneath the symphysis pubis. The bitrochanteric diameter is now in the anterioposterior diameter of the maternal pelvic outlet.

Lateral flexion of the body • The anterior buttock escapes under the symphysis pubis, the posterior buttock sweeps the perineum and the buttocks are born by a movement of lateral flexion: also known as ‘rumping’. • Restitution of the buttocks • The anterior buttock turns slightly to the mother's left side. • Internal rotation of the shoulders • The shoulders enter the brim of the pelvis in the same oblique diameter as the buttocks: namely the right oblique diameter. The anterior shoulder rotates forward of a circle along the left side of the maternal pelvis and escapes under the symphysis pubis; the posterior shoulder sweeps the perineum and the shoulders are born.

• Internal rotation of the head • The fetal head enters the maternal pelvis with the sagittal suture in the transverse diameter of the pelvic brim. The occiput rotates forwards of a circle along the left side of the maternal pelvis and the suboccipital region (nape of the neck) impinges on the undersurface of the symphysis pubis. • External rotation of the head • At the same time the baby's body turns so that it lies parallel with the maternal body. • Birth of the fetal head • The chin, face and sinciput sweep the perineum, and the baby's head is born in a flexed attitude.

Undiagnosed breech presentation • It is still not uncommon for a breech presentation to be discovered for the first time during labour, often towards the end of labour, as the presenting part becomes more easily identified, or in the presence of fresh meconium. If the midwife attends a woman in labour at home with a breech presentation where a hospital birth had initially been planned, it is important to remain calm whilst undertaking a careful assessment of the risk to the woman and baby taking into consideration the parent's wishes before a decision to transfer to hospital is made.

• This will depend on the stage of labour, fetal position and maternal medical and obstetric history. If the woman is nearing the second stage of labour and the labour is progressing well, assistance should be promptly summoned while supporting her to give birth at home. Should a decision be made to transfer to

• hospital, the midwife must alert the hospital of the transfer and ensure that the paramedics are equipped for neonatal resuscitation. The fetal heart and maternal condition should be monitored and recorded throughout the journey to hospital. The midwife must always be prepared for the birth in transit as it may progress more rapidly than initially anticipated.

• In such a situation, the driver should be asked to stop the ambulance in order for the midwife to assist the birth, undertaking any necessary manoeuvres safely. If the baby is likely to be born in transit, it is useful to take a number of towels/blankets to wrap the baby, encouraging skin-to-skin contact and early breast feeding to maintain thermoregulation, i. e. warmth, and reducing the likelihood of hypoglycaemia and hypothermia.

• Types of breech birth • Spontaneous. The birth occurs with little assistance from the attendant. • Assisted breech. The buttocks are born spontaneously, but some assistance is necessary for the birth of extended legs, arms and the head. • Breech extraction. This birth involves manipulating the fetal body by an experienced attendant (usually an obstetrician) in order to hasten the birth of the baby in an emergency situation, such as fetal compromise.

• Position for breech birth • The woman's position can significantly a�ect the physiological labour and birth process and the one that is adopted should ideally be her choice. Many of the existing texts describing vaginal breech births tend to assume the woman should give birth in the hospital environment on the bed in a semi-recumbent, adapted lithotomy position ( • Such a position a�ects the normal physiological process of labour, and may lead to malposition due to the reduction in gravitational force on the fetal mechanisms, consequently increasing the need for the

• midwife to undertake manoeuvres to assist the birth. • While gravity helps to expel the fetus, it is the expulsive contractions and angle of the pelvis that assist in facilitating a physiological breech birth if the woman adopts an upright forwardleaning position. • Little assistance from the midwife is needed if these mechanisms are achieved spontaneously, except in the case of care with the birth of the after-coming head.

• Use of the birth pool is generally not advised, as the buoyancy of the water may work against gravity and thus impede the physiological mechanisms that e�ect a spontaneous breech birth. • A ‘hands o�the breech’ approach is optimal when the woman either adopts a standing or an ‘all-fours’/leaning forwards position.

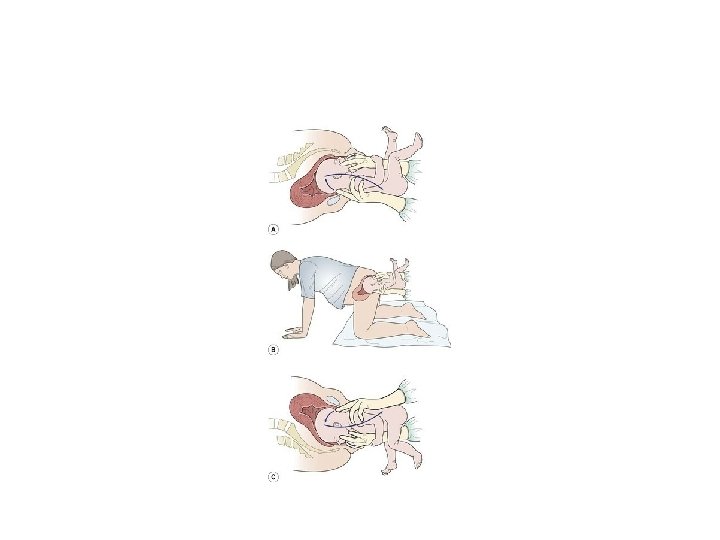
• Where the mother is on all-fours or leans upon the bed/sette or on her birth partner • the baby's trunk descends through the pelvis at 45 o and is able to move more freely around the curve of Carus of the maternal pelvis. • This position provides an excellent view of the birth process and access to the baby's face as it is born over the perineum, as well as ample space for the midwife to undertake any manoeuvres should they be necessary to assist the birth of the baby.


Facilitating a vaginal breech birth in an upright/kneeling position • Breech births can be as physiological as any other vaginal birth and a woman who has chosen to birth vaginally, or discovers in labour that her baby is presenting by the breech, requires calm support from skilled and confident midwives • The importance of not pushing until the cervix has been confirmed as fully dilated should be explained to the woman. • In addition, the woman should be aware that other skilled attendants may need to be called to the birth.

• At the start of the expulsive part of the second stage of labour, the woman tends to make pelvic rocking movements which facilitates the descent of the fetus and corrects positioning for further progress. As the woman commences pushing spontaneously, gradually the anterior buttock should descend, becoming visible at the introitus of the vagina, followed by the baby's anus, genitalia and posterior buttock. The bitrochanteric diameter is then born with lateral flexion, known as ‘rumping’. While this is occurring, the baby's shoulders are entering the oblique diameter of the maternal pelvis.
 and")
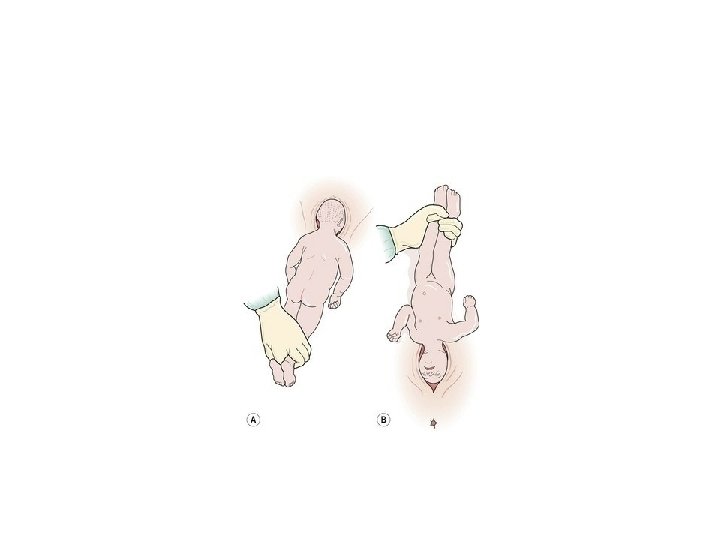
• Descent continues, the baby's thighs, popliteal fossa (back of the knee) and lower legs become visible and the pelvis is eventually born. The baby is then observed to arch its spine backwards, extending its pelvis causing its lower body to curl round the maternal symphysis pubis. • As a result, the tension that this places on the baby's legs assists in their spontaneous release from the introitus, especially when the woman is in an upright, kneeling position, and the baby is born as far as the umbilicus.

• At this point, the woman may spontaneously lower her body so that the baby is sitting on the floor, further encouraging flexion of the baby. It is no longer common practice to pull down a loop of cord to avoid traction of the umbilicus unless there appears to be constriction of the blood vessels as manipulating the cord or stretching it can induce spasm of the vessels.

• With further descent and continued anticlockwise rotation, the head enters the brim of the maternal pelvis as the shoulders rotate in the mid-cavity assisted by the pelvic floor muscles. • emphasizes that this continued rotation of the baby's body assists in bringing the arms down using the pelvic floor muscles in a way that is very similar to the Løvset manoeuvre (used when the birth is delayed should the arms be extended). • The anterior shoulder is released under the symphysis pubis and the posterior shoulder and arm pass over the perineum.

• At this point refers to the baby flexing its legs up towards its abdomen and its arms up towards its shoulders, similar to a sit-up or tummy scrunch. Such a movement, results in the baby flexing its head by bringing its chin down onto its chest and pivoting the occiput on the internal aspect of the symphysis pubis. • This stimulates the woman to lower her body from an upright kneeling position to an all-fours or a knee–chest position, moving her pelvis round the baby's flexing head. • This enables the baby's chin, face, sinciput and head to smoothly pass over the perineum. The midwife is only required to support the baby as the head is spontaneously born.

• If a uterotonic is to be given to the woman as part of the third stage of labour management, it should be withheld until the baby's head is completely born. • The birth of the after-coming head • To avoid any sudden change in fetal intracranial pressure and subsequent cerebral haemorrhage it is vital the head is born in a steady and gradual fashion and often some assistance is given at this point. There are three methods used.

Burns Marshall manoeuvre • This particular manoeuvre facilitates movement of the baby's head through the maternal pelvic outlet, but is only possible when the woman is in a semi-recumbent, adapted lithotomy position. • The baby is allowed to ‘hang’ until the head descends onto the perineum, when after about one to two minutes the nape of the neck becomes visible and the suboccipital region is born. • The baby's ankles are grasped with forefinger between the two, maintaining su�cient traction to prevent the neck from extending and resulting in possible cervical spine fracture

• The feet are taken up through a 180 o arc until the mouth and nose are free of the vulva. This should be undertaken slowly to prevent sudden changes in pressure to the baby's head and undue stretching of the perineum. • The perineum can be guarded to prevent sudden escape of the head • It is imperative that the midwife observes the baby has descended su�ciently to ensure that it is the suboccipital region that pivots under the pubic arch and not the neck to avoid fracture of the cervical vertebra and crushing of the spinal cord.

• Mauriceau–Smellie–Veit manoeuvre • Whilst the baby's head is facilitated through the same 180 o arc as in the Burns Marshall manoeuvre, the Mauriceau–Smellie–Veit manoeuvre provides more control with the birth of the head and places less strain on the baby's back. • This particular manoeuvre can be undertaken in a variety of positions that the woman may adopt for the birth: semi- recumbent, sitting, the adopted lithotomy position or the all-fours position.

• As this manoeuvre facilitates maximum flexion of the baby's head, it can be used to advantage when the head is extended and descent is delayed. • Furthermore, it allows for slow birthing of the baby's head and thus reduces the risk of intracranial haemorrhage.

• In an ‘all-fours’ position, the midwife supports the baby's back over her right arm and flexes the baby's head by tipping the occiput forwards with the middle finger of the right hand by gentle pressure on the baby's malar bones (cheek bones) with the first and ring fingers of the left hand

• It is important that the midwife avoids placing her finger in the baby's mouth to prevent fracture to the jaw or trauma to the mouth and gums, which can result in the baby having di�culties with feeding. The vault of the baby's head should be born slowly and gently to facilitate gradual adaptation of the head to the changing pressures imposed by the birth process. This should be in a downwards direction following the pelvic curve of Carus.

• In the semi-recumbent position, the midwife should support the baby on one of her arms, with her first and ring fingers placed on the baby's malar bones, pulling the jaw down and increasing flexion. The other hand is placed across the baby's shoulders with the midwife's middle finger on the occiput to increase flexion. The outer fingers can apply gentle traction on the baby's shoulders. Maintaining flexion, the head is drawn out of the vagina until the suboccipital region appears and then the baby's head is slowly pivoted gently and slowly upwards around the symphysis pubis following the curve of Carus, delivering the chin and face first

Forceps birth • If an obstetrician is facilitating the vaginal breech birth, forceps may be applied to the after-coming head to ensure the birth is controlled. • Manoeuvres to assist the breech birth • If the midwife uses her professional judgement and decides to undertake a manoeuvre to assist the breech birth, as this will involve making some contact with the woman she must obtain the woman's consent in order to avoid the legal tort of trespass to the person.

• If the fact that the baby is presenting by the breech is known before the onset of labour, it is recommended that the midwife and the woman discuss the reasons for any possible manoeuvres, including their benefit and risks. • The midwife could seek consent to undertake any necessary manoeuvres prior to the labour.

• The following manoeuvres were originally developed to facilitate a breech birth with the woman positioned on the bed, but can be utilized when the woman is on all fours or standing. With the benefits of gravity encouraging descent of the fetus in the later positions, the likelihood of the midwife needing to adopt such measures is reduced. • Nevertheless, as noted above, unexpected breech presentations in late labour still arise, so it is important that the midwife is both aware of, and skilled, in these manoeuvres and maintains her competence in these areas.

• The birth of extended legs • If the fetal legs are not born spontaneously, it is likely they are extended, splinting the baby's body, which impedes lateral flexion of the spine and ultimately delays the birth. • Gentle pressure, can be applied in the popliteal fossa of one of the legs to encourage knee flexion. • This assists in the birth of the leg by sweeping it to the side of the abdomen through abducting the hip.

• This can be repeated for the other leg if necessary. • The knee is a hinge joint which bends in one direction only. • If the knee is pulled forwards from the abdomen, severe injury to the joint can result.

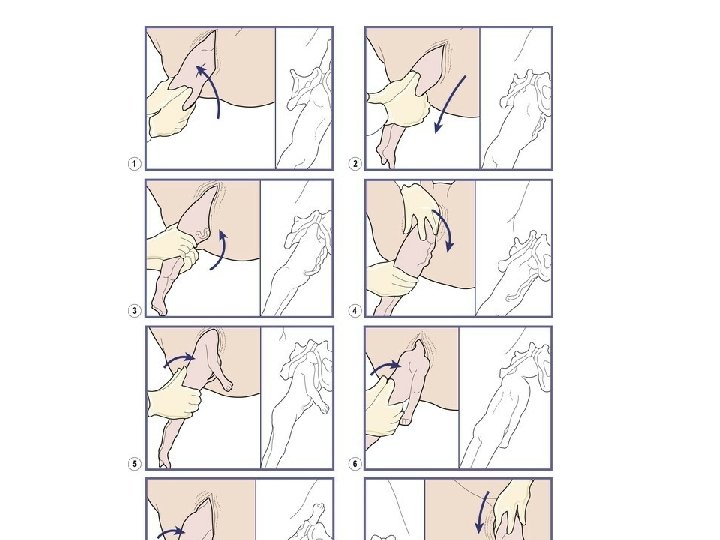
The birth of extended arms: the Løvset manoeuvre • This manoeuvre, which is a combination of rotation and downward traction, is used when the arms fail to appear during the birth of the baby's trunk and chest as a result of them being extended above the head. • If the arms are not released then the birth will be delayed with increasing risk of hypoxia to the baby.

• The baby is held at the iliac crests with thumbs over the sacrum and downward traction is applied whilst the baby is rotated 180° • Care must be taken to always keep the baby's back towards the woman's front, i. e. the baby's abdomen must be uppermost in an all-fours position or the baby's back is uppermost in a semi-recumbent position. • It is important that the baby is not grasped by the flanks or abdomen as this may cause intraabdominal trauma resulting in kidney, liver or spleen injury.

Correct grasp for the Løvset manoeuvre for extended arms.

• To keep the baby's abdomen uppermost should the woman have adopted the all-fours position, if the baby's right arm is extended the baby should be rotated to the right by applying downward traction on the pelvic girdle in order to release the arm. This process is then repeated for the left arm if necessary. • The Løvset manoeuvre creates friction of the baby's posterior arm lying in the sacral curve against the pubic bone as the shoulder becomes anterior, sweeping the arm in front of the face

• The movement enables the shoulders to enter the maternal pelvis in the transverse diameter. The anterior arm is then born and the baby can be rotated back in the opposite direction in order for the other arm to be born. • If the arm is not born spontaneously, it is usual to splint the humerus with two fingers, flex the elbow and sweep the arm across the face and downwards across the baby's chest (‘cat-lick’ manoeuvre).

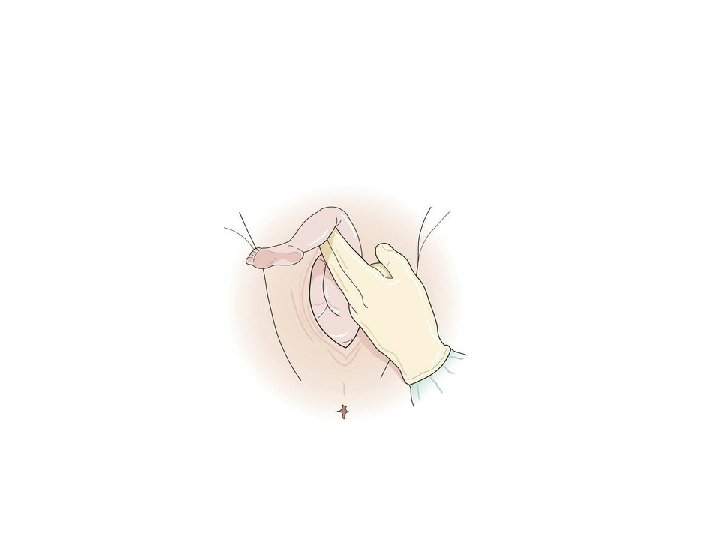
Delay in the birth of the head • If the head is trapped in an incompletely dilated cervix, an air channel can be created to enable the baby to breathe pending intervention. • This is done by inserting two fingers or a Sim's speculum in front of the baby's face and holding the vaginal wall away from the nose. Any mucus is wiped away and the airways are cleared.

• Attempts to release the head from the cervix result in high perinatal morbidity and mortality. • suggested the Mc. Roberts manoeuvre as a method to facilitate the release of the fetal head. • This requires the woman to lie flat on her back, bringing her knees up to her abdomen, and abducting the hips. • More commonly this manoeuvre is used to relieve shoulder dystocia

• Posterior rotation of the occiput is rare and usually results from mismanagement. • If the woman is in a semi-recumbent position, the baby's back should always remain uppermost after the shoulders are born. • To assist the birth should the head be in the occipitoposterior position, the baby's chin and face may pass under the symphysis pubis

• as far as the root of the nose and the baby is then lifed up towards the mother's abdomen to enable the occiput to sweep the perineum. • When facilitating the birth of a woman presenting with a breech at term, there are some important issues for the midwife to consider that are pertinent to the breech scenario.

• Box 17. 4 • Second stage of labour checklist for vaginal breech birth at term – Regular fetal heart monitoring undertaken and documented: Continuous electronic fetal heart monitoring in hospital. Pinard or sonicaid auscultation following every contraction in the second stage at home – Check for cord prolapse if membranes rupture and buttocks are not engaged.

– Check for full dilatation before encouraging the woman to push: The woman may experience a premature urge to push as the fetal body can pass through the cervix prior to full dilatation: the fetal head could become entrapped causing asphyxia increasing perinatal morbidity and mortality. – The umbilical cord may be loosened gently (rarely required): This may be undertaken to prevent constriction of blood vessels as the baby's body is born. In the all-fours position, the condition of the baby can be easily monitored by observing the chest movements.
: To allow")
– Encourage a physiological birth with minimum handling (hands off the breech): To allow the baby to be born by gravity and propulsion and reduce trauma to the baby once the buttocks are distending the vulva. – Vault of the fetal skull should be born slowly: To avoid rapid decompression resulting in intracranial haemorrhage. – Be aware and skilled in manouevres: To assist the birth of the breech if problems arise with fetal descent and to control the birth of the baby's head. – DO NOT PERFORM BREECH EXTRACTION (routine use of manoeuvres/interventions to expedite birth): This can cause delay and obstruction,

• e. g. fetal arms pulled upwards, head extended backwards. – Care of the baby following birth should include: Appropriate resuscitation including suction of the oropharynx and inspection of the vocal cords (if thick meconium), maintaining the baby's body temperature, early feeding and paediatric assessment for signs of birth trauma. – Postnatal examination of the mother: To assess the physical condition, including any birth trauma and discuss the birth and its outcome whilst assessing psychological wellbeing.

– Documentation: Is vitally important throughout the labour and birth, to include specific details of all discussions and referrals and the time they were initiated. – As the breech is born, the time that each stage is reached any manoeuvres undertaken should also be recorded. – Additionally documentation should account for immediate condition of the baby, including any resuscitation measures taken, and the condition of the mother following the birth.

• Potential complications of breech birth • Many of these can be avoided by having an experienced and skilled attendant assisting at the birth. • there were eight intrapartum stillbirths at term.

• Box 17. 5 • Potential complications o f breech birth Potential fetal/neonatal complication Associated cause • Congenital abnormality, e. g. hydrocephaly. A cause for the presentation. • Mechanism of the birth itself poses risks. Congenital dislocation of the hip (↑ frank/extended. Usually a complication of the presentation and not the birth process.
.")
• Fetal asphyxia. • Umbilical cord prolapse (↑ preterm labour/footling breech/ill-fitting presenting part). • Cord compression. • Premature placental separation due to uterine retraction • once the baby's body has been born. Intracranial haemorrhage.

• Rapid decompression of the fetal skull causing tearing of the dura mater lining the brain and other major blood vessels. • Superficial tissue damage/bruising and oedema of baby's genitalia, feet. Fractures of the femur, humerus, clavicle and spine/spinal cord damage. Dislocation of the hip, shoulder, neck. Brachial nerve paralysis
. Pressure on the cervix / prolapsed foot that lies in")
• (Erb's palsy). Pressure on the cervix / prolapsed foot that lies in the vagina or at the vulva for some time. • Incorrect or excessive handling during the birth. Soft tissue damage/rupture to baby's liver, kidneys, spleen and adrenal glands. Abdominal area is roughly squeezed. • Dislocation of fetal jaw /soft tissue damage to mouth and gums/feeding difficulties. Baby's mouth incorrectly being used to create traction rather than the malar bones (cheekbones) in the Mauriceau–Smellie–Veit manoeuvre. • Cold injury/thermal shock and

• hypoglycaemia. • Ambient temperature too cool and baby loses heat during completion of the birth process. • Potential maternal complication. Associated cause. Urethral, vaginal and perineal trauma. Rapid birth of the baby's head. • Effects of anaesthesia (local, regional general), infection, haemorrhage, thromboembolic disorders etc. • Risks of operative procedures. Psychological distress, affecting attachment to baby, feeding difficulties and traumatic stress disorder. • Unexpected vaginal breech birth with lack of time to discuss options.

• Professional responsibilities and term breech birth • the midwife has responsibility to maintain skills in normal physiological birth in relation to breech presentations at term in order to o�er women real choice regarding mode of birth. • . It is therefore essential that these skills are seen as part of the normal physiological birth process rather than viewed as a rare maternity ‘emergency’.

• Record-keeping • . This should include details of any drugs administered, of the duration and progress of labour, of the reason for performing an episiotomy, and of perineal repair. • This information is recorded on the mother's notes (paper and/or computerized) detalis of the baby's condition, including Apgar score, are also recorded.

Diane's birth stor y • The birth of my first baby should have been one of the happiest days of my life. Instead, I felt I had failed; I was mentally and physically traumatized. Five years on, when I was eventually pregnant again, my fears started creeping back, and I considered having a caesarean section. I was referred to the local caseload midwifery team. When my midwife came to visit, I told her that my first birth had leß me traumatized, confused and scared about everything. This was my big turn around: aßer talking to her I realized I did not want a caesarean section, and I started to feel confident about giving birth naturally. • The big day arrived. I was over the moon that I had started my labour naturally. Aßer a

• few hours my midwife came to my house, just to check how everything was going. Eventually, we decided it was time to go to the hospital. When I arrived they organized an epidural for me, which I had discussed, and which was in my birth plan. I was gefling excited, knowing I was going to meet my baby soon. My midwife supported me and encouraged me on everything I decided. She was there for me all the time, keeping me focused and positive about my birth.

• Aßer about 3 hours, I started pushing hard with contractions. The epidural wore o�enough for me to turn around on to my knees with my body upright, and I could feel the baby drop down. I gave it my all for two pushes, and out popped the head. I controlled my breathing, pushing slowly, and my beautiful baby girl came out. The midwife brought her through my legs so I could see her and that's when my husband cut her cord, which was memorable and overwhelming for him. I was the happiest person, I had the biggest smile on my face: to me this was a beautiful birth. Thanks to the wonderful midwives – it goes to show that with the right help and guidance you can overcome your fears and anxieties with positive thinking.
- Slides: 66