v Five billion episodes occurring world wide yearly

개요 v Five billion episodes occurring world wide yearly Guerrant RL et al. Clin Infect Dis 2001; 32: 331 -51

정의 v Diarrhea ‒ Passage of abnormally liquid or unformed stools at an increased frequency ‒ For adults on a typical Western diet, stool weight >200 g/d can generally be considered diarrheal v Pseudodiarrhea ‒ Frequent passage of small volume of stool (rectal urgency: inflammatory bowel syndrome, proctitis) v Fecal continence ‒ Involuntary discharge of rectal contents Harrion’s Internal medicine. 18 ed
 v")
증상의 기간에 따른 정의 v Acute if <2 weeks: viruses and bacteria (90%) v Persistent if 2– 4 weeks: parasite, protozoa, noninfectious etiologies v Chronic if >4 weeks in duration: parasite, protozoa, noninfectious etiologies Harrion’s Internal medicine. 18 ed

국내 감염성 설사의 주 원인균 23, 541명 KCDC. Public Health Wkly Rep 2010; 3: 428 -32

국내 감염성 설사의 역학적 특징 KCDC. Public Health Wkly Rep 2010; 3: 428 -32

국내 감염성 설사의 역학적 특징 5 -9월: 76. 0% 5 -9월: 78. 8% 8 -9월: 65. 6% 5 -9월: 68. 0% 흔한 세균성 설사의 2/3가 여름에 발생!! 바이러스성 설사는 겨울에 호발!! (viral enteritis, winter vomiting disease, intestinal flu) KCDC. Public Health Wkly Rep 2010; 3: 428 -32

감염성 설사 유행의 발생 장소 KCDC. Public Health Wkly Rep 2010; 3: 428 -32
 Inflammatory Diarrhea (invasion or cytotoxin) Proximal small")
발생 기전에 따른 분류 Noninflammatory Diarrhea (enterotoxin) Inflammatory Diarrhea (invasion or cytotoxin) Proximal small bowel Colon or distal small bowel Watery diarrhea Dysentery or Bloody diarrhea No fecal leukocyote Mild to no increase in fecal lactoferrin Fecal polymorhonuclear leukocytes Substantial increase in fecal lactoferrin Vibrio cholerae Enterotoxic E. coli Enteroaggregative E. coli Clostridium perfringens Bacillus cereus Staphylococcus aureus Aeromonas hydrophila Plesiomonas shigelloides Rotavirus, norovirus, enteric adenoviruses Giardia lamblia Cryptosporidium spp. Cyclospora spp. Microsporidia Shigella spp. Salmonella spp. Campylobacter jejuni Enterohemorrhagic E. coli (STEC) Enteroinvasive E. coli Yersinia enterocolitica Listeria monocytogenes Vibrio parahaemolyticus Clostridium difficile A. hydrophilia P. Shigelloides Entamoeba histolytica Klebsiella oxytoca Harrion’s Internal medicine. 18 ed.
")
급성 수양성 설사 v Most bacterial and viral enteropathogens v ETEC (Enterotoxigenic E. coli) v EAEC (Enteroaggressive E. coli) v EIEC (Enteroinvasive E. coli) v Noncholeraic Vibrio v Norovirus Du. Pont HL. Et al. N Engl J Med 2009; 361: 1560 -9
 v Passage of bloody stools: possibility of bacterial cause v Shigella,")
이질 설사 (Dysentery) v Passage of bloody stools: possibility of bacterial cause v Shigella, campylobacter, nontyphoid salmonella, and STEC (EHEC) KCDC. Public Health Wkly Rep 2010; 3: 428 -32
 v 2/3")
Shiga toxin–producing E. coli v Shiga toxin → hemolytic uremic syndrome (HUS) v 2/3 of children with HUS require dialysis v Associated mortality rate is 3 to 5% Du. Pont HL. Et al. N Engl J Med 2009; 361: 1560 -9 Mandell GL et al. Principles and practices of infectious diseases. 7 ed.

E. coli Oligosaccharide : O antigen Fimbriae Flagella: H antigen Mandell GL et al. Principles and practices of infectious diseases. 7 ed.

E. coli Flagella Fimbriae Mandell GL et al. Principles and practices of infectious diseases. 7 ed.

식중독 v Preformed toxin in food is ingested, resulting in an intoxication rather than an enteric infection v Staphylococcus aureus Vomiting within 2 to 7 hours after the ingestion of improperly cooked or stored food containing a heat-stable preformed toxin v Clostridium perfringens Watery diarrhea without vomiting within 8 to 14 hours after the ingestion of contaminated meat, vegetables, or poultry v Bacillus cereus: two toxins

병원내 감염성 설사 “ 3 -day rule” Fecal specimens from patients hospitalized for >3 days should not be submitted for routine stool culture!! Hines J, et al. Clin Infect Dis 1996; 23: 1292 -301

Clostrium difficile infection
 is a unique colonic disease that is acquired")
Definition v Clostridium difficile infection (CDI) is a unique colonic disease that is acquired almost exclusively in association with antimicrobial use and the consequent disruption of the normal colonic flora. v The most commonly diagnosed diarrheal illness acquired in the hospital Harrion’s Internal medicine. 18 ed

Pathogenesis Harrion’s Internal medicine. 18 ed
 B(+): toxin B essential virulence factor v A(+) B(-): real-time toxin")
Pathogenesis v A(-) B(+): toxin B essential virulence factor v A(+) B(-): real-time toxin B assay A (+) B(+) → Diagnostic artifact because of lack of enough sensitive test to detect toxin B!! “Data from studies using molecular disruption of toxin genes isogenic mutants suggest that toxin B is the essential virulence factor” [Harrison’s internal medicine. 18 ed] Harrion’s Internal medicine. 18 ed

Harrion’s Internal medicine. 18 ed

Harrion’s Internal medicine. 18 ed

여행자 설사 v From industrialized regions venture into developing tropical and semitropical areas with reduced levels of personal and food hygiene v Latin America, Africa, and South Asia v E. coli (ETEC, EAEC, etc) v Shigella, salmonella, campylobacter, aeromonas species, noncholeraic vibrios, and plesiomonas Du. Pont HL. Et al. N Engl J Med 2009; 361: 1560 -9

Salmollelosis

Etiology genus Salmonella serotypes S. Typhi and S. Paratyphi restricted to human hosts - enteric (typhoid) fever remaining serotypes (nontyphoidal Salmonella, or NTS) - animals more than 200 serotypes are pathogenic to humans cause gastroenteritis and can be associated with localized infections and/or bacteremia

Etiology Genus salmonella – Species : S. enterica, S. bongori – 6 Subspp : S. enterica subspp. 1 most of human pathogen classification according to serotype Ex) S. enterica subspp. enterica serotype typhimurium S. typhimurium

Samonella enterica Genus Salmonella Species enterica Serotype Typhi Paratyphi A Non-typhoidal salmoneelosis 1. Gastroenteritis 2. Bacteremia and endovascular infection Paratyphi B Typhimurium Enteritidis Enteric (typhoid) fever

Pathogenesis
 decrease stomach acidity ü age of")
Pathogenesis increase susceptibility to Salmonella infection v 1) decrease stomach acidity ü age of <1 year ü antacid ingestion ü achlorhydric disease 2) destruction intestinal integrity ü inflammatory bowel disease ü prior gastrointestinal surgery ü alteration of the intestinal flora by antibiotic administration

Epidemiology • Etiologic agents- S. Typhi and S. Paratyphi serotypes A, B, C • Transmission • Food-borne • Water-borne • sexual (male) • Health care workers

Global distribution
, abdominal pain (only")
Clinical course Enteric fever - fever and abdominal pain Fever (>75%), abdominal pain (only 30– 40%) incubation period for S. Typhi : 10– 14 days (3 to 21 days) inoculum size and the host's health and

Clinical course 국내에서 는 불명열 의 흔한 원인 Most prominent symptom - prolonged fever (38. 8°– 40. 5°C) which can continue for up to 4 weeks if untreated S. Paratyphi A is thought to cause milder disease than S. Typhi, with predominantly gastrointestinal symptoms
 • Gastrointestinal symptoms • chills (35– 45%) Ø anorexia")
Clinical course • headache (80%) • Gastrointestinal symptoms • chills (35– 45%) Ø anorexia (55%) • cough (30%) Ø abdominal pain (30– 40%) • sweating (20– 25%) Ø nausea (18– 24%) • myalgias (20%) Ø vomiting (18%) • malaise (10%) Ø diarrhea (22– 28%) • arthralgia (2– 4%) Ø constipation (13– 16%)

Rose spots

Relative Bradycardia

Relative bradycardia Headach e Hepatosplenomeg aly Cated tongue Abdominal pain Leukopeni Diarrhea or constipation
 l Intestinal perforation (1– 3%) - 3")
Clinical course l Gastrointestinal bleeding (10– 20%) l Intestinal perforation (1– 3%) - 3 rd and 4 th weeks l Neurologic manifestations meningitis, Guillain-Barré syndrome, neuritis, neuropsychiatric symptoms l Rarely, Pancreatitis, pericarditis, IE, orchitis, pneumonia, arthritis l Chronic carriage : women, infants, and persons with biliary abnormalities
, decreased (30%) – Leukocytosis in non-typhoid salmonellosis,")
Laboratory findings Normochromic anemia Leukocyte: normal (70%), decreased (30%) – Leukocytosis in non-typhoid salmonellosis, perforation, focal infection Mild thrombocytopenia, subclinical DIC: common Abnormal LFT Cholesterol : decreased CPK, amylse (50%): common elevated

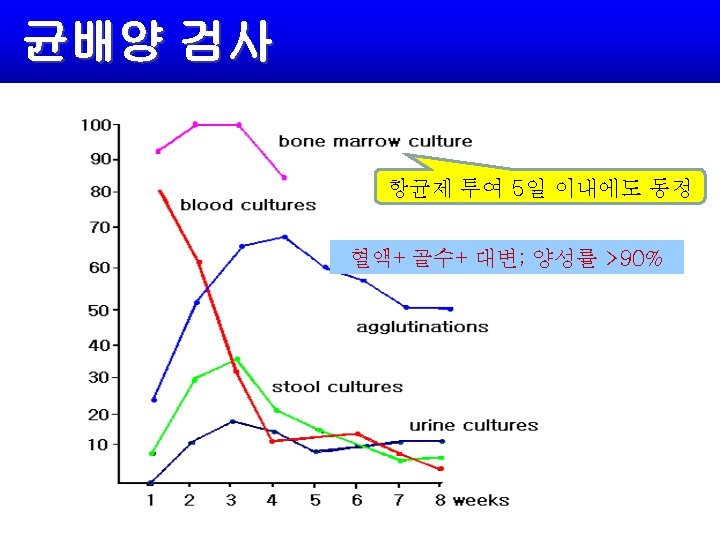
Diagnosis Any febrile traveler returning from a developing country Blood culture: 90% positive during the first week, 50% by the third week Bone marrow culture – Most sensitive in nearly 90% – Used in patients pretreated with antibiotics Stool culture: 30 -40% during the first week, 10% by the 8 th week
 or quinolones : empirical antibiotic")
Treatment Antimicrobial agents – 3 rd. generation cephalosporins (ceftriaxone) or quinolones : empirical antibiotic treatment – Duration for 10 -14 days – Ceftriaxone or cefixime for children – First- and second-generation cephalosporins, aminoglycosides: ineffective Suspected perforation: abdominal radiograph and laparotomy as early as possible

Treatment Relapse: treated the same as for a first attack Chronic fecal carriers (asymptomatic excretion for ≥ 1 y) – Ampicillin or amoxicillin + probenecid; TMP-SMZ; ciprofloxacin for 6 weeks – Chloramphenicol: neither prevent nor effectively treat chronic carrier state – Cholecystectomy to eradicate the carrier state in patients with gallstones or cholecystitis

Prevention Properly managing the water supply and sewage disposal Cooking and refrigerating foods made from animal products Pasteurizing milk and milk products Hand washing before preparing foods and after handling animals and uncooked animal products No vaccine for any salmonella other than S. typhi Prudent use of antimicrobial agents in both humans and animals

Case

Non-Typhoidal Salmonellosis

Etiology In human, enterocolitis is the most common type of diseases. Most common serotype of NTS – S. enteritidis & S. typhimurium

Clinical manifestation Asymptomatic intestinal carrier state – Result from inapparrent infection (m/c form of Salmonella infection) – Usually self-limited Enterocolitis – Incubation period: 12 ~ 48 h – Inflammatory diarrhea – Usually improve over a period of days – Fever lasting no more than 2 -3 d & diarrhea no more

Clinical manifestation Bacteremia – Up to 8% of patients with NTS gastroenteritis – Fever, chills, other symptoms: nonspecific – GI symptoms: unusual – Metastatic infections – Propensity for infection of vascular sites If >50% of 3 or more blood cultures are positive, an endovascular infection should be suspected – Risk factor of endovascular infection Underlying valvular heart disease, Artherosclerosis, prosthetic graft, aneurysm

Diagnosis Isolating organism from stool in enterocolitis, blood in bacteremia, blood and stool in enteric fever, and local site in localized infection Endovascular infection – Echocardigraphy, CT

Treatment Enterocolitis – Fluid & electrolyte replacement – Antimicrobial therapy: not required in majority – Usually self-limited – No effect on clinical course but prolonged excretion in stool – Indicated in infants, the elderly, those with sickle cell disease, lymphoma, leukemia, or other serious diseases who are severely ill and may have bacteremia – Quinolones for 3 -5 days or Amoxicillin, ampicillin, or TMP-SMZ

Treatment Bacteremia & enteric fever – Third-generation cephalosporins, quinolones – Ampicillin, TMP-SMZ, chloramphenicol if susceptible – Without localization of organisms for 2 weeks Carriers – Carriers of salmonellae other than S. typhi : rare – Stools of convalescent carriers spontaneously become negative over a period of weeks to months – Ampicillin + probenecid (6 weeks) or quinolones – Cholecystectomy for gallbladder disease
- Slides: 54