Utilizing the CDC Guideline and Checklist if and

















 § Exercise")






















- Slides: 46
Utilizing the CDC Guideline and Checklist if and when prescribing opioids for chronic pain A guideline for primary providers Jennifer Corder, MD Deputy Health Officer Allegany and Garrett Counties
Objectives Review the evidence base behind the 12 CDC recommendations Examine ways to incorporate the recommendations into your primary care practice Understand the importance of promoting other integrative modalities/therapies in the management of chronic pain
Disclosures None
CDC Guideline for Prescribing Opioids for Chronic Pain- United States, 2016 Primary audience: • PCPs (Physicians, NPs, PAs) treating 18+ with chronic pain >3 mo Secondary audience: • Integrated pain management team members • Behavioral Health, pharmacists and pain management specialists
CDC Guideline inclusions and exclusions • • Including cancer survivors with chronic pain, in remission or under surveillance Excluding those undergoing active cancer treatment, palliative and end-of-life care Excluding opioid prescribing as part of Opioid Use Disorder Excluding <18 population
CDC Guideline scope of advice • • When to initiate or continue Selection, dosage, duration, follow-up and discontinuation Assessing risk and addressing harms Promotes management of chronic pain by the use of integrative modalities
Guideline intentions: Improve communication • Between clinician and patient about risks and benefits of opioid therapy for chronic pain Improve safety and effectiveness Reduce risks associated with long term opioid therapy • Opioid Use Disorder, Overdose and Death
Guideline development: Clinical evidence üGRADE method review of published literature answering to 5 Key Clinical Questions üExpert Opinion üFederal Partner Engagement üStakeholder Comment üConstituent Engagement üPeer Review üPublic Comment üFederal Advisory Committee Review and Recommendation
Guideline development: Contextual evidence Complementary information that assists in translating clinical research findings into recommendations -Non-pharmacologic modalities -Non-opioid pharmacologic options -Clinician values -Patient values -Cost
GRADE approach to evaluating evidence Rating of evidence Randomized controlled trials Observational Clinical experience Type 1 ***** Type 2 **** Type 3 ** *** Type 4 * ** *** Insufficient - - -
Recommendation categories Category A Category B Applies to all persons; most patients should receive the recommended course of action Individual decision making needed; different choices will be appropriate for different patients. Clinicians help patient arrive at a decision consistent with patient values and preferences and specific clinical situations
Key Question #1 What is the effectiveness of long-term opioid therapy versus placebo, no opioid therapy, or non-opioid therapy for long term (> 1 year) outcomes related to pain, function and quality of life? Rating of evidence = Insufficient
Key Question #2 What are the risks of opioids versus placebo or no opioids on abuse, addiction, overdose and other harms? Rating of evidence = Type 3
Key Question #3 What is the comparative effectiveness of different opioid dosing strategies? Rating of evidence = Type 4
Key Question #4 What is the accuracy of instruments for predicting risk of opioid OD, addiction, abuse or misuse? What is the effectiveness of risk mitigation strategies including but not limited to : -opioid management plans -patient education -urine drug testing -PDMP data -pill counts Rating of evidence = Type 3
Key Question #5 What are the effects of prescribing opioid therapy versus not prescribing opioid therapy for acute pain on long-term use? Rating of evidence = Type 3
Contextual evidence summary Effectiveness of non-pharmacologic Effectiveness of non-opioid pharmacologic treatments Benefits and harms of opioid therapy Clinician and patient values and preferences Costs of therapy and risk mitigation
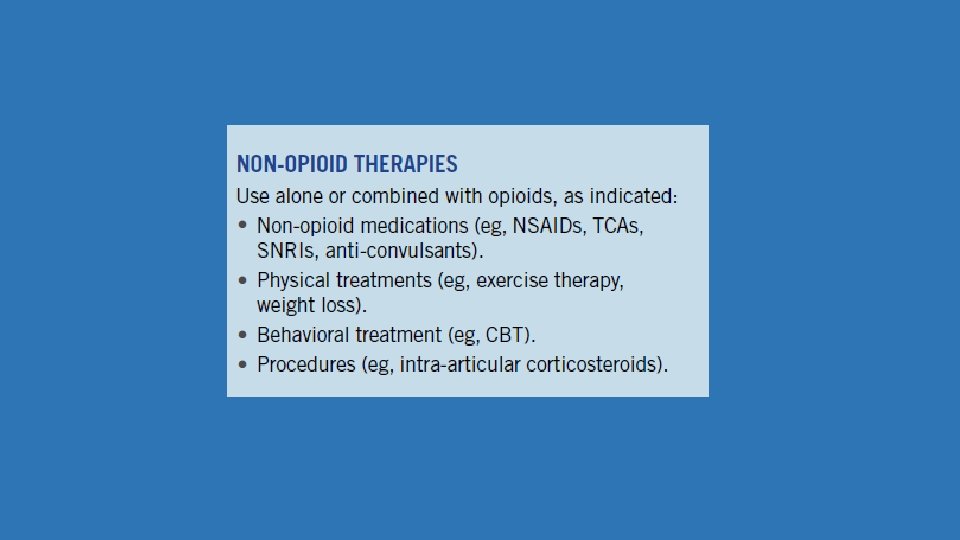
Effectiveness of non-pharmacologic and non-opioid pharmacologic treatments § Cognitive behavioral therapy (CBT) § Exercise therapy § Multimodal approaches § NSAIDS § Acetaminophen § COX-2 inhibitors § Selected anticonvulsants § Selected antidepressants § Interventional approaches
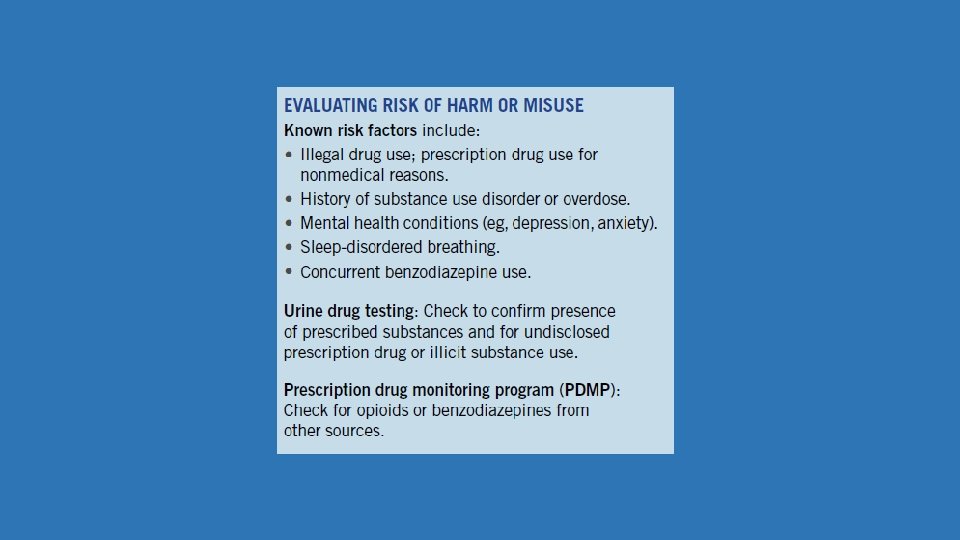
Benefits and harms of prescribing opioid therapy Risk factors for harm Modifiable Un-modifiable LA/ER Sleep disordered breathing Time-scheduled Renal or hepatic insufficiency Methadone Elderly High dose Pregnant Co-prescribing with benzodiazepines Depression/mental illness Multiple prescribers/pharmacies Substance use disorder
Clinician and patient values and preferences Clinicians have reported lack of confidence in: Ability to prescribe opioids safely Predicting and detecting opioid prescription abuse Discussing abuse with their patients Clinicians underutilize: PDMP data Urine drug testing Opioid treatment agreements Patients: Are often unaware what an opioid is Experience side effects commonly Side effects (rather than pain relief) explain most variations in patient preferences
Costs of opioid therapy and risk mitigation • Non-medical use: 53. 4 billion • Abuse, dependence and misuse: 55. 7 billion • OD related costs: 20. 4 billion • Outpatient Rx opioids: 9 billion (2012) Lower cost therapies • Acetaminophen, NSAIDS & TCAs • Massage therapy, yoga, physical therapy, cognitive behavioral therapy (CBT), acupuncture • Urine drug testing including confirmatory testing: $211 -363 per test
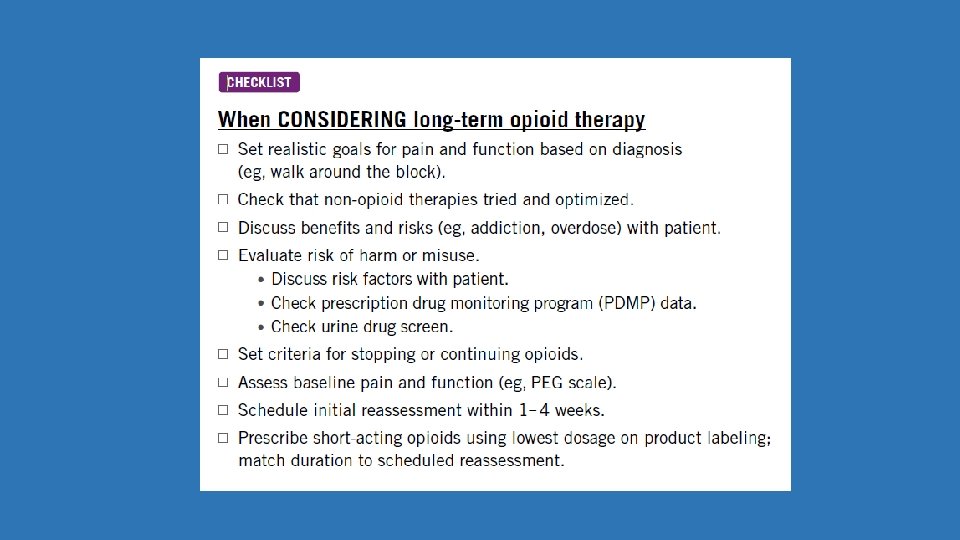
Recommendations: When to initiate or continue opioids for chronic pain 1. Non-pharmacologic and non-opioid pharmacologic therapies preferred for chronic pain. (A, 3) 2. Establish pain-related and function-related treatment goals before using opioids for chronic pain. (A, 4) 3. Discuss known risks and realistic benefits of chronic opioid therapy before starting and periodically during treatment. (A, 3)
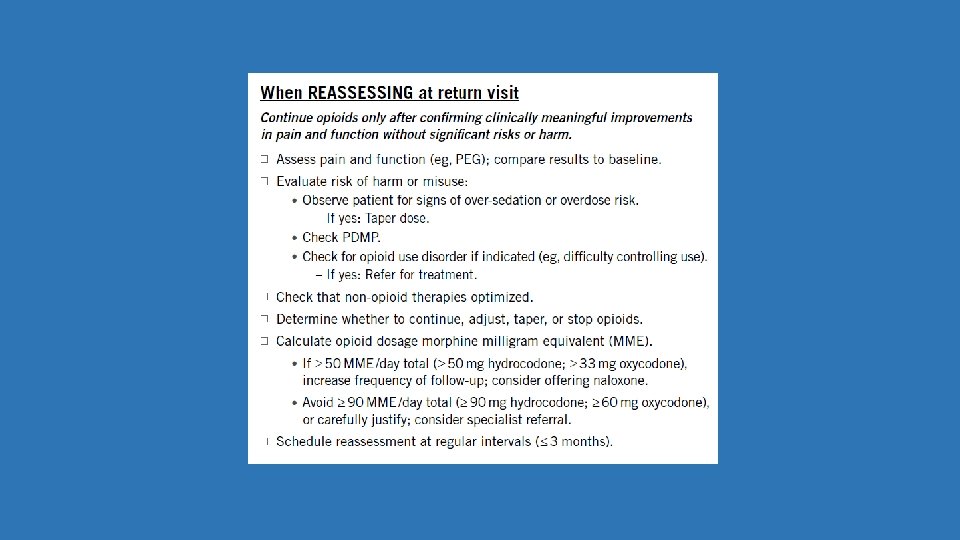
Recommendations: Opioid selection, dosage, duration, follow-up and discontinuation 4. When starting opioids for chronic pain, avoid ER/LA formulations. (A, 4) 5. Prescribe the lowest effective dosage. >50 MME/day triggers reassessment of benefits and risks. Avoid or carefully justify >90 MME/day. (A, 3) 6. Treat acute pain with lowest effective dose of short acting opioid. <3 days often enough. >7 days rarely needed. (A, 4) 7. Evaluate benefits and harms within 1 -4 weeks of starting opioid therapy for chronic pain and on dose escalation; evaluate <Q 3 months when on continued therapy. Benefits must outweigh harms. (A, 4)
Recommendations: Assessing risk and addressing harms of opioid use 8. Evaluate risk factors for opioid related harms (before starting and periodically during). Consider naloxone. (A, 4) 9. Review PDMP data before starting and periodically during. (A, 4) 10. Use urine drug testing before starting and at least annually during opioid use for chronic pain. (B, 4) 11. Avoid prescribing opioids and benzodiazepines concurrently. (A, 3) 12. Offer MAT and behavioral therapies to anyone with Opioid Use Disorder. (A, 2)
Clinical Tool
Krebs, E. E. , Lorenz, K. A. , Bair, M. J. , Damush, T. M. , Wu, J. , Sutherland, J. M. , Asch S, Kroenke, K. (2009). Development and Initial Validation of the PEG, a Three-item Scale Assessing Pain Intensity and Interference. Journal of General Internal Medicine, 24(6), 733– 738. http: //doi. org/10. 1007/s 11606 -009 -0981 -1
Modality Acupuncture Physical therapy Biofeedback Exercise Yoga/Tai chi Mindfulness-based Massage Weight loss Low back pain Migraine Osteoarthritis Fibromyalgia Rheumatoid arthritis Neck pain
Prescribers: Effective July 1, 2018: ü New treatment episode prescribing opioid or benzodiazepine ü At least Q 90 days thereafter for duration of treatment ü Exceptions ü < 3 day supply ü Cancer tx or cancer-related pain ü Patient in inpatient hospital or hospice ü Patient residing in nursing or other assisted living facility ü To treat or prevent acute pain for <14 days following surgery with general anesthesia, fracture, significant trauma or childbirth ü If specific med listed by Secretary in low abuse potential list ü Electrical or technological issues
Primary care prescriber responsibilities Meet patient expectations Treat pain Prevent misuse and diversion
Primary care prescriber responsibilities Manage chronic pain Utilize integrative modalities
Primary care prescriber responsibilities Reduce misuse and diversion use PDMP & UDTs & contracts
Primary care prescriber responsibilities Reframe and meet patient expectations
Opioids for chronic pain Non-opioid choices for chronic pain Nonpharmacologic Non-opioid pharmacologic Poor evidence and safety profile Better evidence and safety profile
Criticisms of the CDC Guideline: Ø Low quality evidence base excluding studies measuring outcomes from 3 mo-1 year Ø May lead to under-treatment, stigmatization, and marginalization of patients using opioids appropriately Ø Insurance limitations for non-pharmacologic treatments Rebuttal from the CDC: “Whereas the benefits of opioids for chronic pain remain uncertain, the risks of addiction and overdose are clear. ”
Core take home CDC messages: ü Non-opioid therapy is preferred for chronic pain outside the context of active cancer, palliative, or end-of-life care. ü When opioids are used, the lowest possible effective dose should be prescribed to reduce the risks of opioid use disorder and overdose. ü Clinicians should exercise caution when prescribing opioids and should monitor all patients closely.
Need more knowledge about complementary and integrative modalities? Allegany College of Maryland Integrative Health Curriculum and special programs Community college affiliate of the Center for Mind-Body Medicine
References Major source providing non-opioid pain modalities: NIH Chronic Pain In Depth https: //nccih. nih. gov/health/pain/chronic. htm#hed 3 CDC Guideline Resources: Non-opioid treatments https: //www. cdc. gov/drugoverdose/prescribing/clinical-tools. html Other Sources: 1. Mayo Clinics: Evidence-Based Evaluation of Complementary Health Approaches for Pain Management in the United States http: //www. mayoclinicproceedings. org/article/S 0025 -6196(16)30317 -2/pdf 2. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016 https: //www. cdc. gov/mmwr/volumes/65/rr/pdfs/rr 6501 e 1. pdf 3. Harvard Medical School Special Report: Pain Relief, Natural and alternative remedies without drugs or surgery 4. ACPA Resource Guide to Chronic Pain Management https: //theacpa. org/uploads/documents/ACPA_Resource_Guide_2017. pdf
Jennifer Corder, MD Jennifer. corder@maryland. gov