Using PRIMIS tools for quality improvement Myth buster

Using PRIMIS tools for quality improvement

Myth buster • • • PINCER is pharmacist-led information technology intervention for reducing clinically important errors in general practice prescribing (PINCER) PINCER is not a clinical audit and it is not a reactive alert tool used to periodically identify patients at risk so that remedial action can be taken. PINCER should not be time consuming for general practice (on average 60 patients per practice were identified in the East Midlands PINCER 3 study, only 50% needed an intervention) PINCER does not need to be ran on a monthly basis – clinical audit and findings from the initial study suggest 6 month review to capture improvement and/or new patient incidents The PINCER audit tool will remain stable over the next 12 months despite changes to general practice systems and coding structures PRIMIS are the technical authors of PINCER (clinical and technical specifications remain the intellectual property of the Uo. N), no other provider of ‘PINCER’ indicators have been validated against the official evidence based set

Information governance assurances O PRIMIS is not involved in the collection of patient identifiable data O PRIMIS does not share data with the pharmaceutical industry or other commercial organisations ü Practices can choose to submit practice level data to PRIMIS for the online comparative analysis service (CHART Online) – data collection agreements exist – the practice controls access ü Use of practice data is governed by our Security and Confidentiality of Practice Data Policy ü Anyone wishing to use PRIMIS tools must register as a member of the PRIMIS Hub - use of that data is governed by our Privacy Policy ü PRIMIS is certified to BSI ISO 9001 and BSI ISO/IEC 27001 and achieved compliance with the NHS IG Toolkit

What we will cover Identifying the need for change Planning the change Reflection and evaluation

Change management is…. …a structured approach to moving individuals, teams, and organisations from the current state to a new state

Managing change in general practice Change necessitated by circumstances is acceptable in general practice Often evidence is not available for required change Change based on fashion is less acceptable than that based on sound evidence Imposed change is more acceptable if it is expressed in terms of outcome rather than detailed behaviour The positive way to deal with imposed change is to create a sense of ownership of the change within the practice Scott and Marinker (1993), Change and Teamwork in Primary Care (BMJ)

Where to start? What do we want to achieve with this change? Why do we need to change? What Who Why How Who is affected by the change and how will they react? How much can we achieve ourselves and what do we need help with?

The PINCER Intervention in practice Run PINCER audits Implemen tation Action planning RCA Meet with practice

PINCER 3 Eleven specific audits developed by PRIMIS in partnership with the University of Nottingham which allows GP practices to easily interrogate their clinical data and identify patients who are potentially at risk of harm through prescribing errors or inadequate drug monitoring. Supports the Can reduce Provides multi. NICE ‘Medicines unnecessary and dimensional data Optimisation inappropriate from patient to Clinical treatment and practice, local Guidelines’ hospital and national published in admissions levels March 2015 Identifies patients who may not have received the necessary monitoring or investigations and require a medication review

OUTCOME: GI BLEED Query 1: In a patient aged ≥ 65 years prescription of an oral NSAID without coprescription of an ulcer-healing drug Query 2: Prescription of an oral NSAID, without co-prescription of an ulcer-healing drug, to a patient with a history of peptic ulceration Query 3: Prescription of an antiplatelet drug to a patient with previous peptic ulcer or GI bleed without co-prescription of an ulcer-healing drug Query 4: Prescription of warfarin or a New oral anti-coagulant (NOAC) and an antiplatelet in combination without co-prescription of an ulcer-healing drug Query 5: Prescription of warfarin or NOAC in combination with an oral NSAID Query 6: Prescription of aspirin in combination with another antiplatelet drug without co -prescription of an ulcer-healing drug

OUTCOME: EXACERBATION OF ASTHMA Query 1: Prescription of a non-selective beta-blocker to a patient with asthma Query 2: Prescription of a long-acting beta-2 agonist inhaler (excluding combination products containing inhaled corticosteroid) to a patient with asthma who is not also prescribed an inhaled corticosteroid OUTCOME: HEART FAILURE Query 1: Prescription of an oral NSAID to a patient with heart failure OUTCOME: STROKE Query 1: Prescription of antipsychotics for >6 weeks in a patient aged ≥ 65 years with dementia but not psychosis OUTCOME: KIDNEY INJURY Query 1: Prescription of an oral NSAID to a patient with chronic renal failure with an e. GFR <45

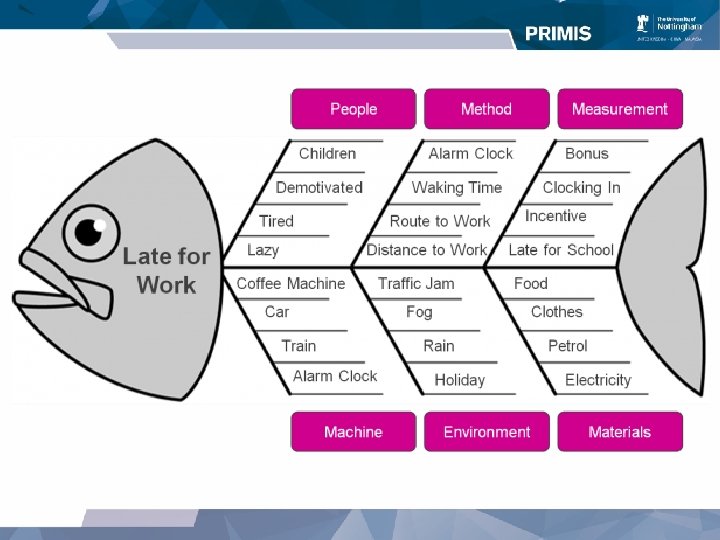
Identifying the need for change Planning the change Reflection and evaluation ROOT CAUSE ANALYSIS

What is Root Cause Analysis? Is the identification of the ‘vital few’ causes that have a material impact on the outputs of a process Analysis is used to identify areas for change and to develop recommendations which deliver safer care for patients.

RCA investigation process • Gathering and mapping information • Identifying care and service delivery problems • Analysing to identify contributory factors and root causes • Generating solutions • Log, audit and learn • NPSA standard • http: //www. nrls. npsa. nhs. uk/resources/coll ections/root-cause-analysis/

Neglect and wilful misconduct are a rare source of harm Person centred System centred Problem Careless individuals Poor design Focus Blame System Solution Remove individual Change system Improving the reliability and safety of healthcare systems is a critical task

How can we identify the underlying system failures which contribute to an adverse event or near miss? 1. Need to identify the root cause. This is a factor: Ø which significantly contributes to an adverse event Ø if resolved will eradicate, or significantly contribute to the resolution of, the identified problem to which it is attached 2. Undertake a root cause analysis (RCA) Ø structured investigation that aims to identify the true cause(s) of a problem, and the actions necessary to eliminate it (Anderson & Fagerhaug 2000)

Applying the principles of RCA 1. Identify incident 2. Gather information 3. Identify and prioritise problems 4. Explore problems Focus on systems not individuals 5. Identify quality and safety improvements 6. Implement action plan and share learning SHARE LEARNING

Think about how you would apply the principles of root cause analysis when delivering the PINCER intervention You have identified 5 people in one practice that are prescribed an antipsychotic for more than six weeks in patients without a read code of psychosis. All have been prescribed in dementia and none of them have entries mentioning the drug in the notes in the last three months

Identifying the need for change Planning the change Reflection and evaluation CONDUCTING A GOOD PRACTICE MEETING

Resistance to change Resistance is a resource Communication is key You can change the change Objections can be valid Acknowledging history reduces resistance

Overcome resistance Awareness and education Participation and negotiation Produce and share an action plan Identify key personnel and responsibilities

The PINCER Intervention in practice Run PINCER audits Implemen tation Action planning RCA Meet with practice
 • Outlining the project •")
Engagement meeting • Foster key relationships (PM, lead GP) • Outlining the project • Defining your role – what you will and won’t do • Updating morbidity codes and test results? • Intervening with at risk patients • Improving systems to prevent future problems • Providing regular feedback

Identifying the need for change • Define the vision of where you want to be • Identifying driving forces and resisting forces (force field analysis) • Recognise the potential hazards of taking a ‘no change’ option (doom scenario) • Define best practice • Carry out SWOT analysis
 • Reach agreement")
Feedback meeting • Present the data • Discuss your findings (RCA) • Reach agreement on actions to be taken and by whom

Effective communication Be specific Have clear reasons and benefits of change Be honest Communication style – be creative Manage any issues as they occur Review progress – does this meet the vision Two-way communication

SWOT analysis Strengths Weaknesses Opportunities Threats

What would you consider? Prescription of aspirin in combination with another antiplatelet drug without co-prescription of an ulcer-healing drug Number of patients =8 Most have a fixed term for the second antiplatelet Second antiplatelet has always been started in hospital

Who adds to repeat and do they know to consider gastro-protection Process for addition Use of computer system and software available Education – prescriber and patient 2 antiplatelets Feedback to hospital Stop dates for antiplatelets to directions Review dates for PPI to directions 30

What would you consider? Prescription of an oral NSAID, without co-prescription of an ulcer-healing drug, to a patient with a history of peptic ulceration Number of patients =8 5 of which have a PPI on repeat but have not collected regularly enough to be adherent

Medication review Repeat issue by reception team Process for identifying nonadherence in the practice NSAID and nonadherence to PPI What to do if PPI declined Clear directions on the medication Education of the patient 32

Identifying the need for change Planning the change ACTION PLANNING Reflection and evaluation

Action planning

Mo. SCo. W Must Do Should Do Could Do Won’t Do

Responsibility charting GPs Practice Manager District Nurses Practice Nurses Computer Operator Reception Patients Install computerised appointments system A R I S R S I Enter hospital discharge summaries onto computer C S I I R R -- Attend clinical coding training R R R -- Audit data quality levels C S -- C R I --

S Specific Be precise about what you want to achieve M Measurable Quantify your objectives. How will you know you have achieved what you set out to achieve A Achievable For an objective to motivate people, it should be challenging but not impossible or too difficult R Relevant Is it going to improve your situation? List the benefits that would be achieved by putting this plan into practice T Timely Give a time frame for achieving the objectives

Action planning Actions Step 1. Identify budget available for new scanner Step 2. Identify the requirements of the new scanner to assist with purchasing the correct model Step 3. Research available scanner models to meet budget and specification needed Person Responsible Start Date Expected Resources Completion Date Actual Completion Date Practice Manager Anna Smith 3 rd March 5 th March 12 month practice financial plan 4 th March Admin Manager Jenny Williams 3 rd March 6 th March Time to consult admin staff, Access to the 12 month I. T plan 6 th March Internet access Budget details Specification requirements Time for research 14 th March I. T Manager John Croft 6 th March 13 th March

Take action! Avoid failure Monitor progress Evaluate

Lessons learned report 40

Tips for success Keep people informed Don’t rely on messages being cascaded Monitor progress Celebrate successes along the way Communicate clearly and positively

Summary • This work provides a real opportunity to improve patient safety in your general practice • The indicators provide a “litmus test” into the practice prescribing • Demonstrating success will, however, be more of a challenge • Key issues include: Ø involving all members of the practice Ø taking a systems approach to patient safety Ø agreeing on a plan of action and executing this

Identifying the need for change Planning the change Reflection and evaluation INTRODUCTION TO QUALITY IMPROVEMENT

GP Pharmacists and QI As experts in medicine and their use, pharmacists play a crucial role in quality improvement programmes The Royal Pharmaceutical Society actively promote the potential benefit that pharmacists can bring to primary care patients particularly in relation to long term condition management By integrating pharmacist skills with those of the rest of the general practice team they can work together to improve patient outcomes and safety PRIMIS tools provide a solid foundation for a quality improvement programme that can be instigated and led by Pharmacists CPPE – Centre for Pharmacy Postgraduate Education

Going forward Quality improvement cycle

Integrating clinical audit with other quality improvement activity • QOF • Raising dissatisfaction • Locally Commissioned Services • QIPP agenda • CQINN scheme • Pathway and service redesign • Care Quality Commission • • • Right. Care inidcators and pathways CCG Assurance Framework Revalidation

Clinical audit

How do you carry out practice-wide audit and involve the whole team (both clinical and non clinical staff)? • Hold regular multi-disciplinary meetings within the practice • Develop a practice audit plan as a team. Consider including carers and patients in those discussions • Involve the team at all stages, particularly decision making

How do you communicate the findings of multi-disciplinary audit to facilitate change of practice? • Ensure the team understands why (and where) change is necessary • Present audit results in an innovative and challenging way may improve buy-in • Fostering a collaborative approach will ensure that the team is interested in the results and willing to make the changes

Can several practices conduct collaborative audit? • YES! • Again, everyone should follow the same audit cycle • Ensure each practice team has clear roles and responsibilities and, crucially, that they reflect on their own practice as part of the audit • Take account of issues of data collection, data sharing and data analysis

PDSA Cycle • Plan next steps – action plan! • Implement proposed changes • Repeat cycle - assess effectiveness • Review the results in CHART - what do they mean? • Lessons learnt • Plan the work – which practice/system/ tool? ACT PLAN STUDY DO • Install CHART • Run the MIQUEST data searches

The change agent does not have to walk on water but… should be patient, persistent, honest, trustworthy, reliable, positive, enthusiastic, co-operative, confident (but not arrogant) a good listener, observant (of the feeling and behaviours of others), flexible, resourceful, difficult to intimidate, willing to take risks and accept challenge and be able to handle organisational politics. And they should have a sense of humour, a sense of perspective and be able to admit ignorance and ask for help when appropriate…” Hutton D. W. , The Change Agents’ Handbook. (1994)

Questions
- Slides: 53