Use of Steroids and IVIG in ICU Dr
















 –")


")























 – Confer")
 – Confer")

















 – No salt retaining")













:")











- Slides: 93
Use of Steroids and IVIG in ICU Dr. Natalie Leung Dr. KC Chan Feb 2008
IVIG in ICU
Immunoglobulins • Normal serum contains Ig. G, Ig. M, and Ig. A – They are referred to as natural antibodies because they are induced without deliberate immunization and are independent of antigenic exposure. – They are considered key to the immunoregulatory effects of immune globulin in immune-mediated disorders
IVIG • “IV”: intravenous • “IG”: immunoglobulin
IVIG • It is made from large volumes of human plasma by a method: ethanol fractionation – Developed by E. J. Cohn in early 1940 s. • It is a plasma product formed by taking antibodies from about 3000 -10000 donors and mixing them together.
• IVIG contains: – Sterile, purified immunoglobulin • 95% unmodified Ig. G • Only trace amounts of Ig. A or Ig. M – Cytokines – Sucrose/ glucose/ some other sugar (based on the manufacturers)
2 preparations of IVIg • Monoclonal – Contain a single class of Ig directed against a single epitope of those present upon a target molecule – Predominantly Ig. G • Polycloclonal – Containing Igs directed against multiple epitopes of the target substance – Ig. G, Ig. M and minor amounts of Ig. A
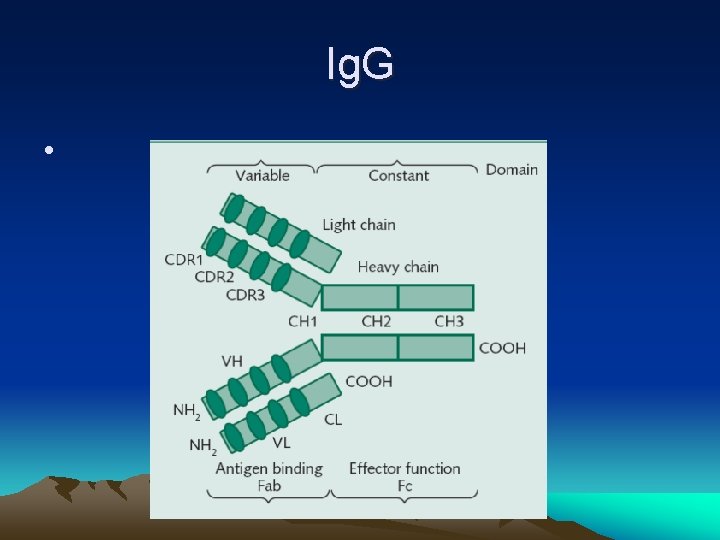
Ig. G • Ig. G – A Y shaped antibodies – It has intact Fc-dependent effector functions
Ig. G • The Fc region of Ig. G facilitates interaction with and signaling through Fc receptors on – phagocytes, B cells, and other cells and with Fc-binding plasma proteins (e. g. components of the complement system).
• Thus, peripheral tissues that are defended mainly by Ig. A antibodies are not fully protected by IVIG – Eyes, lungs, gut and urinary tract
Possible mechanisms
IVIG: how does it work? • Boost the patient’s immunological capacilities – In those with immune deficiency – IVIG maintain adequate antibodies levels to confer a passive immunity – In sepsis – Increase opsonization and phagocytosis – Activation of complement system
• Blunt an autoimmune response – Downregulation of the inflammatory response by the reduction of TNF and other inflammatory mediators – Increase the soluble receptors for a number of cytokines – E. g. Guillian-Barre Syndrome, Myasthenia gravis
Why is IVIG so expensive? • It is a plasma product formed by taking antibodies from about 3000 -10000 donors. • Ethanol fractionation is used as an initial step in the preparation of pooled immunoglobulin • In the past, infusion resulted in a variety of serious reactions – Need IM injection – More painful and slow absorption
Why is IVIG so expensive? • Several steps were added to the fractionation process – Extraction at low p. H – Addition of sugars to decrease aggregation • Lots of procedures are needed to remove – Protein contaminants (to get the concentrated Ig. G) – Deactivate viral contaminants • E. g. HBV, HIV
How long does it take to have effect? • Patients may see a response in their disease within 24 - 48 hrs after IVIG infusion – Some patients will have to wait 3 -4 weeks to see an effect after IVIG – In a few no effect may be seen following IVIG infusion. • If 4 -5 cycles of IVIG do not show any response then try a different approach like plasmapheresis, cytotoxic or immune suppressants.
Side effects • Occur in <5% of patients • Common side effects (self-limited) – Fever, chlls – Myalgias, nausea and dyspnoea • Headache (more common in females with history of Migraines/ SLE, often 24 -72 hrs after infusion) • Flu like symptoms – Fatigue • Changes in BP • Aseptic meningitis
Side effects • If this happen – Slow down the infusion rate – Pre-medicate the patient with antihistamines and steroid
Other rare adverse reactions • Acute renal failure – From 6/1985 - 11/1988, the US FDA received 120 reports worldwide – It occurs with the sucrose-stablized formulation, but not with the D-sorbitol-stabilized formulation (? Related to the sugar content and osmolality) – The FDA’s Center for Biologics Evaluation and Research (CBER) • Issued a warning about ARF and administration of IVIG • Ensure patients are adequately hydrated
Other rare adverse reactions • The FDA’s Center for Biologics Evaluation and Research (CBER) list the risk factors: – – – – Pre-existing renal insufficiency DM Age > 65 Volume depletion Sepsis Paraproteinaemia Anyone who may be on concomitant nephrotoxic drugs
Other rare adverse reactions • Thromboembolic events – E. g. CVA/ TIA/ MI/ DVT – Risk factors: underlying HT, hypercholesterolemia, AF, history of vascular disease Vucic S Thromboembolic complications of intravenous immunoglobulin treatment. Eur Neurol. 2004; 52(3): 141 -4
Indication • It have been used in a wide variety of diseases – Primary and secondary immune deficiency states – Autoimmune disorders – Prophylaxis and treatment of bacterial and viral infection
6 conditions approved by FDA • • • ITP Primary immunodeficiencies Chronic B-cell lymphocytic leukemia Pediatric HIV infection Kawasaki syndrome Haematopoietic stem cell transplantation in patients older than 20 years
Other applications have been outlined by National Guideline Clearinghouse • Hematology – Aplastic anaemia – Autoimmune hemolytic anaemia – Immune-mediated neutropenia…. . • Infectious diseases – Conditions in which acquiring an infectious disease could be deleterious include low birth weight (ie, <1500 g), solid organ transplantation, surgery, trauma, burns, and HIV infection.
Other applications have been outlined by National Guideline Clearinghouse • Neurology – Guillain-Barre Syndrome – Myasthenia gravis – Chronic inflammatory demyelinating polyneuropathy – Lamber-Eaton syndrome – Multiple sclerosis
Other applications have been outlined by National Guideline Clearinghouse • Obstetrics – Recurrent pregnancy loss • Respiratory – Asthma – Chronic chest symptoms • Rheumatology – – RA SLE Dermatomyositis, polymyositis Systemic vasculitis
New uses of IVIG: lung disease Role of Intravenous Immunoglobulin in Severe Steroid-Dependent Asthma Haque S, Boyce N, Thien FC, O'Hehir RE, Douglass J Intern Med J. 2003; 33: 341 -344 • Severe Steroid-Dependent Asthma – IVIG provides a potentially important adjunctive therapy in severe steroiddependent asthma, reducing steroid requirement and decreasing hospital admissions, but not improving lung function.
• Possible mechanisms: – The mechanism by which steroid resistance develops may be related to elevated levels of interleukin 2 (IL-2) and IL-4 in the airways of steroid-resistant asthmatic patients – IVIG reduces production of IL-2 and IL-4 by T cells
New uses of IVIG: Sepsis • Polyclonal IVIG are used off-label either to prevent sepsis in at-risk subjects, or to treat existing sepsis and its consequences
Mechanisms of IVIG in sepsis 1. Blunt the perpetuation of the initial response by attenuating the trigger substances – Igs against antigens present on the surface of the infecting microorganisms – It also against the factors that are released when the organisms is killed by antibiotics • E. g. endotoxin, peptidoglycans
2. Inactivate the sepsis mediators that are produced and released in a more advanced phase of the inflammatory process, or – Neutralize the receptors for these substances located on the cell surface
Why polyclonal IVIG is used? • In septic patients, elevated levels of Ig. M anti-endotoxin antibodies are associated with a better outcome – Thus, Ig. M-enriched polyclonal IVIG can replicate this effect.
Why polyclonal IVIG is used?
New uses of IVIG: Sepsis Polyclonal Intravenous Immunoglobulin for the Treatment of Severe Sepsis and Septic Shock in Critically Ill Adults: A Systematic Review and Meta-analysis Kevin B. Laupland Critical Care Medicine 2007; 35(12): 2686 -2692 • To assess whether adjunctive therapy with IVIG reduces mortality among critically ill adults with severe sepsis and septic shock
• 14 RCTs published between 1988 - 2006 were included
• Characteristics of the included studies Of the 14 included studies -13 had intention-to-treat data available - only nine had adequately concealed randomization - in six the investigators and patients were blinded to treatment allocation
• The effect of IVIG on mortality in adult patients with severe sepsis or septic shock was 0. 66 (95% confidence interval [CI] 0. 53 -0. 83; p <. 0005), indicating a significant reduction in mortality for patients treated with IVIG
• This systematic review demonstrated a significant reduction in mortality in critically ill adult patients with severe sepsis and septic shock treated with polyclonal IVIG
In pediatric patients • In streptococcal toxic shock syndrome – Use of polyclonoal IVIG 2 g/kg for 1 -2 doses has been associated with reduced mortality – In vitro evidence suggests that IVIG can neutralize superantigen activity • Premature newborns of low birth weight – Relatives insufficiency of humoral immunity – Susceptible to sepsis – Meta-analysis showed the use of IVIG marginal reduction of early-onset neonatal sepsis
Cost • IVIG – US$8050 - $40000/ life saved • Activated protein C – US$140000 - $170000/ life saved • PYNEH: $ 650/ 3 g
Steroid in ICU
• What is steroid? • Common use of steroid • Use of steroid in critically ill patients
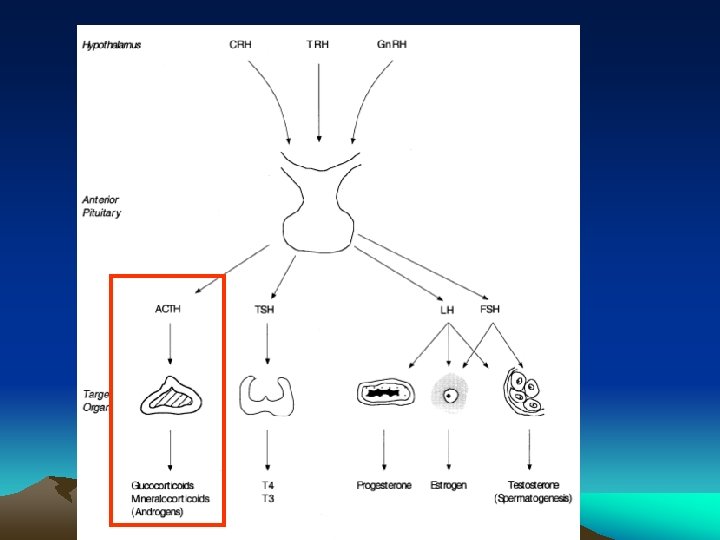
What is steroid? • Steroids are small molecules which are synthesized in 3 places in human body Pituitary gld: smallest amount Adrenal cortex Testicles in men Ovaries in women
• Function of adrenal steroids – Influence metabolism (carbohydrate/ protein/ lipid) – Confer resistance to stress – Regulation of immune function – Modulation of the immune response – Electrolyte and water balance (sodium retention/ alter potassium excretion in urine)
• Function of adrenal steroids – Influence metabolism (carbohydrate/ protein/ lipid) – Confer resistance to stress – Regulation of immune function – Modulation of the immune response – Electrolyte and water balance (sodium retention/ alter potassium excretion in urine) Glucocorticoid effect Mineralocorticoid effect
Synthetic steroid • Replacment therapy – Low dosage – Adrenal insufficiency • Treatment of non-endocrine diseases – Higher doses
Synthetic steroid • ~2000 years ago, some Roman evaporated the urine and get the powdered residue. – These residue contains high level of testosterone/ estrogen – The patients would experience some +ve and –ve effects of these powdered residue
• The Father of modern steroid – Adolf Winhaus – Synthesized the first steroid – Received the 1927 Nobel Prize in Chemistry
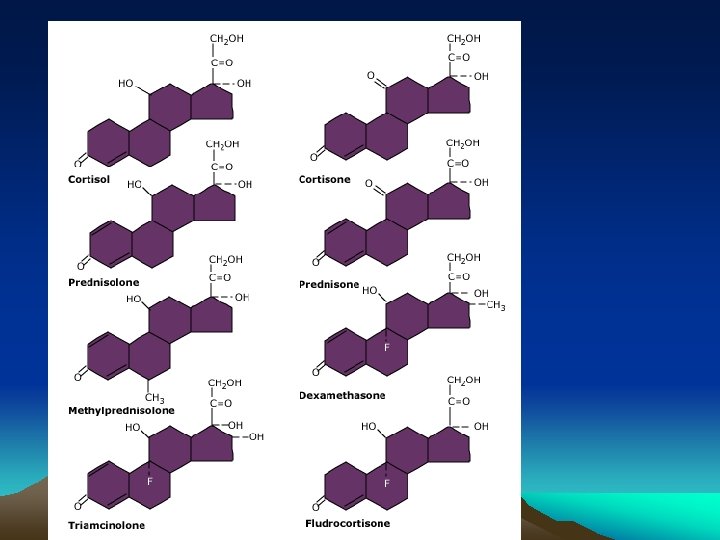
Synthetic steroids • Glucocorticoids – Prednisolone/ prednisone – Methylprednisolone – Dexamethasone – Betamethasone – triamcinolone • Mineralocorticoid – Aldosterone – Fludrocortisone
• Basic glucocorticoid structure Increase glucocorticoid and / or mineralocorticoid activity
Pharmacokinetics • Most cortisol in serum is bound to proteins – Corticosteroid-binding globulin (or transcortin) (Changes in binding proteins level can alter total cortisol concentration) • The binding affinity of synthetic steroid varies – Hydrocortisone ~95% – Prednisolone ~60% • Therefore, they are either bound weakly to albumin or as free steroid
Pharmacokinetics • Administration: – Oral/ IMI/ IV/ topical/ inhaled… • Half-life – Range from 1 hr for prednisolone to 4 hrs for dexamethasone • Clearance is slower in – Elderly – Renal and hepatic diseases
Measurement of cortisol level • Many tests available – Serum total cortisol – Free cortisol – Cosyntropin-stimulated serum total cortisol • Which one is recommended in critically ill patients?
• Free cortisol should be measured in critically ill patient – As most critically ill patients are hypoproteinemia – Binding proteins level is lower, which alter meaured serum total cortisol concentration
Mechanisms of action • Cortisol diffuse into target cells – Binds to a cytoplasmic glucocorticoid receptor – The activated receptor-drug complex enters the nucleus and binds to a specific glucocorticoid regulatory element on target DNA molecules, initiating or inhibiting gene transcription.
Effects of glucocorticoid • Metabolic effects – Facilitate conversion of protein to glycogen – Inhibit protein synthesis and stimulate protein catabolism to amino acid – Stimulate gluconeogenesis • It is vital to prevent hypoglycaemia during fasting
Effects of glucocorticoid • Anti-inflammatory – Reduce circulating immunocompetent cells and macrophages – Reduce formation of inflammatory mediators. • E. g. prostaglandins, leukotrienes
Effects of glucocorticoid • Immunosuppressive effects – Depress monocyte/ macrophage function – Decrease circulating thymus-derived lymphocytes (esp helper T 4 lymphocytes) – Inhibit the release of interleukins IL-1 and IL-2 – Inhibit the production of antibody
• Most synthetic glucocorticoids are: – Higher affinity for the receptor – Less rapidly inactivated – Have little or no salt-retaining properties
Common used glucocorticoids • Hydrocortisone – The pharmacologic form of cortisol • Prednisone/ dexamethasone/ methylprednisolne – Additional pharmacologic glucocorticoids • Compare to hydrocortisone – the other pharmacologic glucocorticoids bind cortisol binding globulin (CBG) poorly, resulting in more free, physiologically active glucocorticoid and greater potency at any given dose
Corticosteroid preparation Steroid Relative antiinflammatory potency Relative Naretaining potency Duration of action Hydrocortisone 1 1 S Prednisone 4 0. 8 I Dexamethasone 25 0 L Methylprednisolone 5 0 Fludrocortisone 10 125 S
Characteristics of common used steroids • Hydrocortisone – Oral: for replacement – IV: shock/ status asthmaticus – Topically: ointment for eczema • Prednisolone – Most widely used in inflammatory disease and allergic diseases
• Dexamethasone – Very potent (25 times of hydrocortisone) – No salt retaining actions – Especially useful for high-dose therapy in conditions e. g. cerebral edema (as water retention would be a disadvantage)
• Beclomethasone/ budesonide – Pass membranes poorly – More active topically than when given orally – Commonly used in asthma/ eczema
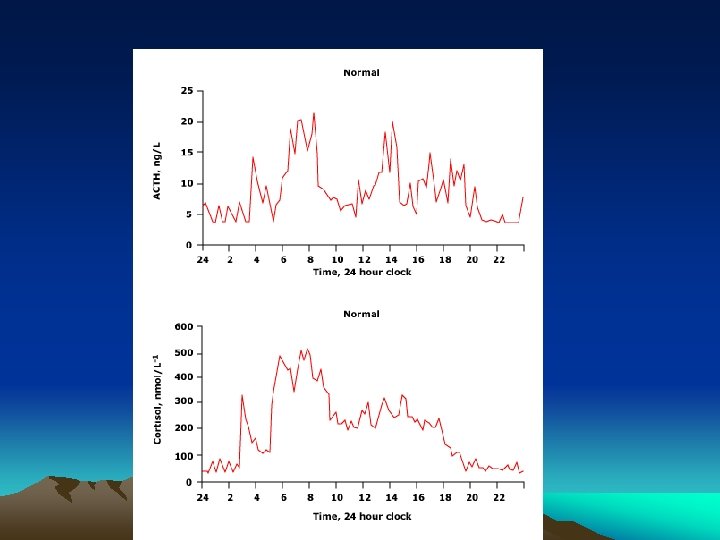
Normal serum cortisol production
In critically ill patients… • During physiological stress – E. g. major surgery, hypotension, severe infection • The HPA axis is activated – Diurnal variation is lost – Serum cortisol increase
In critically ill patients… However, there are circumstances in which cortisol availability can not be increased sufficiently to meet demand
Circumstances which may affect cortisol production • • Head injury Infections Malignancy Drugs – Etomidate – CNS depressants • Pituitary infarction • Adrenal haemorrhage • Previous glucocorticoid therapy
In critiically ill… • Absolute adrenal deficiency is rare • However suboptimal production is common Raise the interest in the possible therapeutic role of glucocorticoid in severe infection
Steroid in critical ill • The use of steroid in critical illness has existed since the early 20 th century. • 20 th century… – Adrenal glands are crucial to survival under conditions of physiologic stress • 80 th century… – The role of steroids in the treatment of septic shock has generated significant interest.
In the 1980 s • 3 prospective, randomized, double-blind, placebo-controlled studies • The effects of high-dose corticosteroids in patients with septic shock. A prospective, controlled study N Engl J Med 1984 Nov 1; 311(18): 1137 -43. • A controlled clinical trial of high-dose methylprednisolone in the treatment of severe sepsis and septic shock. N Engl J Med 1987 Sep 10; 317(11): 653 -8. • Effect of high-dose glucocorticoid therapy on mortality in patients with clinical signs of systemic sepsis. The Veterans Administration Systemic Sepsis Cooperative Study Group. N Engl J Med 1987 Sep 10; 317(11): 659 -65
In the 1980 s • 3 prospective, randomized, double-blind, placebo-controlled studies • The effects of high-dose corticosteroids in patients with septic shock. A prospective, controlled study N Engl J Med 1984 Nov 1; 311(18): 1137 -43. • A controlled clinical trial of high-dose methylprednisolone in the treatment of severe sepsis and septic shock. N Engl J Med 1987 Sep 10; 317(11): 653 -8. • Effect of high-dose glucocorticoid therapy on mortality in patients with clinical signs of systemic sepsis. The Veterans Administration Systemic Sepsis Cooperative Study Group. N Engl J Med 1987 Sep 10; 317(11): 659 -65
• None of the trials found a mortality benefit • Only 1 trial noted decreased duration to shock resolution associated with the administration of glucocorticoid • Remarks – All of the trials administrated high dose glucocorticoids (e. g. methylprednisolone 30 mg/kg ) – Used early endpoints (e. g. 14 days mortality)
In 1990’s • New interest about smaller, more physiological doses of steroid for longer duration
Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002 Aug 21; 288(7): 862 -71. • The largest double-blind, placebo-controlled trial • 300 patients were randomized within 8 hrs of the onset of septic shock – To receive placebo or – Hydrocortisone (50 mg Q 6 H) + fludrocortisone (50 mcg QD) • Classify the patients to have adequate adrenal reserve/ inadequate reserve by ACTH stimulation test
• Results – In the inadequate adrenal reserve group, hydrocortisone administration was associated with decreased • 28 days mortality • ICU mortality • Hospital mortality • More vasopressor withdrawal within 28 days – No difference in mortality in adequate adrenal reserve group
Corticosteroids for treating severe sepsis and septic shock. Cochrane Database Syst Rev 2004; (1): CD 002243. • A meta-analysis of 15 randomized, controlled trials (2023 patients) – Examine glucocorticoid administration in severe sepsis and septic shock – Use of glucocorticoid was associated with • Increased shock reversal by days 7 and 28 – Low dose glucocorticoid used > 4 days • Reduced 28 -day mortality • Reduced ICU mortality • Reduced hospital mortality
• Most studies investigating therapeutic role of glucocorticoid in critically ill patients with septic shock – Whether these findings can be applied to other critical illnesses is unknown
• A multicenter, randomized, double-blind, placebo-controlled trial
• Included total 499 patients – All with septic shock and remained hypotensive or required treatment with vasopressors for at least 1 hour after adequate fluid resuscitation • Study group – Hydrocortisone 50 mg Q 6 H for 5 days, then tapered during a 6 days period
• Primary end point – 28 days mortality in patients who did not response to corticotropin • Secondary end point – 28 days mortality in those response to corticotropin and in all patients – The rates of death in ICU and in the hospitals – The rate of death at 1 year – A reversal of organ system failure – Length of stay in ICU and hospital
Kaplan-Meier Curves for Survival at 28 Days
Kaplan-Meier Curves for the Time to Reversal of Shock
• Hydrocortisone did not improve survival in patients with septic shock, either overall or in patients who did not have a response to corticotropin • Use of hydrocortisone resulted in more rapidly reversal of shock (However, more rapid weaning from vasopressors does not improved survival!)
Other common indications of steroid in ICU • Chest – Asthma/ COPD – Other lung condition • Autoimmune diseases – Newly diagnosed or previously on steroid • Neurological condition – Brain mass – Meningitis
Conclusion • IVIG: – Although use of polyclonal IVIG is not recommended in current guidelines, recent studies found administration of it was associated with better outcomes. – Further investigation is required before introducing it into clinical practice.
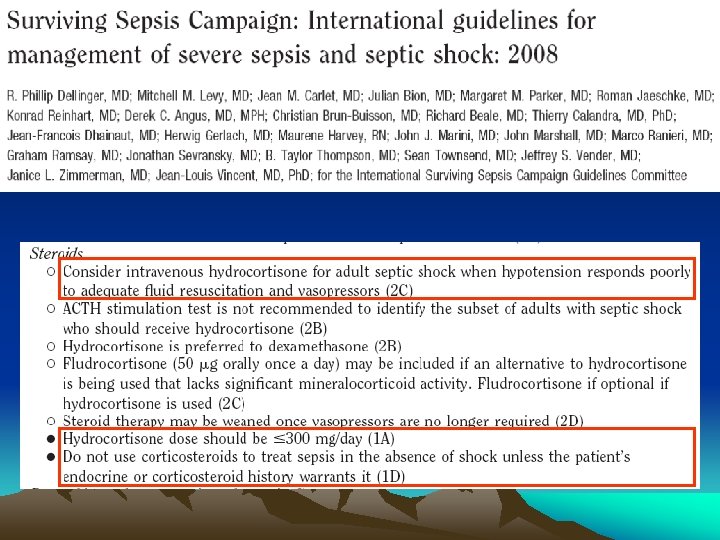
Conclusion • Steroid: – Steroid is a very common medication being used in ICU – Different preparations of steroid is recommended in different situations – Use of steroid is recommended in severe sepsis and septic shock according to Surviving Sepsis Campaign.
The End Thank you