Urogynecology Urinary incontinence Abdurrahman Sarisi Introduction Urinary incontinence

Urogynecology Urinary incontinence Abdurrahman Sarisi

Introduction �Urinary incontinence is the inability to hold urine, producing involuntary urinary leakage. �It is specially problematic because it is affects personal hygiene as well as social life. �It is increasingly prevalent as the ageing population expands.

The prevalence increases with age, with approximately 5 % of women between 15 and 44 years of age being affected, rising to 10 % of those aged between 45 and 64 years, and approximately 20 % of those older than 65 years.

Risk Factors

Physiology of continence � Continence and micturition involve a balance between urethral closure and detrusor muscle activity. � Normally urethral pressure > bladder pressure holding of urine. � The proximal urethra and bladder are normally both within the pelvis. � Intraabdominal pressure increases (from coughing and sneezing) are transmitted to both urethra and bladder equally, leaving the pressure differential unchanged, resulting in continence. � Normal voiding urethral pressure falls and bladder pressure rises. � Spontaneous bladder muscle (detrusor) contractions occur normally but they’re easily suppressed voluntarily.

Sensory signals Motor signals Detrusor muscle Sphincters

Physiology of Incontinence � a -adrenergic receptors. These are found primarily in the urethra and when stimulated cause contraction of urethral smooth muscle, preventing micturition. �b-adrenergic receptors. These are found primarily in the detrusor muscle and when stimulated cause relaxation of the bladder wall, preventing micturition. �Cholinergic receptors. These are found primarily in the detrusor muscle and when stimulated cause contraction of the bladder wall, enhancing micturition.

Cystometry - A flow pressure study - The patient is asked to empty the bladder as much as he can - A catheter is inserted to the bladder it measures whatever needed volume and pressure (bladder pressure) - A second catheter is inserted into the anus to measure the abdominal pressure - The bladder is filled with normal saline - When the patient feels a desire to urinate he will go and do so while the devices are in place

The following are parameters of normal bladder function: �Residual urine of <50 m. L. �First desire to void between 150 and 200 m. L. �Capacity between 400 and 600 m. L. �Detrusor pressure rise of <15 cm. H 2 O during filing and standing. �Absence of systolic detrusor contractions. �No leakage on coughing.

Classification of Incontinence � Urinary incontinence is classified according to pathophysiological concepts rather than symptomatology. � but the following definitions of symptoms are commonly used.
 pressure Detrusor over")
Cause of incontinence Change in pressure Rise in the internal (bladder) pressure Detrusor over activity incontinence Rise in the external (abdominal) Stress incontinence Change in volume Overflow incontinence
, previously called genuine stress incontinence. �is defied")
Urodynamic stress incontinence �Urodynamic stress incontinence (USI), previously called genuine stress incontinence. �is defied as the involuntary leakage of urine during increased abdominal pressure in the absence of a detrusor contraction (the pressure rise forms outside the bladder) �This is the most common incontinence in young women.

- With normal pelvic support any rise in the pressure* will be transmitted equally between the bladder and the proximal urethra which will prevent leakage of urine. - But, when pelvic support is lost for any reason the pressure will be only in the bladder exceeding that in the proximal urethra resulting eventually in incontinence. *This rise is not from detrusor over activity. Rather, it results from an increase in the abdominal pressure like sneezing or coughing.

The etiology of USI is thought to be related to a number of factors: � Damage to the nerve supply of the pelvic floor and urethral sphincter (loss of pelvic support). � Menopause and associated tissue atrophy may also cause damage to the pelvic floor (loss of pelvic support). � A congenital cause may be inferred, This may be due to altered connective tissue, particularly collagen (loss of pelvic support). � Chronic causes, such as obesity and chronic obstructive pulmonary disease, raise intra-abdominal pressure, and constipation and associated straining may also result in problems (increasing intraabdominal pressure).

History � Loss of urine occurs in small spurts simultaneously with coughing or sneezing. It does not take place when the patient is sleeping. Examination � Pelvic examination may reveal a cystocele. Neurologic examination is normal. � Investigative studies. Urinalysis and culture are normal. � Cystometric studies are normal with no involuntary detrusor contractions seen.

Cystocele

With cough or sneezing

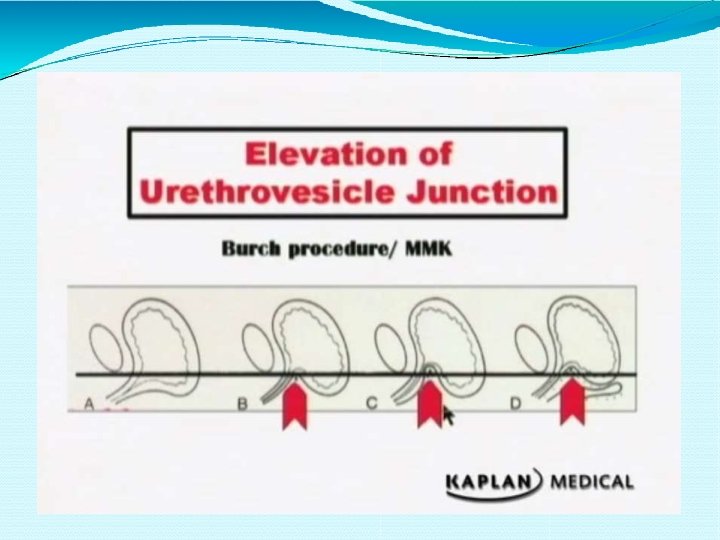
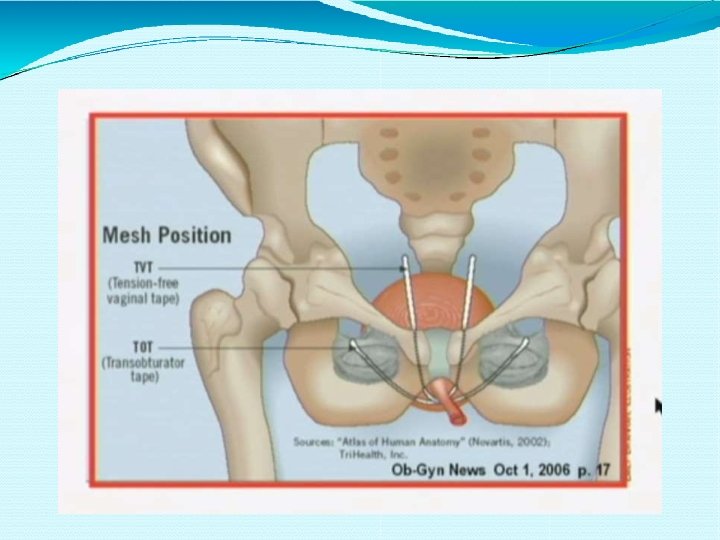
Management � Medical therapy includes Kegel exercises and estrogen replacement in postmenopausal women. � Surgical therapy aims to elevate the urethral sphincter so that it is again an intra-abdominal location (urethropexy). � This is done by attachment of the sphincter to the symphysis pubis, using the Burch procedure as well as the Marshall Marchetti-Kranz (MMK) procedure. � The success rate of both of these procedures is 85– 90%. � A minimally invasive surgical procedure is the tension-free vaginal tape procedure in which a mesh tape is placed transcutaneously around and under the mid urethra. It does not elevate the urethra but forms a resistant platform against intra-abdominal pressure.
. So,")
Bladder over-activity �It’s a bladder contraction during filling phase (< 400 ml volume). So, it’s characterized by �Urgency �Frequency �Nocturia
 Incontinence. This is the most common incontinence in older women. �It")
�Motor Urge (Hypertonic) Incontinence. This is the most common incontinence in older women. �It can be wet (there is urinary incontinence) or dry (no urinary incontinence). Etiology �Involuntary rises in bladder pressure occur from idiopathic detrusor contractions that cannot be voluntarily suppressed.

History � Loss of urine occurs in large amounts often without warning. This can take place both day and night. The most common symptom is urgency. Examination � Pelvic examination shows normal anatomy. Neurologic examination is normal. Investigative studies � Urinalysis and culture are normal. � Cystometric studies show normal residual volume, but involuntary detrusor contractions are present even with small volumes of urine in the bladder.

Without coughing Or sneezing
![Management Anticholinergic medications (e. g. , oxybutynin [Ditropan]); nonsteroidal anti-inflammatory drugs (NSAIDs) to inhibit](http://slidetodoc.com/presentation_image_h2/699bdca12a678a75f34f8a2a97d72a5d/image-26.jpg "Management Anticholinergic medications (e. g. , oxybutynin [Ditropan]); nonsteroidal anti-inflammatory drugs (NSAIDs) to inhibit")
Management Anticholinergic medications (e. g. , oxybutynin [Ditropan]); nonsteroidal anti-inflammatory drugs (NSAIDs) to inhibit detrusor contractions; tricyclic antidepressants; calcium-channel blockers.

Retention with over-flow �It’s leakage secondary to over-distended bladder, which becomes higher than urethral pressure. There is no or poor bladder contraction �Pathophysiology �Detrusor muscle hypotonia Denervated bladder � Medication like anti-cholinergic or alpha agonist � �Urethral obstruction
 Incontinence Etiology �Rises in bladder pressure occur gradually from an overdistended, hypotonic")
Overflow (Hypotonic) Incontinence Etiology �Rises in bladder pressure occur gradually from an overdistended, hypotonic bladder. When the bladder pressure exceeds the urethral pressure, involuntary urine loss occurs but only until the bladder pressure equals urethral pressure. (the pressure rises due to the effect of volume not contractions) �The bladder never empties. �Then the process begins all over. This may be caused by denervated bladder (e. g. , diabetic neuropathy, multiple sclerosis) or systemic medications (e. g. , anticholinergics).

History � Loss of urine occurs intermittently in small amounts. This can take place both day and night. The patient may complain of pelvic fullness. Examination � Pelvic examination may show normal anatomy; however, the neurologic examination will show decreased pudendal nerve sensation. Investigative studies � Urinalysis and culture are usually normal, but may show an infection. � Cystometric studies show markedly increased residual volume, but involuntary detrusor contractions do not occur.

There is no contractions in the bladder, but the residual volume is markedly increased.

Management �Intermittent self-catheterization may be necessary. �Discontinue the offending systemic medications. �Cholinergic medications to stimulate bladder contractions and a-adrenergic blocker to relax the bladder neck.

Sensory Irritative Incontinence Etiology � Involuntary rises in bladder pressure occur owing to detrusor contractions stimulated by irritation from any of the following bladder conditions: infection, stone, tumor, or a foreign body. History � Loss of urine occurs with urgency, frequency, and dysuria. This can take place day or night.

Examination � Suprapubic tenderness may be elicited, but otherwise the pelvic examination is unremarkable. Investigative studies A urinalysis will show the following abnormalities: � bacteria and white blood cells (suggest an infection) or red blood cells (suggest a stone, foreign body, or tumor). � A urine culture is positive if an infection is present. � Cystometric studies (which are usually unnecessary) would reveal normal residual volume with involuntary detrusor contractions present. Management � Infections are treated with antibiotics. � Cytoscopy is used to diagnose and remove stones, foreign bodies, and tumors.

Congenital causes Intra-urethral Epispidias, it’s due to failure of midline fusion of mesoderm. It’s associated with widening of bladder neck and short urethra.

Congenital causes �Extra-urethral cause �Bladder exstrophy is failure of mesoderm migration with absence of anterior bladder wall, anterior bladder wall �Ectopic ureter

Fistula �Can be �Gynecological cause like 95% due to pelvic surgery and radiation. Pelvic tumor can cause fistula �Obstetric cause like childbirth, in which bladder is compressed between head of fetus and bony pelvis �Can be uretrovaginal, vesicovaginal and urethrovaginal

History � The patient usually has a history of radical pelvic surgery or pelvic radiation therapy. � Loss of urine occurs continually in small amounts. This can take place both day and night. Examination � Pelvic examination may show normal anatomy and normal neurologic findings. Investigative studies � Urinalysis and culture are normal. � An intravenous pyelogram (IVP) will demonstrate dye leakage from a urinary tract fistula. With a urinary tractvaginal fistula, intravenous indigo carmine dye will leak onto a vaginal tampon. Management � can be treated by primary closure or by surgery and can be delayed until tissue inflammation and edema have resolved at about 4 weeks.


- Slides: 39