URINARY SYSTEM PHYSIOLOGY BIO 139 ANATOMY PHYSIOLOGY II

URINARY SYSTEM PHYSIOLOGY BIO 139 ANATOMY & PHYSIOLOGY II

Urinary System Functions • Maintain stability of the extracellular fluid volume by maintaining electrolyte composition • Helps maintain blood pressure and blood p. H • Maintains correct plasma volume through salt and water balance • Filters blood for removal of wastes during urine formation • Erythropoietin and renin release (endocrine function) • The kidneys always make urine even in the absence of fluid intake!
 FORM URINE. The tubular organs carry urine to outside the body.")
THE KIDNEYS (NEPHRONS) FORM URINE. The tubular organs carry urine to outside the body. The amount and content of urine made depends on conditions of the internal environment of the body.

Urine Formation: 3 Steps • Glomerular Filtration • Filtration of blood plasma • Tubular Reabsorption • From tubules to peritubular capillaries • Tubular Secretion • From peritubular capillaries back to tubules • Urine formation is a result of ALL of these processes!

Glomerular Filtration • 1 st step in urine formation • Non-selective, 20% of plasma that enters glomerulus is filtered • Remaining 80% of plasma sent to efferent arteriole • 180 L of glomerular filtrate formed a day • Entire plasma volume filtered 65 X a day

Tubular Reabsorption • Valuable substances returned to peritubular capillaries from filtrate in tubules = Selective • Substances eventually return to venous system • 180 L of filtrate formed a day, 178. 5 L reabsorbed • 1. 5 L eventually sent to renal pelvis

Tubular Secretion • Selective movement of non-filtered substances from peritubular capillaries to tubular system • Second way for substances to exit the blood • Secrete excess ions or substances the body does not need

Diagram the three processes!

Urine contains substances that were filtered and substances that were secreted, but not filtered.

Blood Supply to a Nephron • Renal artery branches into afferent arterioles • Each nephron receives blood from an afferent arteriole • Blood is filtered in glomerulus • Unfiltered blood exits through an efferent arteriole • This is still arterial blood • There is no gas exchange in the glomerulus!

Blood Supply to a Nephron • Efferent arteriole subdivides into peritubular capillaries • These supply renal tissue with blood • Are important in exchanges between the tubular and vascular components of a nephron • Tubular Reabsorption and Secretion

Glomerular Filtration • 20% of blood that enters glomerulus is filtered • Cells and proteins are not filtered • Glomerular filtrate exits through fenestrated pores in capillary walls and enters Bowman’s capsule
 • Recall the")
Glomerular Filtration • Filtration due to glomerular blood pressure (hydrostatic pressure) • Recall the processes discussed in Chapter 15 • GBP does not decrease through the length of the glomerulus (as it does in systemic capillaries) • Filtration occurs throughout ENTIRE length of capillary • 180 L of filtrate formed a day • Glomerular filtration rate (GFR) = 125 ml/min • 124 ml/min is reabsorbed later

Factors affecting GFR • Plasma Colloid Osmotic Pressure • Due to presence of plasma proteins • Is usually less than GBP so blood is filtered • Bowman’s Capsule Hydrostatic Pressure • Due to fluid in bowman’s capsule • As long as GBP is greater than the sum of COP and Bowman’s HP, blood is filtered

Glomerular Filtration

Factors Affecting Glomerular Filtration Rate • Changes in plasma colloid osmotic pressure • Loss of protein rich plasma (burn patient) • _ COP = GFR • Dehydrating diarrhea • _ COP = GFR • Obstruction (kidney stone) • Increases Bowman’s HP, which will decrease GFR

Relationship of Systemic BP to GBP • Normally you would expect: • ↑ Systemic BP to ↑ GBP (which would ↑ GFR) and • ↓ Systemic BP to ↓ GBP(which would ↓ GFR) • Autoregulation prevents this!

Autoregulation • In order to compensate for changes that would occur in GFR, resistance of afferent arteriole is adjusted • This works to maintain normal GFR in a wide range of systemic blood pressures

Renal Autoregulation of GFR • BP constrict afferent arteriole • BP dilate afferent arteriole • Stable for BP range of 80 to 170 mm. Hg (systolic) • Cannot compensate for extreme BP
 • Vasoconstriction of afferent arteriole = less blood flow")
Autoregulation of GFR (through GBP) • Vasoconstriction of afferent arteriole = less blood flow to glomerulus • Vasodilation of afferent arteriole = increase blood flow to glomerulus

Autoregulation: Tubuloglomerular Feedback Mechanism • Juxtaglomerular apparatus detects changes in GFR in DCT • In response, releases vasoactive chemicals that act on afferent arteriole • Vasoconstrictors • Vasodilators

AUTOREGULATION WORKS TO MAINTAIN GFR WITHIN THE NORMAL RANGE OF BP FLUCTUATIONS. However, GFR can be changed ON PURPOSE by extrinsic control mechanisms that override Autoregulation. This is used to control Blood Pressure.

Sympathetic Control of GFR • More long term, in response to changes in blood volume • If blood volume decreases, will produce less urine to conserve more plasma • Vasomotor center in medulla detects changes in blood pressure • Sympathetic innervation of smooth muscle of arterioles • Vasoconstriction of afferent arteriole = less blood flow to glomerulus = ↓GBP = ↓GFR = less urine output = salt & water conserved = ↑MAP • Would also have increases in tubular reabsorption of water and salt and increased thirst

THE KIDNEYS RECEIVE 2025% OF THE TOTAL CARDIAC OUTPUT. They compose less than 1% of total body weight.

Tubular Reabsorption • Tubules → Peritubular capillaries • Selective process, only reabsorb what the body needs • Electrolytes, glucose, amino acids, organic nutrients, water • 180 L filtrate formed, 178. 5 L reabsorbed • Goal is to maintain proper ECF volume and composition • Tubules have higher capacity to reabsorb substances needed by the body than for substances of no value!

Tubular Reabsorption • Absorptive capacity depends on the body’s needs • ***As water is reabsorbed, concentration of wastes and ions in urine increases in the tubules • Both active and passive processes are involved • Active – Na+, glucose, amino acids, organic nutrients, PO 43 -, K+, Ca++, SO 42 • Passive – Cl-, H 20, urea
 • Reabsorbs 65% of GF to peritubular capillaries • Great")
Proximal Convoluted Tubules (PCT) • Reabsorbs 65% of GF to peritubular capillaries • Great length, prominent microvilli and abundant mitochondria for active transport • Reabsorbs greater variety of chemicals than other parts of nephron • transcellular route - through epithelial cells of PCT • paracellular route - between epithelial cells of PCT • Transport maximum: when transport proteins of plasma membrane are saturated; glucose > 220 mg/d. L remains in urine (glucosuria)

Sodium Reabsorption • 80% of total energy requirement of kidneys used for Na+ transport • Na+ reabsorbed through entire length of tubules (involves Na+/K+ ATPase pump) • 99. 5% of filtered Na+ is reabsorbed • 67% in PCT • 25% in ascending loop of Henle • 8% in DCT & collecting duct (hormonal control)

Renin-Angiotensin-Aldosterone System • Controls Na+ reabsorption in the DCT and collecting duct • Responds to decrease in Na. Cl/ECF volume/arterial blood pressure • Why are all three of these related?

Salt and Water Relationship • Na+ and Cl- responsible for 90% of ECF osmotic activity • ↑Na+ = ___ H 20 due to osmosis = ___ ECF volume = ___ BP; OR • ↓Na+ = ___ H 20 due to osmosis = ___ ECF volume = ___ BP

Cells Of Juxtaglomerular Apparatus Release Renin In Response To Low Na. Cl/Ecf Volume /Arterial Blood Pressure

Renin-Angiotensin-Aldosterone System -efferent arterioles
")
Effects of Angiotensin II • Stimulates aldosterone release from adrenal cortex • Na+ (Cl-) reabsorption in DCT & CD • H 20 retention (under control of vasopressin) • Induces arteriolar vasoconstriction • Increases thirst • Stimulates vasopressin release from posterior pituitary • H 20 reabsorption in DCT & CD • *DCT & CD impermeable to water unless vasopressin is present
 • BP stimulates")
Inhibitors of Renin Pathway • Effect of atrial natriuretic factor (ANF) • BP stimulates right atrium • atrium secretes ANF • ANF promotes Na+ and water excretion by inhibiting renin and aldosterone release • BP drops

Congestive Heart Failure • Failing heart muscle causes decreased arterial blood pressure • Stimulates renin system • Causes H 20 retention, making condition worse • Accompanied by fluid retention and edema, which the activation of renin exacerbates • Treatment: • Low salt diet, diuretics, ACE inhibitors

Tubular Secretion: Selective • Peritubular capillaries to tubules • Mostly for K+ and H+ and organic ions • Urine composed of substances from glomerular filtration and tubular secretion

Tubular Secretion • H+ secretion • Important in acid-base balance • PCT, DCT, CD • ↓ p. H = ↑ H+ secretion • K+ secretion • Important in maintaining normal membrane potential in muscles and nerves • Reabsorbed in PCT • Secreted in DCT & CD in response to aldosterone • Both processes coupled to Na+ reabsorption!!

K+ and H+ Secretion from DCT & CD o. Both processes coupled to Na+ reabsorption!!

Aldosterone Release • Aldosterone is released in response to 2 different stimuli • Decreased Na+ levels • Increased K+ levels

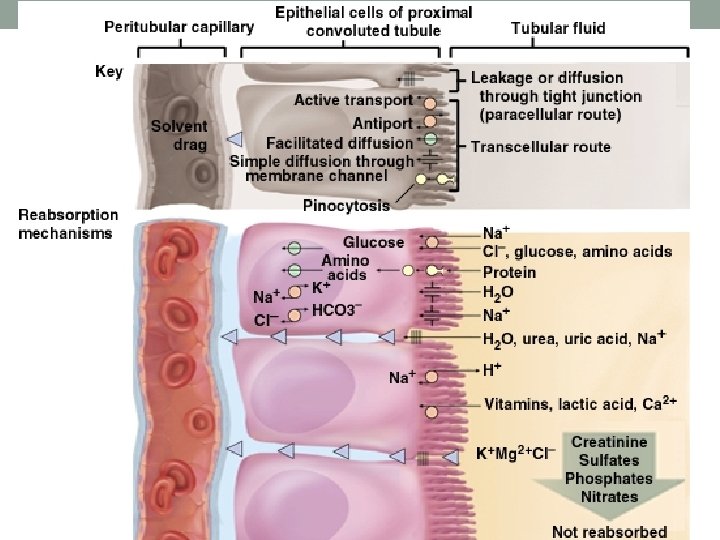
Let’s summarize what occurs in the tubular system for reabsorption and secretion.

Summary of Tubular Reabsorption and Secretio

Urine Formation • Glomerular Filtration • Tubular Reabsorption • Tubular Secretion • Substances found in urine come from filtration and secretion • 1. 5 L produced a day

Urine Formation • Body can produce urine of varying concentrations • Involves juxtamedullary nephrons and corresponding vasa recta

Osmotic Gradient of Kidneys • Concentration of medullary interstitial fluid increases towards renal pelvis • 300 mosm/L-1200 mosm/L from cortex to medulla • Gradient allows kidney to produce urine ranging in concentration from 1001200 mosm/L • Interstitial fluid around LOH not isotonic to other body fluids • Maintained by countercurrent mechanism of Vasa recta & limbs of Loop of Henle

Osmotic Gradient of Kidneys • Fluid from PCT that is entering descending loop of Henle is isotonic to body fluids • Descending loop of Henle • highly permeable to H 20 • Slightly permeable to Na. Cl • *H 20 is reabsorbed, following Na in ascending loop • *Fluid becomes HYPERTONIC by tip of loop • Ascending loop of Henle • impermeable to H 20 • Permeable to Na. Cl • *Na+ is reabsorbed, H 20 remains in tubule • *Fluid becomes HYPOTONIC as it reaches DCT

Countercurrent Mechanism of Vasa Recta • Flow in long loops of Henle and vasa recta is countercurrent • Flow in the 2 adjacent limbs of the loop is in opposite directions • Na+ reabsorption in ascending loop results in H 20 reabsorption from descending loop • Vertical osmotic gradient exists in renal medulla here • PCT fluid is isotonic to body fluids • DCT fluid is hypotonic to body fluids

Countercurrent Multiplier of Nephron Loop Diagram

Maintenance of Osmolarity in Renal Medulla
")
Vasa recta Loop of Henle Juxtamedullary nephron and its blood supply together Glomerular (Bowman’s) capsule H 2 O Glomerulus Afferent arteriole Na+CI– Blood flow Distal convoluted tubule Presense of Na +-K+-2 CI– symporters Interstitial fluid in renal cortex 200 H 2 O Efferent arteriole 300 Collecting duct 300 100 H 2 O 320 Na+CI– 400 Interstitial fluid in renal medulla 380 200 H 2 O 400 800 600 Na+CI– 700 780 600 H 2 O Urea H 2 O 980 1000 Na+CI– 400 500 600 ascending limb cause buildup of Na+ and Cl– H 2 O collecting duct reabsorb more water when ADH is present H 2 O 1 Symporters in thick Osmotic gradient 3 Principal cells in H 2 O 580 600 320 300 H 2 O Proximal convoluted tubule Flow of tubular fluid 800 H 2 O 800 900 4 Urea recycling 1000 Na+CI– H 2 O causes buildup of urea in the renal medulla 1000 1100 H 2 O 1200 2 Countercurrent flow through loop of Henle establishes an osmotic gradient 1200 Loop of Henle 1200 Papillary duct 1200 Concentrated urine (a) Reabsorption of Na+CI– and water in a long-loop juxtamedullary nephron 1200 (b) Recycling of salts and urea in the vasa recta

Concentrating Urine • Urine is concentrated due to the effect of the hormone vasopressin • Causes H 20 reabsorption in the DCT and CD as needed by the body fluids • What stimulates vasopressin release? • Where is it released from?

Collecting Duct Concentrates Urine • Osmolarity 4 x as high deep in medulla • Medullary portion of CD is permeable to water but not to Na. Cl

Effect of ADH on Renal Tubules • without ADH, DCT and collecting duct are impermeable to water • with ADH, DCT and collecting duct become permeable to water • with ADH, water is reabsorbed in DCT and CD by osmosis 20 -27

Urea and Uric Acid Excretion Urea • product of protein catabolism • plasma concentration reflects the amount or protein in diet • enters renal tubules through glomerular filtration • 50% reabsorbed • the rest is excreted Uric Acid • product of nucleic acid metabolism • enters renal tubules through glomerular filtration • 100% reabsorbed • 10% secreted and excreted 20 -28
 Amount returned to blood/d (Reabsorbed)")
Tubular Reabsorption Amount in 180 L of filtrate (/day) Amount returned to blood/d (Reabsorbed) Amount in Urine (/day) 3 L 180 L 178 -179 L 1 -2 L Protein (active) 200 g 2 g 1. 9 g 0. 1 g Glucose (active) 3 g 162 g 0 g Urea (passive) 1 g 54 g 24 g 30 g 0. 03 g 1. 6 g Total Amount in Plasma Water (passive) Creatinine (about 1/2) 0 g 1. 6 g (all filtered) (none reabsorbed)
 • UREA • URIC ACID • TRACE AMINO ACIDS")
Urine Composition • WATER (95%) • UREA • URIC ACID • TRACE AMINO ACIDS • IONS

Elimination of Urine • • • Glomerulus Bowman’s Capsule Pct Loop Of Henle Dct Collecting Duct Minor Calyx Major Calyx Renal Pelvis Ureters Urinary Bladder Urethra
- Slides: 57