URINARY OBSTRUCTION By d hana omer Incidence Frequency

URINARY OBSTRUCTION By: d. hana omer.

• Incidence Frequency – – – • No data available in unselected populations 20 -35% prevalence in large survey among elderly men 3. 8% (adults); 2. 0% (children) postmortem examinations Sex – – No gender difference until 20 years Women 20 -60; Men > 60

ETIOLOGY Ø A urinary obstruction means the normal flow of urine is blocked. As the urine backs up, it can cause infections in the urinary system, damage the bladder and affect the kidneys. If the kidneys are injured (a condition called hydronephrosis) it can be life threatening.

CLINICAL MANIFESTATIONS Ø The cause in children may be a birth defect. In children or adults, the urine may be blocked due to scarring along the urinary tract due to injury or infection. In adults, the most common cause is a kidney stone (renal lithiasis). With men, as they age, the most common cause is an enlarged prostate gland. Other causes include tumors, cancers and pregnancy.

n Etiology Types of obstruction n Mechanical blockade ¡ ¡ n n Intrinsic extrinsic Functional defects Congenital

Ø The obstruction can involve one or both kidneys, called unilateral or bilateral obstruction. The blockage may be complete or partial. It can occur suddenly (acute) or develop over time (chronic). It varies by location.

UNILATERAL OBSTRUCTION
 weak stream")
Signs and symptoms Ø Ø Ø inability to pass urine (urinary retention) weak stream of urine interrupted stream blood in the urine pain in either flank (side) or in the back abdominal pain and/or swelling

LABS AND DIAGNOSTICS Ø Ø The physician may order a kidney, ureter, and bladder (KUB) radiograph. Renal ultrasonography or IVP will provide definitive information about structural changes. Other diagnostic tests may include visual examinations with the aid of endoscopy blood chemistry profile

l An X ray of a blocked ureter. The ureters are muscular tubes that carry urine from the renal pelvis in each kidney to the urinary bladder.

MEDICAL MANAGEMENT Ø Ø Ø To establish urine drainage and relieve discomfort Conservative measures include insertion of an indwelling catheter, analgesic (usually opioid), and an anticholinergic agent (Atropine) to decrease smooth muscle motility To establish urine drainage, inserting a catheter directly into the bladder through the abdominal wall (suprapubic cystostomy)
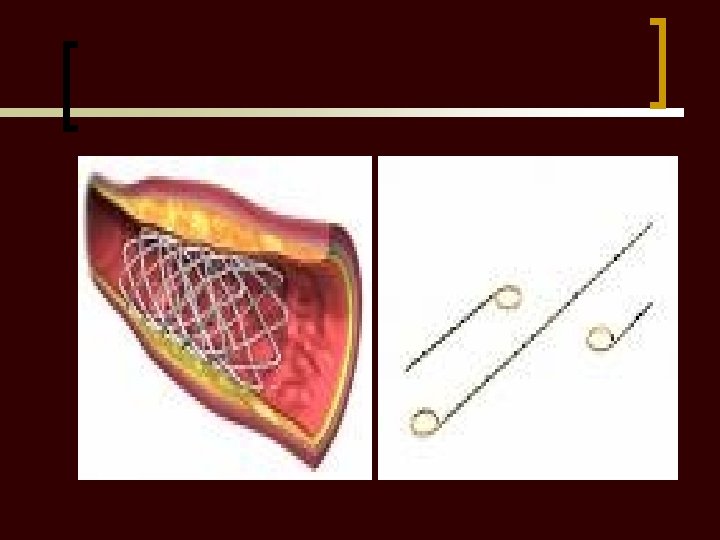
, or into the kidney (nephrostomy). A stent")
CONT… Ø Ø Into a ureter (ureterostomy), or into the kidney (nephrostomy). A stent is a tube, use for surgical correction of an obstruction in the urinary system A mesh-like tube or coil-shaped device is inserted through an endoscope into the ureter Stent holds the tubular structure open to facilitate drainage.

Nx INTERVENTIONS Ø Ø Observation for hemorrhage Maintaining aseptic care of surgical site Restoring optimal urinary function Providing a safe environment to prevent injury and infection

PATIENT TEACHING Ø Ø Liberal fluids to produce two litres of urine per day A diet without excessive sodium (salty food), calcium (dairy products), oxalate (nuts) and urates (for example, red meat). Avoid excessive intake at dinner (overeating) and extend interval from dinner until retiring for the night. Urinary alkalinisation with addition of citrate (a stone inhibitor) is helpful in recurrent uric acid or calcium stone-formers

PROGNOSIS Ø Ø Is variable, depending on the cause of the obstruction. If surgical correction is successful, the prognosis is excellent.
- Slides: 17