UpperAirway Stimulation for Obstructive Sleep Apnea 31914 Satomi

Upper-Airway Stimulation for Obstructive Sleep Apnea 3/19/14 Satomi Fujii

Case � 59 yo. M w/ PMH of HTN, obesity, DMII, HLD and moderate OSA non-compliant with CPAP �CPAP is “too uncomfortable” �Trial of several different masks failed �c/o Daytime sleepiness �BP 140’s/80’s on 3 anti-hypertensives �BMI 31 �Mallampati score 4 �Neck circumference 18 in �Any alternative therapy for OSA?

Obstructive Sleep Apnea �Affects 13% Men & 6% women in N. America � 26% adults at risk �Age increases from 18 -45 yo, plateau 55 -65 yo �More prevalent in AA <35 yo

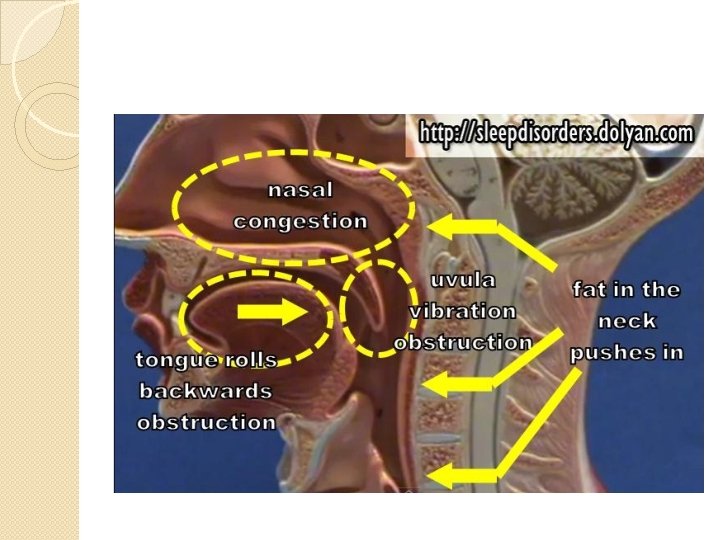
Definition �Anatomical compromise in which soft tissues and craniofacial structures around the pharyngeal airway lead to increased airway collapsibility �Intermittent oxyhemoglobin desaturation & sympathetic activation

OSA Definitions �Apnea ◦ Cessation of airflow for >10 s �Hypopnea ◦ Reduction in airflow (≥ 30%) for ≥ 10 s with EEG arousal or oxyghemoglobin desaturation (≥ 4%) � AHI � Number �Oxygen of apnea & hypopneas per hour of sleep time desaturation index ◦ the number of times per hour of sleep that the blood oxygen level drops by ≥ 4% from baseline

Disease Spectrum AHI Daytime Sleepiness HTN Cor pulmonale Cardiopulmonar y failure Nocturnal angina Mild 5 -15 -/+ Moderate 15 -30 + Severe >30 ++ - ++ +/+/- - - +/-

Pathophysiology �Anatomic narrowing ◦ Requires increased inspiratory pressures �Abnormal neuromuscular control ◦ Pharyngeal airway maintains patency due to protective reflexes while awake ◦ Loss of the reflexes during sleep ◦ Reduces the activity of the pharyngeal dilator muscle ◦ Collapse of the susceptible airway

Impoten ce Sex Drive MVA Nighttime Cardiac Death Peri/Po st-op Complic a-tions Memory Problem OSA DM or Insulin Resista nce Stroke Heart Failure All. Cause Mortalit y Medical Disabilit y

Treatment �Nonsurgical modalities �Surgical modalities

Nonsurgical Treatment � Weight loss ◦ Diet, exercise, bariatric surgery, medications � Sleep hygiene ◦ Avoidance of sedatives, alcohol ◦ Positional changes- lateral recumbent � Pharmacotherapy ◦ ◦ ◦ (none proven to be effective) Protriptyline- decreases REM sleep Xanthine based drugs Steroids Antibiotics Nasal medications � Nasal continuous positive airway pressure (CPAP) � Oral appliances

Upper Airway Bypass Procedure Tracheostomy Nasal Procedures Septoplasty Functional rhinoplasty Nasal Valve Surgery Turbinate reduction Nasal polypectomy Endoscopic procedures Oral, Oropharyngeal & Nasopharyngeal Procedures Uvulopalatopharyngoplasty Palatal advancement pharyngoplasty Tonsillectomy and/or adenoidectomy Excision of tori mandibularis Palatal implants Hypopharyngeal Procedures Tongue Reduction (partial glossectomy, tongue ablation, lingual tonsillectomy) Tongue Advancement Stabilization (Genioglossus advancement, Hyoid suspension, mandibular advancement, tongue suspension) Laryngeal Procedures Epiglottoplasty Hyoid suspension Global Airway Procedures Maxillomandibular advancement
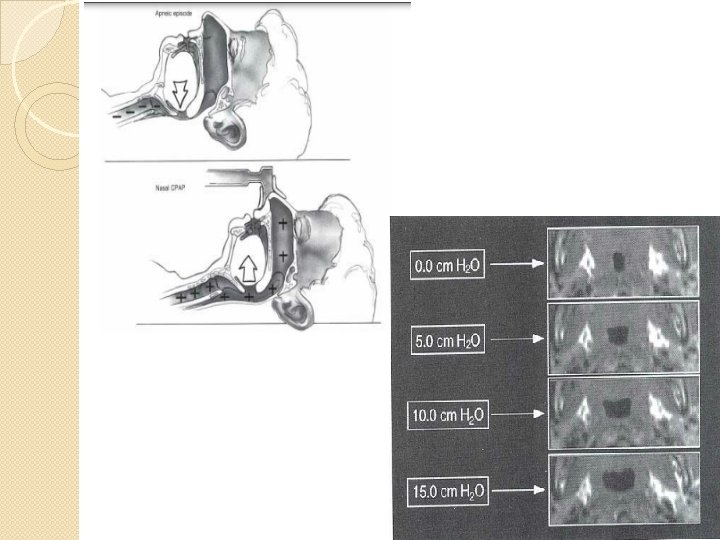
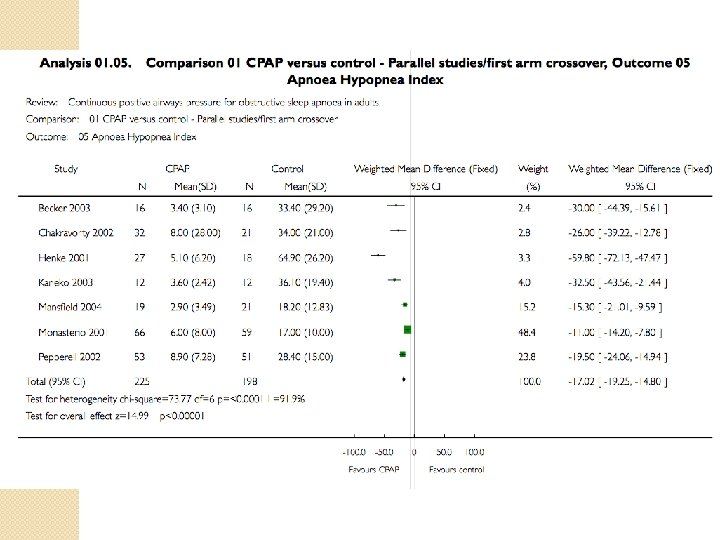
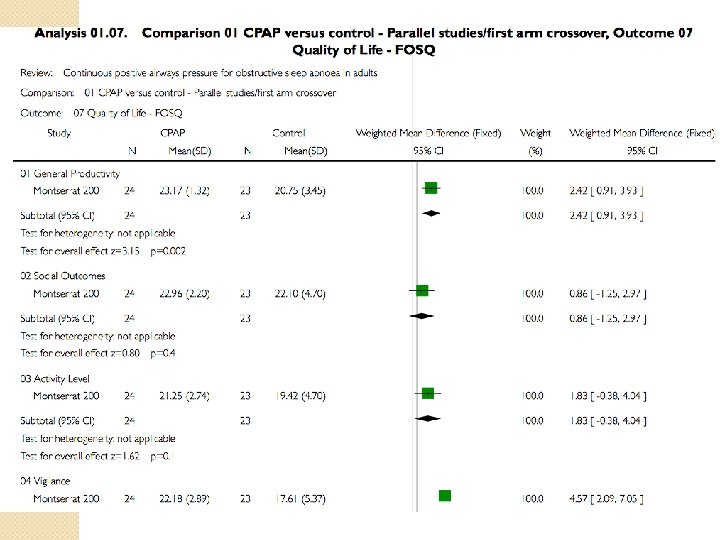

CPAP �Reduced the frequency of respiratory events during sleep �Decreases daytime sleepiness �Improves quality of life across a range of disease severities �Improves cognitive function �Improves Depression �More effective than oral appliances �? Mortality benefit
 uses ≤ 4 hrs/night �Mean duration of use 3")
CPAP Adherence �Non-adherence (29 -83%) uses ≤ 4 hrs/night �Mean duration of use 3 hrs among pts w/ non-adherence �Mean use of 5 hours per night �Objective improvement seen w/ ≥ 6 hours/night use

Risks for Non-Adherence

Risks for Non-Adherence

Other Reasons for Unsuccessful Treatment of OSA �Weight gain �Inappropriate level of prescribed positive pressure �Additional disorder (i. e. narcolepsy) �Drugs

�Alternative to CPAP for OSA Treatment?

Hypothesis �Strategies that increase activity in the pharyngeal dilator muscles should be effective for patients who have dysfunction in these muscles �Stimulation of the hypoglossal nerve may present the reduction in drive to the upper-airway muscles

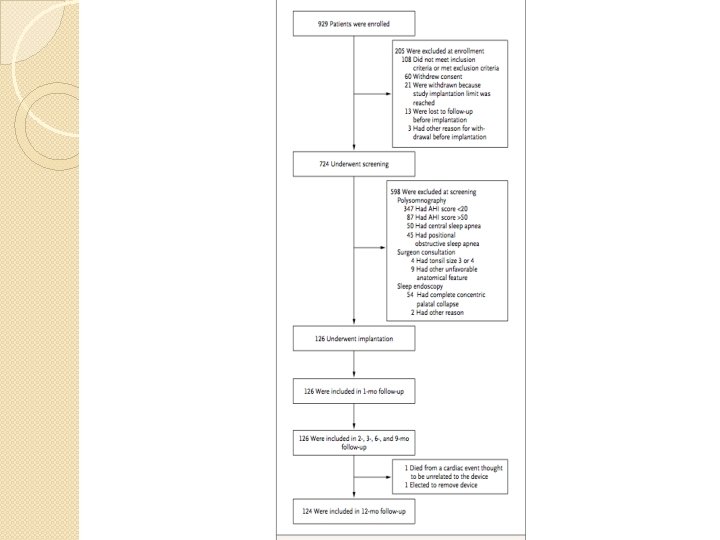
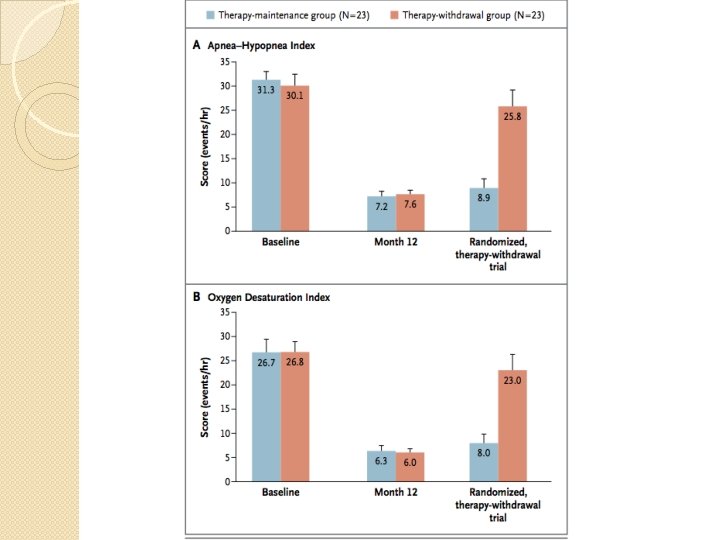
Method �Multicenter, uncontrolled, prospective, single-group, cohort design �Nov 2010 -March 2013 �N=126 �Participants serving as their own controls �Primary outcome eval RCT tx �Responders( N= 46)were randomly assigned to therapy-maintenance gp (N=23) or therapy-withdrawal gp (N=23) (device turned off x 7 days)

Inclusion Criteria �Moderate-to-severe OSA pts w/ difficulty accepting or adhering to CPAP �Dx confirmed w/ polysomnography �Medical & surgical consultation �Endoscopy during drug-induced sleep to assess anatomy

Exclusion Criteria ◦ ◦ ◦ ◦ BMI >32 Neuromuscular disease Hypoglossal-nerve palsy Severe restrictive or obstructive pulmonary disease Moderate-to-severe pulmonary arterial hypertension Severe valvular heart disease NYHA class III/IV HF Recent MI or severe cardiac arrhythmias (w/in 6 months) ◦ Persistent uncontrolled HTN despite meds ◦ Active psychiatric disease ◦ Coexisting nonrespiratory sleep disorders ◦ AHI<20 or >50 ◦ AHI <10 while not in supine ◦ >25% of apnea & hypopnea d/t central or mixed sleep disorder ◦ Anatomical abnormalities(tonsil visible beyond the pillars or extending to midline) ◦ Complete concentric collapse at the retropalatal airway

Intervention
 in the R")
Intervention �Surgical implantation of the upperairway stimulation system (Inspire Medical Systems) in the R ipsilateral mid-infraclavicular region �The stimulation electrode placed on the hypoglossal nerve to recruit tongue-protrusion function �The sensing lead was placed btw the internal & external intercostal muscles to direct ventilatory effort

Use of Therapy

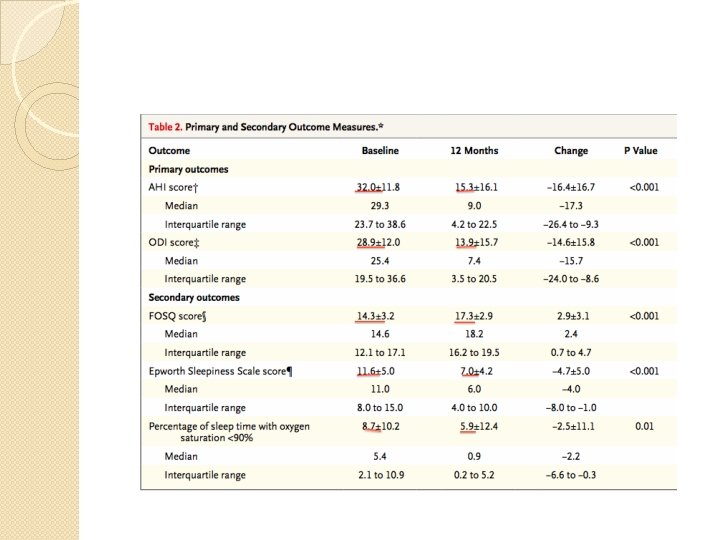
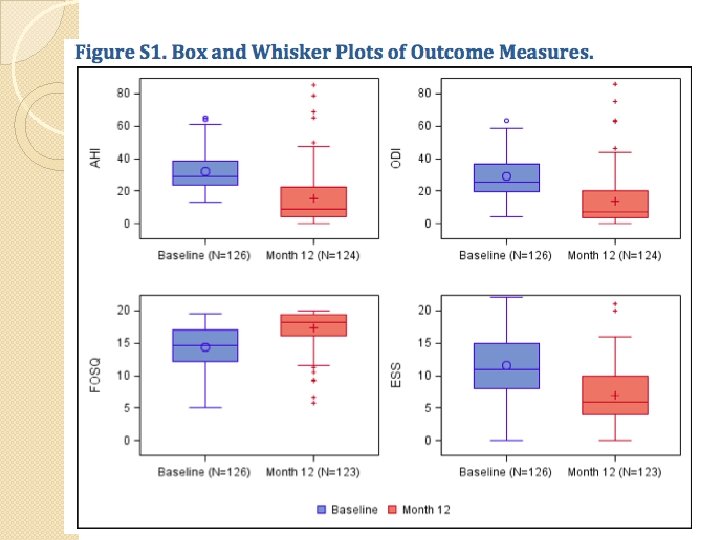
Method �Primary outcome ◦ Change in the severity of OSA by AHI & Oxygen Desaturation Index (ODI) at 12 month ◦ Proportion of pts w/ AHI score reduction of at least 50% ◦ AHI score <20 at 12 months ◦ ODI reduction at least 25% �Secondary outcome ◦ Self-reported sleepiness ◦ Disease-specific quality of life (Epworth Sleepiness Scale & Functional Outcomes of Sleep Questionnaire or FOSQ) ◦ % of sleep time w/ O 2 sat <90%

Follow ups �Polysomnographic study, Epworth Sleepiness Scale & FOSQ at 2, 6 & 12 months �Device adjustment at 2 & 6 months

Characteristics

Results �Primary outcome ◦ Median AHI 29. 3 9. 0 at 12 months ( 68%)p<0. 001 ◦ Median ODI 25. 4 7. 4 ( 70%) p<0. 001 ◦ At least 50% in AHI & AHI <20: 66% (97. 5% CI, 57) ◦ At least 25% ODI: 75% (97. 5% CI, 66) �Secondary outcome ◦ FOSQ mean change 2. 9 pts; 95% CI, 2. 4 -3. 5 (p<0. 001) ◦ Epworth Sleepiness Scale score: 11 6 (p<0. 001) ◦ Median % of sleep time w/ O 2 sat <90%: 5. 4% 0. 9% (p=0. 01)
")
Therapy-Withdrawal Study �AHI score: 25. 8 vs 7. 6 at 1 -week (p<0. 001) �Average increase in AHI in therapywithdrawal gp: 18. 2 events/hr �Average increase in therapymaintenance gp: 1. 7 events/hr (difference in changes in mean scores, 16. 4+/-12. 0 events/hr; p<0. 001)

Adverse Event
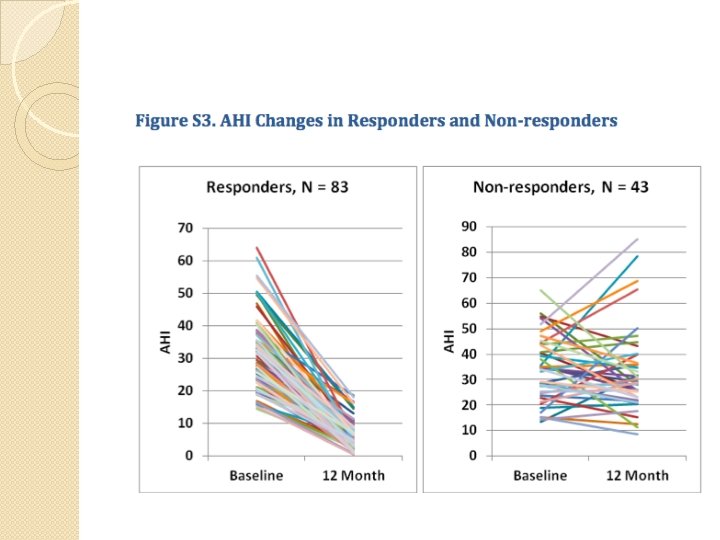

Non-Responders �Total 19 w/ increase in AHI ◦ 7: AHI>15/hr ◦ 12: increase in AHI of <15/hr ◦ 4: increase in AHI >60/hr � 3: Retropalatal airway remained closed despite elimination of tongue-base collapse w/ stimulation � 2: significant central & mixed apnea >25% of total apneas/hypopneas � 1: marked maxillomandibular deficiency & low anterior hyoid bone long narrow upper airway

Clinical Appraisal �Endoscopic study carefully selected patients who may benefit from the implantation of the stimulation device �Eliminate adherence issues �RCT of therapy-withdrawal study suggests AHI decrease was d/t the stimulation device rather than AHI variability �Surgical procedures without major benefits may be replaced by hypoglossal-nerve stimulation over

Limitations � Only a minority of screened pts underwent implantation � Small study � Unblinded, prospective, open-label design No control group although control of CPAP users would be impractical � No control � Unmeasured factors (diet, exercise) may have changed during the study & may have contributed to the reduction OSA � OSA reduced but not eliminated � May not be appropriate for people w/ excessive airway collapsibility

Limitations �Unable to objectively assess adherence of the stimulation device (86% w/ daily use by self-report) �Some w/ significant increase in AHI at 12 months �Non-responders were not included in RCT �? Population �Need to refine patient selection (sophisticated analysis of airflow signals & focused biomarkers) �? CV risk and mortality effects �? Cost effectiveness

Can this be applied to my patient? �Yes �Meets inclusion criteria �May increase his quality of life and improve daytime sleepiness �Rare side effects �? Long term effect

Conclusion �In selected moderate-to-severe OSA patients who are non-adherent to CPAP therapy, hypoglossal-nerve stimulation resulted in a reduction in the severity of OSA with acceptable adverse-event profile.

Thank you
- Slides: 49