UPPER RESPIRATORY TRACT INFECTIONS ALOK SINHA Department of


 Chronic")





















 and/or surrounding tissue n Caused by: •")

 shows a ‘Cherry red' epiglottis")
 for HIB • result takes long")


 • Others - Ampicillin and")




 Group A beta-haemolytic streptococcus (20 -30%)")






 flu pandemic data Area Confirmed deaths Worldwide (total) 14,")
 Influenza)")














 and zanamivir • used to prevent or reduce influenza")



- Slides: 63
UPPER RESPIRATORY TRACT INFECTIONS ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal
• The upper respiratory tract includes • nose • paranasal sinuses • pharynx • upper part of the larynx above the level of the true vocal cords
Infections of the Upper Respiratory Tract Site Nasal cavity Disease Coryza (common cold) Chronic atrophic rhinitis Rhinoscleroma Invasive fungal infections Nasal diphtheria Mucocutaneous leishmaniasis Syphilis (tertiary) Lepromatous leprosy Rhinosporidiosis Agents Many different viruses Bacteria (Klebsiella ozaenae) Klebsiella rhinoscleromatis Mucor, Aspergillus Corynebacterium diphtheriae Leishmania braziliensis Treponema pallidum Mycobacterium leprae Rhinosporidium seeberi Paranasal sinuses Acute sinusitis Chronic sinusitis Aspergilloma ("fungus ball") Pyogenic bacteria Aspergillus species Pharynx, tonsil Acute pharyngitis Many different viruses Streptococcus pyogenes Diphtheria Corynebacterium diphtheriae Pharyngeal gonorrhea Neisseria gonorrhoeae Peritonsillar abscess (quinsy) Pyogenic bacteria Infectious mononucleosis Epstein–Barr virus Retropharyngeal space Abscess Tuberculosis Larynx Acute laryngitis Acute epiglottitis and laryngitis Pyogenic bacteria Mycobacterium tuberculosis Many different viruses Haemophilus influenzae
Which specialty should treat & there for teach these diseases ?
The Common Cold. .
CORYZA n n An estimated 2 of every 5 persons are affected each year (40%) World population: 6, 775, 235, 741 40% of this = 2, 710, 094, 296 Some experience multiple episodes in 1 year
n Rhinoviruses: most common agents n n Over 100 serotypes have been implicated Other viruses implicated included n n n coronaviruses influenza C parainfluenza virus adenoviruses respiratory syncytial virus
• Highly contagious: 75% of patients infected with Rhinovirus will have symptoms • Respiratory droplets spread by sneezing, coughing v hand contact with nose, eyes, or face v Fomite - Skin cells, hair, clothing (hanky) bedding v
n Contributing factors: Change in weather n Loss of sleep n Going outside with wet hair n Fatigue n
Signs and symptoms n Incubation period: 2 – 4 days n May last from 6 – 10 days or possibly up to 3 weeks after incubation period
• Initial complaints • sneezing • clear, watery rhinorrhea @ nasal obstruction • general malaise but no fever • Subsequently • Headache • nasal congestion • scratchy throat
After 2 – 3 days • nasal discharge becomes thicker, cloudy, and yellowish in color • systemic symptoms improve • Hoarseness, cough, and sore throat may last up to 7 – 10 days
Diagnosis: n n n Made on clinical grounds • Pt’s symptoms • nasal exam showing n reddened, edematous mucosa n narrowed nasal passages n watery discharge Laboratory and/or imaging only indicated if other conditions are strongly suspected Viral isolation/culture is not practical
Treatment
n n No curative treatment Supportive therapy – 10 treatment • Rest • Fluids & humidification • Decongestants (Phenylephrine - α 1 -adrenergic receptor agonist) • Analgesics • Cough suppressants • Mucolytics • Antihistamines
Zinc Gluconate n Short term use of zinc lozenges (zinc gluconate 10 -15 mg q 2 hrs) shown to reduce duration of subjective symptoms if begun early in course of disease
n n n ? Role of antibiotics Antibiotics should be considered if symptoms last longer than 10 -14 days (secondary bacterial infection) Inappropriate prescribing of antibiotics is common • Due to patient beliefs/misinformation of cold being bacterial in origin
Pharyngitis
n n May be of bacterial or viral origin Most common cause Rhinovirus • Self-limiting; usually lasts 3 -4 days n Group A, beta-hemolytic strep is the primary bacterial pathogen q in 1/3 cases - early detection reduces incidence of
Signs and symptoms: n Inflammation of pharynx & lymphoid tissue results in • Fever & malaise • sore throat • rhinorrhea • Tonsillar exudates n • Anterior cervical adenopathy There is usually a lack of cough
Diagnosis n On PE: observe throat for tonsillar exudates; obtain throat swab n Rapid streptococcal identification tests are most commonly used • Sensitivity – 80% • Specificity – 95% n Throat cultures may be collected if rapid strep screen is negative
Management/Treatment: n Symptomatic treatment • salt-water gargles • throat lozenges • Acetaminophen • cool-mist humidification
n Antibiotics treatment necessary to treat proven strep infections • Benzathine penicillin G 1. 2 million units as a single dose, is optimal therapy • For pen – allergic pts, n erythromycin 500 mg po QID x 10 days n Azithromycin 500 mg once daily x 3 days
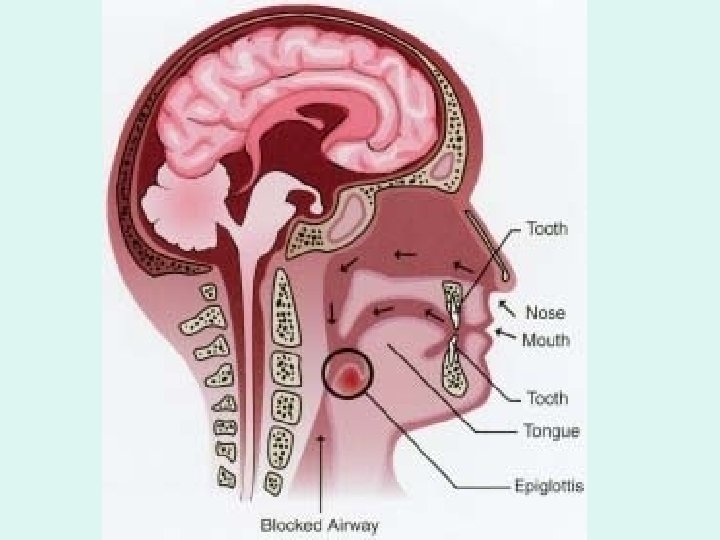
Acute epiglottitis
n Bacterial cellulitis of the epiglottis (supraglottis) and/or surrounding tissue n Caused by: • Haemophilus influenzae type b (Hi. B)- most likely • H. parainfluenzae and streptococci some times n Average of onset: 1– 5 years old • In most adults the disease is less severe and of slower onset
Clinical Features n Sudden onset of • Sore throat • Fever • Head forwardly extended, usually with drooling n Stridor - present
Pharyngeal visualization (w/ EXTREME caution) shows a ‘Cherry red' epiglottis
n n Neutrophil leucocytosis Epiglottis culture usually (+) for HIB • result takes long time n Blood cultures frequently (+) for HIB in children • organisms fewer than in meningitis n Lateral X-Ray neck • • • enlarged hypopharynx forward neck extension with “thumbprinting” of epiglottitis
Epiglottitis- Differential diagnosis n n n n Angioneuropathic edema of supraglottic structures Anaphylaxis Caustic ingestion Thermal burns of epiglottis Infectious mononucleosis Laryngotracheitis Blunt Trauma
Treatment • Intubation is often required, but usually discontinued in less than 24 h • Early antibiotic treatment and intubation may prevent the need for tracheostomy • Steroids to reduce inflammation and avert tracheostomy- unproven but used • Tracheostomy: may be required in life threatening conditions
n Drug treatment • #1 Ceftriaxone (or cefotaxime, cefuroxime) • Others - Ampicillin and Sulbactam • Ticarcillin disodium and clavulanate potassium • piperacillin/tazobactam • levaquin • Gatifloxacin • Amoxicillin should not be used due to noted resistance
Prevention n Hi. B vaccination early!!! • Prior to Hi. B, there were roughly 20 K cases of Hi. B disease each year (U S data) • Post-vaccine era = incidence has decreased by 95%. n Prophylaxix: Family Members, day-care workers, health-care workers • Rifampin 300 mg q 12 h x 2 d
Acute laryngitis
Healthy Vocal Cords n Healthy vocal cords have smooth straight edges
Normal healthy vocal cords • pearly-white color • in contrast to the pinkish surrounding tissue
Causes n n Viral (70 -80%) Group A beta-haemolytic streptococcus (20 -30%)
n Often a complication of acute coryza • Dry sore throat • Hoarse voice or loss of voice • Attempts to speak cause pain • Initially painful and unproductive cough • Stridor in children (croup) because of inflammatory oedema leading to partial obstruction of a small larynx Croup (Laryngotracheobronchitis) is a group of respiratory diseases that often affects infants and children[
Complications rare § Chronic laryngitis • Downward spread of infection may cause • Tracheitis • Bronchitis • Pneumonia
Treatment n n Rest voice Paracetamol 0. 5 -1 g 4 -6 -hourly for relief of discomfort and pyrexia Steam inhalations may be of value Antibiotics not necessary in simple acute laryngitis
Influenza
l. Possible accounts in 412 BC Flu First recorded pandemic in 1580 l. Destroyed Charlemagne's army in 876 A. D. l. Killed thousands in 1647
1918 -1919 Spanish Flu pandemic l 21 million people died worldwide out of a billion infected (total world population at that time 1. 8 billion) 8. 5 million people died in World War I l. Possible end to war
2009 (H 1 N 1) flu pandemic data Area Confirmed deaths Worldwide (total) 14, 286 European Union and EFTA 2, 290 Other European countries and Central Asia 457 Mediterranean and Middle East 1, 450 Africa 116 North America 3, 642 Central America and Caribbean 237 South America 3, 190 Northeast Asia and South Asia 2, 294 Southeast Asia 393 Australia and Pacific 217 Note: The proportion of confirmed deaths within total deaths due to
Swine Flue (H 1 N 1) Influenza)
Answer these two questions n Is the Influenza or Flu caused by “Influenza” virus ? n What H. Influenza is
Etiology • caused by a group of myxoviruses • common types • A Influenza A (H 1 N 1) virus is a subtype. causes • endemic in pigs – swine influenza • and birds – avian influenza new H 1 N 1 strain of swine-origin caused pandemic • B • C
• New influenza viruses are constantly being produced by mutation • antigenic drift: – small changes in surface antigen • antigenic shift: – acquire new antigens by reassortment between avian/swine & human strains
Transmission n n Swine influenza virus common throughout pig populations worldwide Transmission from pigs to humans is not common and does not always lead to human influenza
• People with regular exposure to pigs are at increased risk of swine flu infection – Meat of an infected animal poses no risk of infection when properly cooked • Transmission from one person to another is by droplet or fomite
Mild symptoms : • Fever • sore throat & cough • headache, muscle or joint pains • nausea vomiting, or diarrhea n Those at risk of a more severe infection: • asthmatics • diabetics • obesity • heart disease • immunocompromised • pregnant women
Symptoms in severe cases : n n n Difficulty breathing or shortness of breath Pain or pressure in the chest or abdomen Sudden dizziness Confusion Severe or persistent vomiting Low temperature
Complications Abigail & Brittany Hensel March 7, 1990
n Some patients deteriorates around 3 to 5 days after onset • Respiratory failure n requiring immediate admission to an intensive care unit & mechanical ventilation • myocarditis & collapse - some times
Diagnosis n Should not wait for laboratory confirmation • Diagnosis based on clinical & epidemiological background & start treatment early n For Confirmation a nasopharyngeal or oropharyngeal tissue swab tested with • Real-time or RT-PCR n not required in most people with flu symptoms. test results do not affect recommended course of treatment
n n For diagnosis of influenza and not H 1 N 1/09 flu more widely available tests: Rapid influenza diagnostic tests (RIDT): results 30 minutes • high rate of false negative n n patients should be treated empirically based on the level of clinical suspicion Direct & indirect immunofluorescence assays (DFA & IFA): take 2– 4 hours
Role of immunization l. The l. Natural l. Humans flu virus is constantly mutating immunity is not very strong will probably never be immune from the flu
Influenza immunization l. Not 100% effective l. Scientists l. Chosen choose the predominant strains the year before
Swine flu vaccines 1. Nasal spray vaccine released in early October 2009 • live attenuated H 1 N 1 virus approved for use in healthy individuals age 2 - 49 n not be used in pregnancy or immunocompromised n 2. Injectable vaccine • Made from killed H 1 N 1 n used from 6 months to the elderly including
Antiviral agents n Oseltamivir (Tamiflu) and zanamivir • used to prevent or reduce influenza A and B symptoms • Efficacy reduces if the flu symptoms already have been present for 48 hours or more n Supportive measures in severe infection • ventilation support • treatment of other infections like pneumonia
Prophylaxis n n Avoid crowded places Well ventilated houses Covering mouth & nose while coughing / sneezing Avoid touching nose & eyes
Frequent hand washing
That’s all in this session !