UPPER LIMB FRACTURES FRACTURES CLINICAL PICTURE INVESTIGATIONS TREATMENT

UPPER LIMB FRACTURES

FRACTURES CLINICAL PICTURE INVESTIGATIONS TREATMENT COMPLICATIONS

: E E R U R T U C T A C R I F P Y L N A A C I N I L C LOCAL: SYMPTOMS: History of trauma, Pain, Swelling, Limited movements. SIGNS Swelling, Ecchymosis, Tenderness, Limited movements Deformity, Length discrepancy, Abnormal movements, Crepitus SYSTEMIC: SHOCK HYPOVOLAEMIC NEUROGENIC SPINAL DISTAL: NEURO-VASCULAR

UMA : Direct l l l Indirect Vehicular accedents Fall from height Crushing accidents Avulsion fractures Special types n Fall on out-stretched arm Minor trauma…Path. Fr n Frequent trauma … Stress fr n FRACTURE DISLOCATION FRACTURE-DISLOCATION
 SIGNS OF FRACTURE Swelling Local pain Tenderness Ecchymosis, abrasions Limited joint movement")
PROBABLE(SUSPICIOUS) SIGNS OF FRACTURE Swelling Local pain Tenderness Ecchymosis, abrasions Limited joint movement

Sure Signs: Deformity, Length discrepancy, Abnormal movements, Crepitus DINNER FORK Crepitus VARUS S-SHAPE
 PLAIN X-RAY CT MRI ISOTOPE SCAN SONOGRAPHY LAB OTHERS: TYPES")
INVESTIGATIONS RADIOGRAPHY( IMAGING ) PLAIN X-RAY CT MRI ISOTOPE SCAN SONOGRAPHY LAB OTHERS: TYPES SPECIAL FINDINGS D. D SPECIAL TECHNIQUES Angio-, sino-, EMG, DEXA, ….
")
TREATMENT FRACTURE: REDUCTION FIXATION FOLLOW-UP OPEN FRACTURES ASSOCIATED INJURY l CONSERVATIVE Traction CAST (POP) Others (sling, bandage, …) l OPERATIVE

COMPLICATIONS l. EARLY l. LATE - BONY - SOFT TISSUES MANAGEMENT

UP PE R LI M B IN JU RI ES

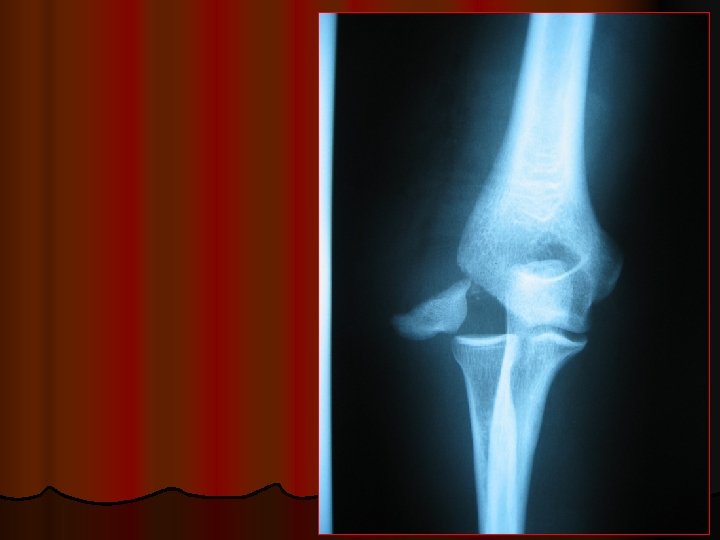
INJURIES AROUND THE ELBOW <<7 4 l l l l 1 - SUPRACONDYLAR FRACTURE 2 - DISLOCATION ELBOW 3 - FRACTURE OLECRANON 4 - FRACTURE HEAD RADIUS 5 - FRACTURES OF HUMERAL CONDYLES 6 - EPICONDYLE FRACTURE 7 - PULLED ELBOW 3 >>2 5 6 1 5

SUPRACONDYLAR FRACTURE l Two types: Flexion typeₒExtension type l Caused by fall on caused by fall on tip of elbow(15%)outstretched hand(85%) FLEX EXT

Cubitus varus “ Carrying angle”


TREATMENT A- REDUCTION: Undisplaced or minimally displaced fractures: No need for reduction Displaced fractures : Must be reduced as soon as possible Closed Reduction is done under general anaesthesia (G. A) by traction and manipulation to correct sideways and front to back displacement, tilt, and rotation. Reduction is performed under xray control. Radial pulse must be palpated after reduction; if absent the elbow is gradually extended till the pulse returns l l X-Rays are taken to confirm reduction B- FIXATION : Above E. Slab
 IN Unstable types WITH Vascular injuries FOLLOW- UP")
PINNING (Percutaneous…Open ) IN Unstable types WITH Vascular injuries FOLLOW- UP
: - gangrene")
COMPLICATIONS A- Early complications: 1. Vascular injury (injury of the brachial artery): - gangrene of the digits - Compartment syndrome - Volkmann’s ischaemic contracture - ischaemic neurologic damage 2. Nerve injury: - The median nerve - The radial and ulnar

B. Late complications: 1. 2. Deformity from malunion cubitus varus Volkmann’s ischaemic contracture 3. Myositis ossificans (Post-traumatic ossification) 4. Elbow stiffness 5. Nonunion: is very rare to occur in S. C. Fr CUBITUS VARUS

VOLKMANN, s ISCHAEMIC CONTRACTURE

Cubitus varus “ Carrying angle”

Cubitus valgum “ Carrying angle”

MYOSITIS OSSIFICANS

DISLOCATION ELBOW POSTERIOR

PO ST ER IO R rior Ante POSTERIOR DISLOCATION
")
PULLED ELBOW (SUBLUXATION OF THE HEAD OF THE RADIUS )

DISLOCATION SHOULDER ANTERIOR RECURRENCE
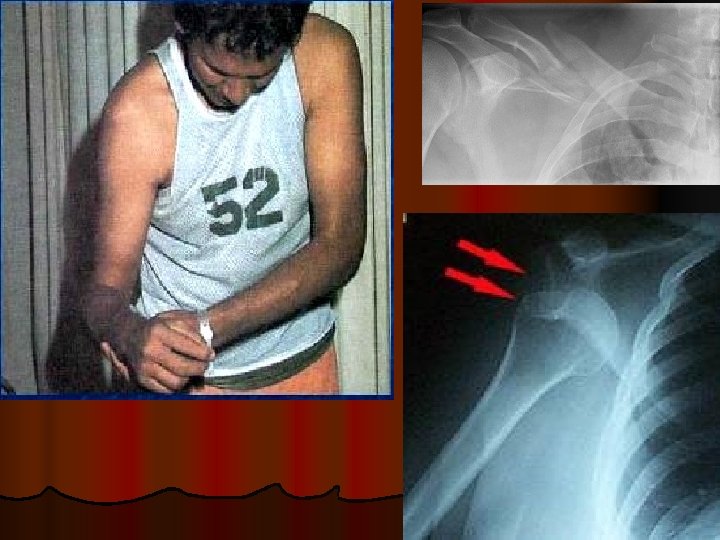

l Axillary nerve injury Deltoid wasting

FRACTURE CLAVICLE

l Figure of 8 bandage l Simple arm sling

INJURIES OF THE WRIST Colles’ fracture: - It is the most common of all fractures in older people. - The patient is usually a post menopausal woman. Mechanism of injury: Fall on the out stretched hand. It occurs within 2 cm of the articular surface and may extend into the distal radio-carpal joint or the distal radio-ulnar joint. The distal fragment shows: Dorsal angulation (Dinner fork deformity), dorsal displacement, radial angulation, radial displacement, impaction (shortening) and There is often an accompanying fracture of the ulnar styloid

Clinical features: There is a dinner fork deformity, with prominence on the back of the wrist and a depression in front with local tenderness and pain on wrist movements. X-ray: There is a transverse fracture of the radius at the corticocancellous junction, and often the ulnar styloid process is broken off. The distal fragment is impacted into radial and backwards tilt. Sometimes it is comminuted or severely crushed. .

Special Types COLLES FR. SMITH FR

BARTON FRACTURE This is an intra-articular fracture. A fracture in which the dorsal or volar rim of the distal radius is displaced with the hand.
, cast is applied below elbow (if")
Treatment: Undisplaced fractures (or only very slightly displaced), cast is applied below elbow (if ulnar styloid is intact) or above elbow if there is fracture ulnar styloid. If the patient’s wrist is markedly swollen a splint is first applied till the sweling has resolved, then cast is applied. Displaced fractures must be reduced under anaesthesia then cast is applied either below or above elbow according to the presence of ulnar styloid fracture. X-rays are taken after one week, redisplacement is not uncommon to which re-reduction is done. The fracture usually unites in about 6 weeks.
 FOR SIMPLE NONDISPLACED FRACTURES WITH NO SKIN NOR NEUROVASCULAR COMPROMISE")
CAST (POP) FOR SIMPLE NONDISPLACED FRACTURES WITH NO SKIN NOR NEUROVASCULAR COMPROMISE

Comminuted Or unstable types of Colles’ fr. - can not be treated sufficiently with cast - immobilization, this is supplemented by Kwire fixation OR Plate and screws. - Cast and wires are removed after 6 weeks. Severely comminuted fractures external fixator is needed.

Complications: Early Circulation in the fingers should be checked; cast may need to be split. Nerve injury is rare, but compression of the median nerve in the carpal tunnel is fairly common. Mild symptoms may resolve by elevation and release of cast. Persistent and severe symptoms require carpal tunnel release. Reflex sympathetic dystrophy is common but usually it does not progress to full picture of Sudek’s atrophy. This is avoided by finger exercises. Triangular fibrocartilage complex (TFCC) injury: As the distal radius displaces dorsally, the TFCC is damaged.

Late Malunion is common either because reduction was not complete or because displacement within the plaster was overlooked. Osteotomy to correct the deformity is needed if there is painful movement. Delayed union and non union of the distal radius are rare, but the ulnar styloid process often joins by fibrous tissue only and remains painful for several months. Stiffness of the shoulder, elbow and fingers from patient neglect is a common complication that can be avoided by exercises. Tendon rupture of extensor pollicis longus occasionally occurs a few weeks after an apparently trivial undisplaced fracture of the lower radius.

GOOD LUCK
- Slides: 41