Upper Cervical Spine Fractures Dr Hani Alsulaimany Upper



















 Basion to Tip of Dens <12 mm")






 may be treated nonoperatively")






")

 Type II 50 -75")

 • Airway compromise – 0/8 nondisplaced")













 Second most common fracture of axis 25% of C")
 Usually due to hyperextension-axial compression forces")






- Slides: 61
Upper Cervical Spine Fractures Dr Hani Alsulaimany
Upper Cervical Spine Fractures • • • Epidemiology Anatomy Imaging Characteristics Common Injuries Management Issues
Epidemiology • 717 cervical spine fractures in 657 patients over 13 years • C 1 and Hangman fractures found more in the young – Odontoid fractures evenly distributed • Younger patients have higher energy injuries • C 2 fractures most common The epidemiology of fractures and fracture-dislocations of the cervical spine Ryan, M. D. ; Henderson, J. J. Injury, 1992, 23, 1, 38 -40
Upper Cervical Anatomy
Upper Cervical Anatomy • Biomechanically Specialized – Support of “large” Cranial mass – Large range of motion • Flexion/extension • Axial rotation • Unique osteological characteristics
Large Cranial Mass Keel below the SNL is thick bone Roberts, DA; Doherty, BJ; Heggeness MH. Quantitative Anatomy of the Occiput and the Biomechanics of Occipital Screw Fixation Spine 23(10), 15 May 1998, pp 1100 -1107
The course of the vertebral artery through C 1 and C 2 determines the possibility of placing screws for fixation of fractures and dislocations • C 1 lateral mass screws • C 1 -2 transarticular screws • C 2 pedicle/pars screws
Normal Vertebral Artery
Tortuous Vertebral Artery
C 1 - Atlas • No body • 2 articular pillars – Flat articular surface – Vertebral artery foramen • 2 arches – Anterior – Posterior • Vertebral artery groove
C 2 Anatomy • Dens – Embriological C 1 body – Base poorly vascularized – Osteoporotic • Flat C 1 -2 joints • Vertebral artery foramena – Inferomedial to superolateral
Anatomy – The Ligaments • Allow for the wide ROM of upper C-spine while maintaining stability • Classified according to location with respect to vertebral canal – Internal: • Tectorial membrane • Cruciate ligament – including transverse ligament • Alar and apical ligaments – External • Anterior and posterior atlanto-occipital membranes • Anterior and posterior atlanto-axial membranes • Articular capsules and ligamentum nuchae
Atlanto-Axial Anatomy Tectorial Membrane
Atlanto-Axial Anatomy Tranverse Ligament C 1 -C 2 joint Occiput C 1 C 2 Alar Ligament
Atlanto-Axial Anatomy Facet for Occipital Condyle Transverse Ligament
Vertebral Artery Atlanto-Axial Anatomy
Radiographic Evaluation
Plain Radiographic Evaluation Lateral View Prevertebral Swelling Soft Tissue Shadow <6 mm at C 2 Concave/Flat Pre-dental space < 3 mm Atlanto-Occipital Joint Congruence Radiographic Lines* Open Mouth AP Distraction C 1 -2 Symmetry
Radiographic Diagnosis – Screening Lines Harris’s lines Powers’s Ratio
Radiographic Lines Harris’ Lines Basion-Dental Interval (BDI) Basion to Tip of Dens <12 mm in 95% >12 mm ABNORMAL Basion-Axial Interval (BAI) Basion to Posterior Dens -4 -12 mm in 98% >12 mm Anterior Subluxation >4 mm Posterior Subluxation Harris et al, Am J Radiol, 1994
Radiographic Lines Powers’ Ratio • BC/OA – >1 considered abnormal • Limited Usefulness • Positive only in Anterior Translational injuries • False Negative with pure distraction Powers et al, Neurosurg, 1979
Radiographic Diagnosis CT Scan Same rules as with plain films Better visualization of cranio-cervical junction Subluxation Focal hematomas Occipital condyle fractures Dens fractures
Radiographic Diagnosis MRI Increased Signal Intensity in : C 0 -C 1 Joint C 1 -2 Joint Spinal Cord Cranio-cervical ligaments Pre-vertebral soft tissues Dickman et al, J Neurosurg, 1991 Warner et al, Emerg Radiol, 1996
Upper Cervical Spine Fractures • Common Injuries – Occipital Condyle Fracture – Craniocervical sprain? – C 1 ring injuries – Odontoid Fracture – Hangman’s Fracture • Uncommon Injuries – Craniocervical Dislocation – Rotatory subluxation
Occipital Condyle Fracture Type I Impaction Fracture Type II Extension of basilar skull fracture Type III ALAR ligament Avulsion Anderson , SPINE 1988 Tuli, NEUROSURGERY, 1997
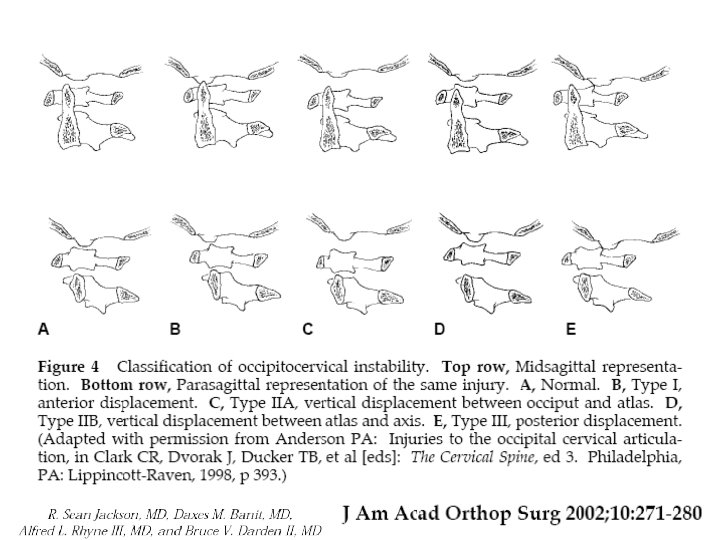
Cranio-cervical Dislocation • • Antlanto-Occipital Joint Occipito-Cervical Joint Cranio-cervical Joint Atlanto-Axial Joint
Cranio-cervical sprain (stage 1) may be treated nonoperatively
Cranio-cervical Dislocation Commonly Fatal Present 6 -20% of post mortem studies – Alker et al, 1978 – Bucholz & Burkhead, 1979 – Adams et al, 1992 50% missed injury rate 1/3 Neurological Worsening – Davis et al, 1993
Cranio-cervical Dislocation Treatment Emergency Room Collar/sandbag Halo vest Definitive Posterior occipital cervical fusion ALWAYS include C 1 and C 2
Atlas Fractures - Treatment Collar 1. Isolated anterior arch 2. Isolated posterior arch 3. Non-displaced Jefferson fracture
Atlas Fractures - Treatment Displaced <6. 9 mm Halo vest * 3 mos Displaced >6. 9 mm Halo traction (reduction) * several weeks followed by halo vest Immediate halo vest Posterior C 1 -2 fusion (unable to tolerate halo) After brace treatment complete confirm C 1 -2 stability Flexion/extension films C 1 -2 fusion for ADI > 5 mm
Transverse ligament avulsion Bony avulsions may heal with nonoperative management TAL rupture does not heal with nonoperative management and requires C 1 -C 2 arthrodesis
Atlas Fractures - Treatment Fusion options Gallie Post-op halo Brooks Jenkins Transarticular Screws C 1 lateral mass/C 2 pars-pedicle screws
Odontoid Fractures Most common fracture of Axis (nearly 2/3 of all C 2 Fxs) 10 – 20 % of all cervical fractures Etiology Bimodal distribution Young - high energy, multi-trauma Elderly - low energy, isolated injury (most common C-spine Fx elderly)
Elderly and the Odontoid • Platzer Studies – Elderly increased pseudarthrosis rate( 12% v. 8%) – Elderly tolerated pseudarthosis well(1/5) – Elderly tolerated halo well – 10% mortality (4/41) – 22% complication rate • Chapman studies – Elderly did not heal the odontoid fracture (4/17) – Elderly tolerated halo well (7/8) – 15% mortality (3/20) • Harrop and Vaccaro – 9/10 “union” – 5/10 postop halo – 1/10 perioperative death • Multiple series of high mortality rates Anterior screw fixation of odontoid fractures comparing younger and elderly patients. Authors: Platzer, P. ; Thalhammer, G. ; Ostermann, R. ; Wieland, T. ; Vecsei, V. ; Gaebler, C. Source: Spine, 2007, 32, 16, 1714 -1720, United States Nonoperative management of odontoid fractures using a halothoracic vest. Authors: Platzer, P. ; Thalhammer, G. ; Sarahrudi, K. ; Kovar, F. ; Vekszler, G. ; Vecsei, V. ; Gaebler, C. Source: Neurosurgery, 2007, 61, 3, 522 -9; discussion 529 -30, United States Posterior atlanto-axial arthrodesis for fixation of odontoid nonunions. Authors: Platzer, P. ; Vecsei, V. ; Thalhammer, G. ; Oberleitner, G. ; Schurz, M. ; Gaebler, C. Source: Spine, 2008, 33, 6, 624 -630, United States Type II odontoid fractures in the elderly: early failure of nonsurgical treatment. Authors: Kuntz, C. , 4 th; Mirza, S. K. ; Jarell, A. D. ; Chapman, J. R. ; Shaffrey, C. I. ; Newell, D. W. Source: Neurosurg. Focus. , 2000, 8, 6, e 7, United States Efficacy of anterior odontoid screw fixation in elderly patients with Type II odontoid fractures. Authors: Harrop, J. S. ; Przybylski, G. J. ; Vaccaro, A. R. ; Yalamanchili, K. Source: Neurosurg. Focus. , 2000, 8, 6, e 6, United States
Fracture Classification Anderson and D’Alonzo Type I 2 % (2/49) Type II 50 -75 % (32/49) Type III 15 -25 % (15/49) Fractures of the odontoid process of the axis. Authors: Anderson, L. D. ; D'Alonzo, R. T. Source: J. Bone Joint Surg. Am. , 1974, 56, 8, 1663 -1674, UNITED STATES
Subtypes of Type II Fractures • Type IIA and B are amenable to anterior fixation • Type IIC is not • Does not include part of facet, not a Type III Grauer, J. N et al Proposal of a modified, treatment-oriented classification of odontoid fractures. Spine J. , 2005, 5, 2, 123 -129
Acute Management • Spinal cord injury rare (17/226) • Airway compromise – 0/8 nondisplaced – 1/21 anterior displacement – 13/32 posterior displacement (2 deaths) Don’t do flexion reductions! Epidemiolgy of spinal cord injury after acute odontoid fractures JAMES S. HARROP, M. D. , ASHWINI D. SHARAN, M. D. , AND GREGORY J. PRZYBYLSKI, M. D. Neurosurgical Focus 2000 Closed management of displaced Type II odontoid fractures: more frequent respiratory compromise with posteriorly displaced fractures GREGORY J. PRZYBYLSKI, M. D. , JAMES S. HARROP, M. D. , AND ALEXANDER R. VACCARO, M. D. Neurosurgical Focus 2000
Definitive Treatment Options Type 1 C-Collar beware unrecognized CCD Evidence-based analysis of odontoid fracture management. Authors: Julien, T. D. ; Frankel, B. ; Traynelis, V. C. ; Ryken, T. C. Source: Neurosurg. Focus. , 2000, 8, 6, e 1, United States Type 3 C-Collar 10 -15% nonunion SOMI brace Halo Vest
Treatment Options odontoid fracture Type 2 • • • C-Collar SOMI / Minerva Halo Vest Odontoid Screw C 1 -2 posterior fusion
Anterior Odontoid Screw Fixation Indications • • • Displaced Type II, Shallow Type III Polytrauma patient Unable to tolerate halo-vest Early displacement despite halo-vest (Reduces in extension) • • Non-reducible odontoid fracture (Reduces in flexion) Body habitus (Barrel chest ) Associated TAL injury Subacute injury (> 6 months) Reverse oblique (elderly) Contraindications Roy-Camille Classification
Anterior Screw History Note reduced dorsal cortex
Anterior Screw Technique • Skin incision at C 5 • Note slight extension • Missing key element in diagram (need to atraumatically obtain open mouth fluoroscopy) • Biplanar fluoroscopy Direct anterior screw fixation for recent and remote odontoid fractures. Authors: Apfelbaum, R. I. ; Lonser, R. R. ; Veres, R. ; Casey, A. Source: J. Neurosurg. , 2000, 93, 2 Suppl, 227 -236, UNITED STATES
Anterior Screw Technique • Need to enter body caudal portion of promontory • Midline for single screw placement Direct anterior screw fixation for recent and remote odontoid fractures. Authors: Apfelbaum, R. I. ; Lonser, R. R. ; Veres, R. ; Casey, A. Source: J. Neurosurg. , 2000, 93, 2 Suppl, 227 -236, UNITED STATES
Anterior Screw Technique • Critical to cross rostral cortex • Critical to use lag screw technique • Limited support for second screw Direct anterior screw fixation for recent and remote odontoid fractures. Authors: Apfelbaum, R. I. ; Lonser, R. R. ; Veres, R. ; Casey, A. Source: J. Neurosurg. , 2000, 93, 2 Suppl, 227 -236, UNITED STATES
Posterior Odontoid Stabilization
Posterior Odontoid Stabilization • Options – Posterior wiring • Up to 25% pseudoarthrosis • Halo vest necessary (? ) Dickman JNS 1996, Grob Spine 1992 – Transarticular screw fixation • Magerl and Steeman Cerv Spine 1987 • Reilly et al, JSD 2003 – C 1 lateral mass - C 2 pars/pedicle/lamina screw
Wiring Techniques Biomechanical comparison of C 1 -C 2 posterior arthrodesis techniques. Authors: Papagelopoulos, P. J. ; Currier, B. L. ; Hokari, Y. ; Neale, P. G. ; Zhao, C. ; Berglund, L. J. ; Larson, D. R. ; An, K. N. Source: Spine, 2007, 32, 13, E 363 -70, United States
Trans-articular Screw Technique Primary posterior fusion C 1/2 in odontoid fractures: indications, technique, and results of transarticular screw fixation Authors: Jeanneret, B. ; Magerl, F. Source: J. Spinal Disord. , 1992, 5, 4, 464 -475, UNITED STATES
C 1 C 2 Segmental Instrumentation Posterior C 1 -C 2 fusion with polyaxial screw and rod fixation. Authors: Harms, J. ; Melcher, R. P. Source: Spine, 2001, 26, 22, 2467 -2471, United States
pedicle Pars Trans-articular C 2 pars/pedicle
Traumatic Spondylolisthesis Axis (Hangman’s Fracture) Second most common fracture of axis 25% of C 2 injuries Most common mechanism of injury is MVA
Hangman’s Fracture Younger age group (Avg 38 yrs) Usually due to hyperextension-axial compression forces (windshield strike) Neurologic injury seen in only 5 -10 % decompresses canal) Traditional treatment has been Halo-vest Collar adequate if < 6 mm displaced Coric et al JNS 1996 (acutely
Where Cranio-cervical meets Subaxial Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985; 67: 217 -226
Hangman Fracture • Intact disk defines Type I • Halo treatment difficult with torn disk (types II and III) • Exercise caution Dysphagia and Dysphonia Resolved immediately with halo adjustment
Hangman’s Fracture Treatment Types II and III Treatment Posterior – Open reduction and C 1 -C 3 fusion – Direct pars repair and C 2 -C 3 fusion Anterior – C 2/C 3 ACDF with instrumentation
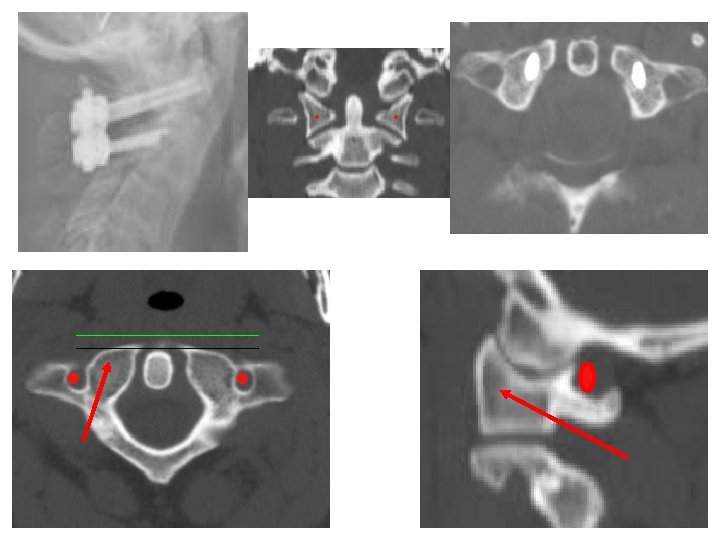
Atlanto-axial Rotatory Subluxation Fuentes et al Traumatic atlantoaxial rotatory dislocation with odontoid fracture: case report and review. Spine 2001; 26(7) 830 -834
Atlanto-axial Rotatory Subluxation • • Traction/halo Posterior fusion Lateral facetectomy, reduction, fusion Transoral facetectomy, reduction, fusion
Thank you