Updates in Diabetic Nephropathy Rodica PopBusui M D

Updates in Diabetic Nephropathy Rodica Pop-Busui, M. D. , Ph. D Division of Metabolism, Endocrinology and Diabetes Michigan Comprehensive Diabetes Center University of Michigan

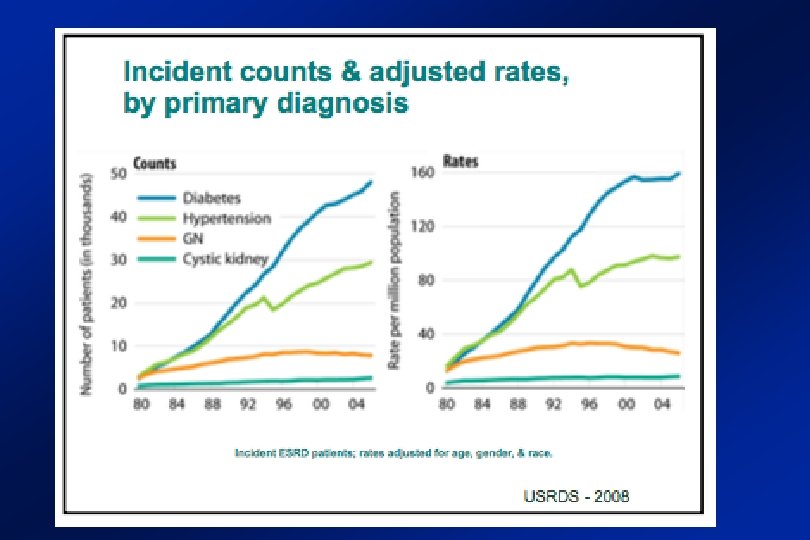
Diabetes is the dominant cause of ESRD in USA Incident ESRD patients; rates adjusted for age, gender, & race. USRDS 2013

Incidence of ESRD Among Patients with Type 1 Diabetes Number of new cases +1600 Overall a greater than 35% increase in ESRD in T 1 D in the USA in the last 25 years -100 -250 RASS Group Rosolowsky, Krolewski, et al, JASN 22: 545, 2011 USRDS 2008 5

Pathology of diabetic nephropathy Normal Glomerulus Early Diabetic Glomerulus Podocyte damage & loss Thickened BM Capillary lumen Basement membrane Mesangial cell Mesangium – Afferent and efferent hyaline arteriolosclerosis – Interstitial fibrosis and tubular atrophy Expanded mesangium

Progression of diabetic nephropathy Renal preglomerular vasodilation Systemic hypertension Glomerular hypertension Hyperglycemia Genetic factors Ox stress Inflammation Glomerular sclerosis and tubulointerstitial fibrosis from T. Hostetter

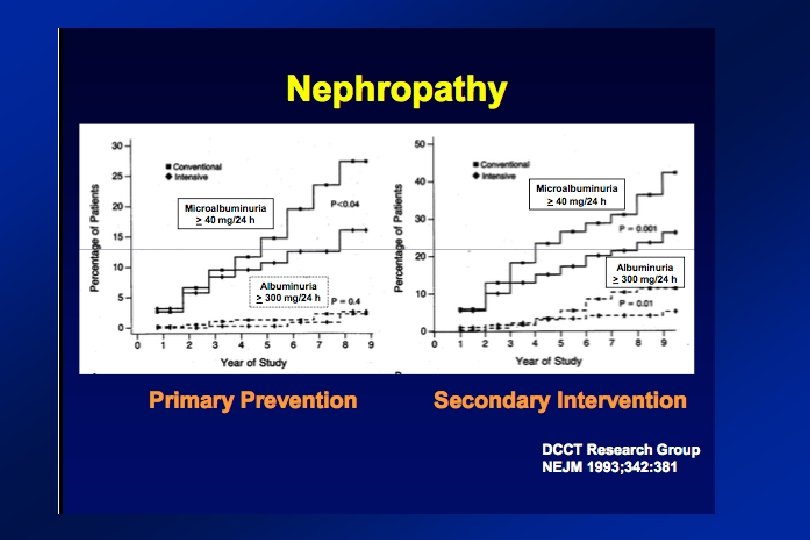
Current strategies to prevent kidney function loss on in diabetes Intensive glycemic control Nephropathy Incidence during EDIC DCCT, NEJM 1993 N Engl J Med. 2011 Dec 22; 365(25): 2366 = Metabolic memory

Current strategies to prevent kidney function loss on in diabetes RAAS Inhibition Lewis et al, NEJM 1993

Limits of RAAS inhibitors in preventing kidney function loss in diabetes GFR ≤ 50 -60 ml/min GFR >50 -60 ml/min From Lewis et al, NEJM 1993

Prevention of nephropathy ACEIs vs. ARBs? ? ? “Early blockade of the renin-angiotensin system in patients with type 1 diabetes did not slow nephropathy progression but slowed the progression of retinopathy. ” RASS Study N Engl J Med. 2009 Jul 2; 361(1): 40 -51.

Treatment of diabetic nephropathy: Effect of ACEIs PLUS ARBs Now we know for sure

DN progression, decline in GFR, without development of albuminuria in T 1 and T 2 DN Perkins, et al. J Am Soc Nephrol 2007; 18: 1353– 1361.
 82, 1010– 1017")
DN pathology precedes clinical disease Kidney International (2012) 82, 1010– 1017

Serum uric acid predicts CKD risk in the general population Baseline Serum Uric Acid (mg/dl) Q 1 (1. 50 -4. 49) n=3, 499 12 -year follow-up (Ref. ) Q 2 (4. 50 -5. 39) Q 3 (5. 40 -6. 29) Q 4 (6. 30 -14. 50) Adjusted Odds Ratio of CKD ≤ 3 Adapted from Domrongkitchaiporn et al, JASN 2005

Serum uric acid predicts albuminuria in the type 1 diabetic population • Steno Diabetes Center • T 1 D inception cohort • n=270 • 18 -yr follow-up • Outcome: Macroalbuminuria Hovind et al. Diabetes 2009

Serum uric acid predicts GFR loss in the type 1 diabetic population • Joslin Kidney Study (n=355) • T 1 D Natural History cohort • Baseline GFR >60 ml/min/1. 73 m 2 • 6 -yr follow-up • Outcome: GFR loss (>3. 3%/yr) Ficociello et al. Diabetes Care 2010

Serum uric acid predicts CKD in the type 2 diabetic population • Verona Diabetes Study (n=1, 449) • T 2 D, no proteinuria, GFR ≥ 60 ml/min/1. 73 m 2 • 5 -yr follow-up • Outcome: CKD (GFR <60 ml/min/1. 73 m 2 or proteinuria), n=194 Zoppini et al. Diabetes Care 2012
- Slides: 27