Update in Paediatric Sleep Medicine Dr Scott Burgess

Update in Paediatric Sleep Medicine Dr Scott Burgess Ph. D FRACP Paediatric Sleep and Respiratory Physician

Outline and learning objectives Improve understanding of: Common paediatric medical sleep problems Common behavioural sleep problems How much sleep children need? What is a sleep study? Questions at end.

Case 1: Sleep Noah is a 4 ½ yo boy. Parents’ main concerns are his night waking and daytime function Seen by ENT who has recommend T’s and A’s – enlarged tonsils Typical sleep He needs his parents to be with him Takes 1 -2 h to fall asleep (often by 9 -10 pm) Averages 8 -9 h sleep / night Wakes multiple times and comes into his parents’ bed He is a very restless sleeper, always kicking his legs Snores but no witnessed apnoeas Background: He is a picky eater Impulsive, has problems interacting with other children at preschool. He has been seen by a paediatrician who has suggested he may have ADHD What potential sleep problems does Noah have?

Obstructive sleep apnoea OSA is characterised by: Recurrent episodes of partial or complete upper airway obstruction during sleep Disruption of normal gas exchange intermittent drops in oxygen or hypercapnoea Sleep fragmentation poor quality sleep.

Frequency of snoring / OSA 25% children snore intermittently, especially with colds 10% - loud snoring, => 3 times per week 2% of children have OSA.

Pathophysiology OSA is associated with narrowing or collapse of the upper airway during inspiration. Typically at the level of the soft palate and adenoids (Isono, Shimada et al. 1998).

Predisposing factors Shape, size and collapsibility of the airway: Inherited – family history is common Medical conditions – eg. Down syndrome Sleep state: dreaming sleep - low muscle tone and altered breathing Adenotonsillar hypertrophy: growth of adenoids and tonsils relative to the airway, peaks from 2 -8 years Exposure to cigarette smoke and recurrent viral URTIs Obesity: effects of tissue in the neck, abdomen and blunted respiratory drive.

Consequences � Like most disorders that affect sleep quality, OSA is associated with: � Poor attention and concentration � Hyperactivity and impaired impulse control � Moodiness / increased tantrums � Sleepiness – uncommon symptom, less common than in adults � Impaired learning � Reduced scores on psychometric (IQ) testing � Severe cases - effects growth and cardiovascular health.

Treatment of OSA Treatment depends upon severity and cause �Medical treatment: eg. Nasal steroid or Singulair �Weight loss �Remove cigarette smoke exposure �ENT surgery: T’s and A’s, or other surgery �CPAP – second line or complicated cases �Other treatments.

Behavioural insomnia of childhood • Most common sleep problem • Limit setting type- Resistance going to bed or coming out soon after being put to bed (curtain calls) • Sleep onset association disorder – Independent = needs toy, blanket etc. to go to sleep but not a person – Dependent = needs input from someone else to go or return to sleep Waking during the night – It is normal to wake multiple time during the night – Most children can return to sleep quickly by themselves – Common presentation of SOAD.

Management of Behavioural insomnia Parental education Structured night time routine and consistent bedtime Child needs to learn to go to sleep independently Parent gradually fades out as child goes to sleep Can be stressful but is not harmful Parents need: Clear plan and understanding of what they are doing To be consistent each night and between carers Support Diary – helps parents stay on track Rewards – motivate child to have a go Key point – do not swap one association for another.
")
Restless legs syndrome Affects 2 -4% of school aged children, under diagnosed RLS (definition) An urge to move the legs, often associated with an unpleasant sensation Begins or worsens during periods of rest or inactivity, lying or sitting Partially or totally relieved by movement such as walking or stretching More common in the evening or night Not due to another medical condition History – explore symptoms in the child’s own words Often family history of RLS Differentiated from growing pains, GPs = movement makes worse Commonly associated with Periodic Limb Movement Disorder Stereotyped, repetitive and periodic lower limb movements detected by leads which measure muscle movement during a sleep study.

RLS and PLMS are associated with Trouble going to sleep Disrupted / restless sleep Problems with daytime function The cause is unknown but likely due to abnormalities in neurotransmitters Dopamine and Glutamate Low brain iron strongly associated (iron affects Dopamine receptors and transporters) Ferritin often low and symptoms typically improve with supplemental iron if ferritin increased >50 Dopamine traditionally used in adults but problematic and rarely used in children. Anti-epileptic medicine Gabapentin helps with sleep quality and better tolerated High prevalence in ADHD, ASD and several medical conditions Exacerbated by some medicines: SSRI / SNRI’s.

How much sleep do children need? There is significant individual variation 5 nights of sleep deprivation followed by 2 night of catch up sleep does not return a young person to their functional baseline There are high rates of young people having insufficient sleep Insufficient sleep has been shown to: Impair cognition and learning Result in increased risk taking behaviours / problematic behaviours Negatively impact on mood and weight Compound negative effects of other sleep problems.

Recommended sleep durations Age Recommended duration 4 -12 months 12 -16 h* 1 -2 years 11 -14 h* 3 -5 years 10 -13 h* 6 -12 years 9 -12 h 13 -18 years 8 -10 h *This is total sleep for 24 hour period and includes naps / daytime sleep AASM recommended guideline - 2016

What is a sleep study?
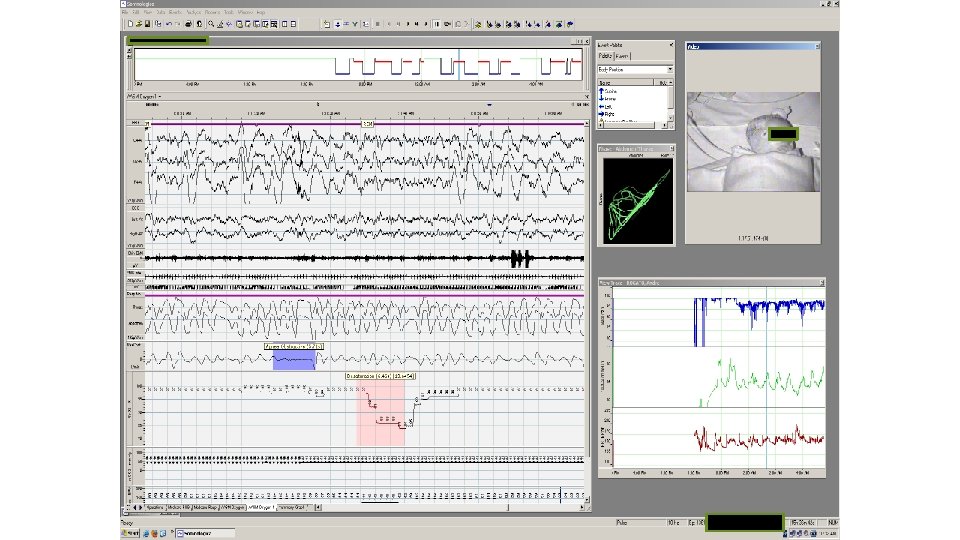

Sleep tests Sleep study Actigraphy Sleep quality and breathing in sleep Sleep patterns and sleep duration at home Mean sleep latency test Objective measure of sleepiness and diagnostic test for narcolepsy.

Case 1: Sleep Noah is a 4 ½ yo boy. Parents’ main concerns are his night waking and daytime function Seen by ENT who has recommend T’s and A’s – enlarged tonsils Typical sleep He needs his parents to be with him Takes 1 -2 h to fall asleep (often by 9 -10 pm) Averages 8 -9 h sleep / night Wakes multiple times and comes into his parents’ bed He is a very restless sleeper, always kicking his legs Snores but no witnessed apnoeas Background: He is a picky eater Impulsive, has problems interacting with other children at preschool. He has been seen by a paediatrician who has suggested he may have ADHD What potential sleep problems does Noah have?

Summary: Possible problem Evaluation Management Insufficient sleep History or actigraphy Education and support Sleep onset association disorder History Education and support OSA Sleep study ENT surgery RLS / PLMS History, blood tests and sleep study Iron

Thank you

Questions? What is the first letter in the English alphabet?
- Slides: 22