united for health Third World Health Aid Training




")








 Bandung Conference in 1955 with independent African and Asian States")





 Political answer to the crisis •")

 or “The Cure that makes")


 and transnational (TNC) companies grew")










- Slides: 36
united for health Third World Health Aid Training module: Access to health care The political economy of global health policy
Objective of the session Introduction to political and economic determinants of global health policy in a historical perspective
Programme 1. Introduction 2. Group work: 'Time line' 3. Presentation
Remember: What is “Health”? “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. "
What are the social determinants of health? (Solar&Irwin 2010)
What is political economy of global health policy? Politics = Asking the question “Who gets what and why? ” Questions: - Where is global health policy decided upon? - Who sets the priorities? -… History can help us analyse and understand.
Group work: Timeline Put the cards with events on the timeline and explain the link of this event with health and/or health policy.
End WW 2 1944 Bretton Woods: IMF, WB 1947: GATT NHS & social security systems 1948 WHO UN Decolonization Neoliberalism Alma Ata Globalization WB Report Investing in Health GHI’s WHO WHR 2008
At the heart of the debate: The role of the state in health Polarized debate: • “Health is an individual responsibility and health care is a commodity” (ex : US “self help” model) versus • “Health is a human right and health care shouldn't exclude people based on financial means or socioeconomic status” (ex : European health systems based on “social solidarity”) This debate has influenced health system developments in developing countries.
Birth of the “international community” • 1944: Bretton Woods Conference: • IBRD executes Marshall Plan > Becomes World Bank Group (5 institutions). 187 Member States. Voting rights defined by economic power of shareholders of the Bank (1 dollar 1 vote) • International Monetary Fund (IMF): 188 members. Aim is financial stability, cooperation, international trade and economic growth. • UN 1948: Multilateral system of international collaboration • World Health Organization (WHO): Specialized health agency of the UN: 1 country 1 vote • World Trade Organization (WTO): Created in 1995, grown from GATT 1947. 160 Member States. Aim is facilitating international trade with inclusion of dispute settlement mechanisms in trade agreements.
“Forum shopping” at a global level • Between WHO, WB etc: Countries chose forums to discuss issues according to their national interests • Political analysis: Which interests are these and why? Is global health policy a purely technical issue? Or are there political and economic interests that determine global health policy?
Universal Declaration of Human Rights Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control UN General Assembly, December 10 th 1948, Article 25 -1 = First reference to the ‘right to health’
End of WWII 1945 1960 1970 1980 1990 2000 2010 Decolonisation First succesful independence movements: India, Pakistan, Philippines, Indonesia, . . . Congo 1960
The Non-Aligned Movement (NAM) Bandung Conference in 1955 with independent African and Asian States gave rise to the NAM finally established in Yugaslavia in 1961 New international economic order, 1974 (opposes Bretton Woods system) Havana Declaration, 1979 The national independence, sovereignty, territorial integrity and security of non-aligned countries in their struggle against imperialism, colonialism, neocolonialism, racism
60's Power struggle within WHO: 1 country 1 vote Developing countries are majority in WHO General Assembly → power relations change → WHO comes under pressure: Call for preventive action Growing attention for social determinants Development of ‘primary health care’ logic
70's: WHO reviews its strategy Successful community health initiatives in India, the Philippines, Bangladesh, Costa Rica, Cuba, Mexico, Nicaragua, Guatemala, … China’s bare foot doctors Central America: social movements for health, social justice and human rights USSR campaigns for ‘health systems policy’ … → 1977 Health for all WHO General Assembly adopts resolution → 1978 Alma Ata Conference WHO and UNICEF
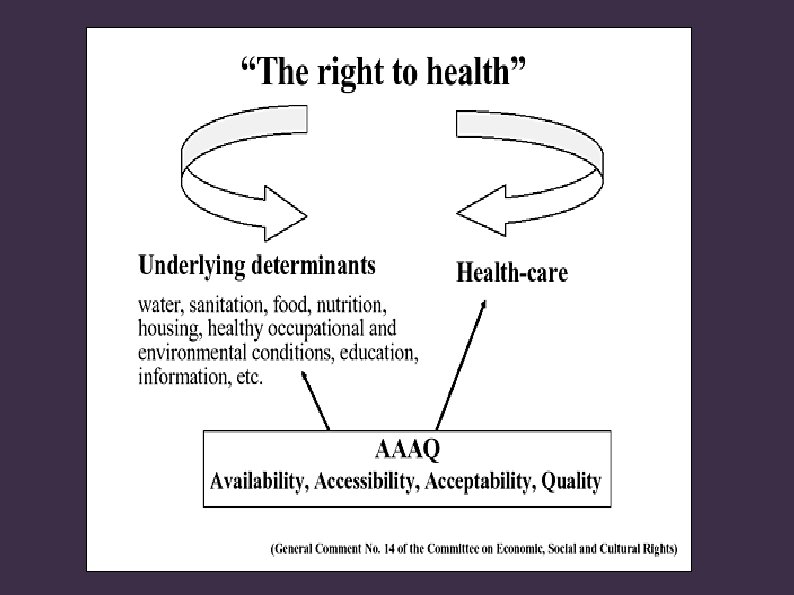
Alma-Ata Conference 1978 Integrated health and health services strategy Right to health & healthcare Responsibility of government Universal access Multi-sectorial approach Participation Comprehensive approach to health Call for New International Economic Order
Horizontal versus vertical approaches 1979 : Bellagio symposium of Rockefeller Foundation: Start of counter offensive against Comprehensive Primary Health Care (horizontal): CPHC is “idealistic, costly, not realistic”. Campaign for Selective Primary Health Care as an alternative: • • 'intermediary solution' focus on mother and child health rapid progress is possible with new techniques technical criteria decide on priority problems: incidence, prevalence, morbidity, mortality, feasibility, efficiency, cost, … → Attention moves from health to diseases
Foto Reagan & Thatcher Neoliberale maatregelen van beide Antivakbond Sandinisten/FMLN/Etc 80's: neoliberalism
Neoliberalism? Washington consensus Bretton Woods institutions (WB, IMF) Political answer to the crisis • Shrinking of the state → Less government control over the economy • • Free markets and deregulation: encouraging trade and investments by removing 'trade barriers' (= government regulations: technical requirements, taxes, . . . ) Privatisations: enhancing the role of the private sector in public services (health, public transport, . . . )
80's Power struggle within WHO 1981 WHO/UNICEF International Code of Marketing of Breast-milk Substitutes adopted (34 th. WHA): Sole opposing vote coming from the US: code perceived as interference in marketing practices Economically powerful states freeze the regular budget → WHO in financial crisis → Increase of 'extrabudgettary' donations = earmarked voluntary donations for selective interventions Voluntary funding means that global health agenda is skewed towards donor interests rather than health needs worldwide.
Meanwhile: IMF and WB = Structural Adjustment Programmes (SAPs) or “The Cure that makes the disease worse”: Loans with conditions attached, austerity, privatization → People living in poverty are first victims, destroyed health systems and low morale health workers Followed by Poverty Reduction Strategy Papers (PRSPs): Still development aid with conditions, but more reasonable: “SAP with a human face”
90's : World Bank takes the lead • • • From 'reconstruction and development' now also 'development aid' Within World Bank → largest economies have most power 1993 World Development Report Investing in health = promoting enhanced private -for-profit sector
Health sector as a business opportunity No universal access to health care from commercial sector provision of services: • User fees: private serves the wealthy (the poor use the more affordable) public sector • Operates mainly in urban areas underserved rural areas (where majority in developing countries live) • Mainly highly technological hospitals little attention for basic preventive services • Creating “neglected diseases”: does not invest in nonprofitable diseases (lassa, ebola, etc…)
Globalization? = “transnationalism”: from 1970 to 2000 Multinational (MNC) and transnational (TNC) companies grew in number from 7, 000 to 53, 600 • • Placing parts of production process in # countries: e. g. extract resources in Africa, production in Asia, sales in Europe and waste back to Africa. MNCs and TNCs are based in wealthy countries: profits flow to wealthy countries → inequality between rich and poor countries • Accumulation of profits: 200 TNCs > 182 states (80% world population) → inequality between rich and poor within countries • Globalisation → widening gap between rich and poor.
Impact on health? • On a global level: global economy • On a national level: individual health risks, household economy and health system Woodward et al, WHO 2001
Free Trade and health • Trade Agreements under WTO: • GATS : General Agreement on Trade in Services; liberalization of services, including the health sector. • TRIPS: Trade Related Intellectual Property Rights, including patents on medicines • After DOHA round in 2001: States circumvent WTO by negotiating bilateral and regional Trade and Investment Agreements (ex: TTIP, TISA) → Impact on health • Inclusion of dispute settlement mechanisms means that trade agreements are binding, while health guidelines aren't binding. Consequence? Trade trumps health.
UN Millennium Development Goals
2000's Global Health Initiatives Public-private partnerships Global Fund to fight AIDS, TB and Malaria (GFATM), PEPFAR (U. S. President’s Emergency Plan for AIDS Relief), Bill & Melinda Gates Foundation, Roll back Malaria, Global Alliance for Vaccines and Immunization (GAVI), . . . Global Health Initiative World Economic Forum (WEF): While the UN members are governments, ours come mostly from the field of business. Committed to improving the state of the world. → Privatization of global health
2008
“The toxic combination of bad policies, economics, and politics is, in large measure, responsible for the fact that a majority of people in the world do not enjoy the good health that is biologically possible … Social injustice is killing on a grand scale” www. who. int/social_determinants/final_report (6)
What good does it do to treat people's illnesses. . . and then send them back to the conditions that made them sick? (Michael Marmot, CSDH)
Conclusion - International power relations and political economy influence global health agenda's. - Polarized debate: 'Right to health' versus 'health sector as a business opportunity'
Réferences • Backman, G. , 2008. Health systems and the right to health: an assessment ofr 194 countries. • Blouin, C. , Chopra, M. & van der Hoeven, R. , 2009. Trade and social determinants of health. The Lancet, 373(9662), pp. 502– 507. • Dodgson, R. , Lee, K. & Drager, N. , 2002. Global Health Governance, a conceptual review. , (1). • Gilson, L. et al. , 2007. Challenging inequity through health systems. Final Report of the Knowledge Network on Health Systems, • Kickbusch, I. , 2000. The development of international health policies-accountability intact? Social science & medicine (1982), 51(6), pp. 979– 89. • Koivusalo, M. & Schrecker, T. , Globalization and Policy Space for Health and Social Determinants of Health. • Labonte, R. & Schrecker, T. , 2006. Globalization and social determinants of health Analytic and strategic review paper, • Labonté, R. & Schrecker, T. , 2007. Globalization and social determinants of health: Introduction and methodological background (part 1 of 3). Globalization and health, 3, p. 5.
• Mc. Pake, B. & Mills, a, 2000. What can we learn from international comparisons of health systems and health system reform? Bulletin of the World Health Organization, 78(6), pp. 811– 20. • Ottersen, O. P. et al. , 2014. The Lancet – University of Oslo Commission on Global Governance for Health The political origins of health inequity prospects for change. The Lancet, 6736(13). • Ranson, M. K. & Mills, A. , 2000. The Design of Health Systems. , pp. 513– 552. • Smith, R. D. , 2010. The Role of Economic Power in Influencing the Development of Global Health Governance. Global health Governance, 3(2). • Smith, R. D. & Hanson, K. , 2012. What is a health system? In Health systems in low- and middle-income countries: An economic and policy perspective. pp. 1– 16. • Smith, R. D. , Lee, K. & Drager, N. , 2009. Trade and health: an agenda for action. Lancet, 373(9665), pp. 768– 73. • De Vos, P. & Van der Stuyft, P. , 2015. Sociopolitical determinants of international health policy.