UNIT1 CHRONIC SUPPURATIVE OTITIS MEDIA PRESENTED BY Ms

UNIT-1 CHRONIC SUPPURATIVE OTITIS MEDIA PRESENTED BY: Ms. Pavithra K Lecturer, MSN dept

LEARNING OBJECTIVES At the end of the class students will be able to • define CSOM • enlist the types of CSOM • describe the Patho-Physiology of CSOM • list down the clinical features of CSOM • Enlist the diagnostic features of CSOM • enumerate the management of CSOM

INTRODUCTION • Is a chronic inflammation of the middle ear mucosa with tissue damage usually caused by repeated episodes of acute otitis media • Antibiotic resistant organism • Treatment failure

DEFINITION • CSOM is the inflammation of the middle ear cleft mucosa characterized by chronic purulent discharge from the middle ear. It is the result of repeated episodes of acute otitis media causing irreversible, pathological changes and persistant perforation of the tympanic membrane

ETIOLOGY • Bacteria – – Streptococcus Staphylococcus Proteus Pseudomonas • Acute otitis media • Congenital Cholesteatoma

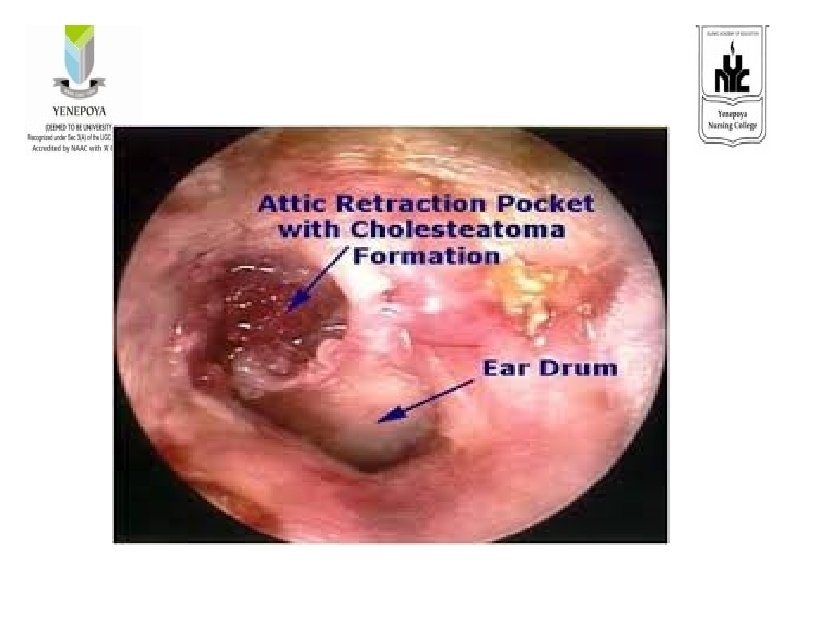
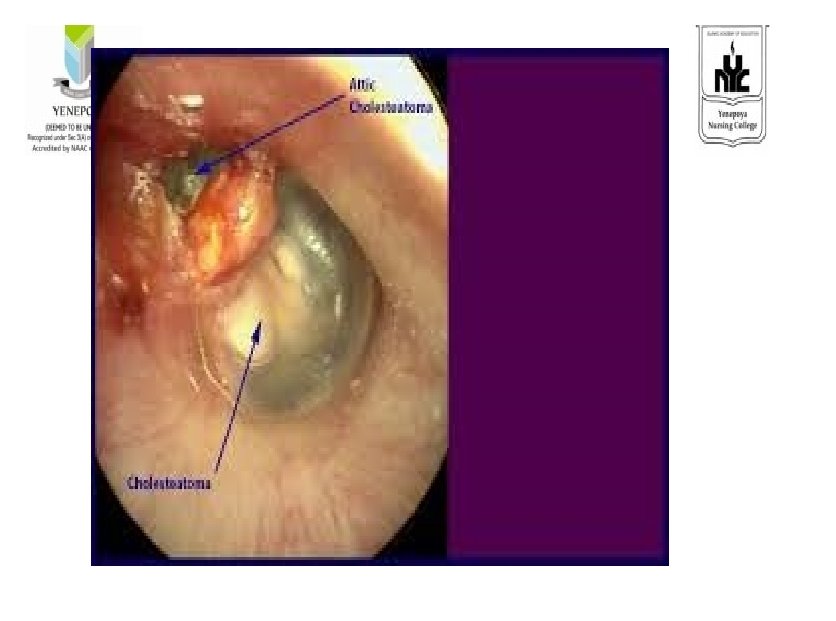
CHOLESTEATOMA • Abnormal, noncancerous skin growth • Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear.

Types • Tubotympanic • Atticoantral

TUBOTYMPANIC • • • Benign Profuse, mucoid, odourless discharge Central perforation of the ear drum Limited to the tympanic membrane and eustachian tube Pale Polyp No complications

ATTICOANTRAL • • Dangerous Scanty, purulent , foul smelling dischrage Marginal perforation Beyond the tympanic membrane Cholesteatoma Granulations Red and flesh polyp complications

Pathophysiology – tubotympanic Etiology Necrosis of ear drum Necrosis of ossicles Sclerosis of mastoid bone Polyp formation

ATTICO ANTRAL Cholesteatoma formation Granulation Retraction and Perforation of the ear drum Complete damage to the ossicles Conductive Hearing loss

CLINICAL MANIFESTATIONS • • ASOM clinical manifestations Persistent blockage or fullness of the ear Chronic ear drainage balance problems Facial weakness Persistent deep otalgia Fever with chills

DIAGNOSTIC EVALUATION • • • History collection Physical examination Otoscopy Culture and sensitivity of ear discharge x-ray of the mastoid antrum CT/ MRI

COMPLICATIONS Mastoid Infection • Mastoiditis • Mastoid abscess Extra cranial Complications • Petrositis • Facial nerve palsy • labyrinthitis

Intracranial complications • Extradural abscess • Subdural abscess • Meningitis • Brain abscess • Hydrocephalus

MANAGEMENT GOALS: • To relieving the discomfort • To reduce the swelling • To eradicating the infection

PHARMACOLOGICAL MANAGEMENT • • • Amoxicillin -80 -90 mg / kg Amoxicillin – 90 mg/kg Azithromycin – 30 mg/kg (3 day course , ROM) Clarithromycin – 15 mg/kg Clindamycin – 30 -40 mg/kg Ceftriaxone – 50 mg/ kg

Analgesics • Severe • Actetaminophen – 15 mg • Ibuprofen- 10 mg • Diclo- 10 mg Nasal decongestants Antihistamines

AURAL TOILET • • • Dry moping Jobson horne probe is used to clear the external auditory meatus debris, discharge, soft wax or excess fluid Improve conduction of sound to the tympanic membrane. Removeing debris will allow to examine the external auditory meatus and the tympanic membrane.



MASTOIDITIS • • Prolonged antibiotherapy ceftriaxone IM for 10 days + ciprofloxacin PO for 14 days, cleaning of the ear canal surgical treatment

SURGICAL MANAGEMENT Myringotomy : • A small incision is made in the eardrum to allow fluid to drain and keep the eardrum from rupturing Myringoplasty • Myringoplasty is the closure of the perforation of pars tensa of the tympanic membrane.

• Tympanoplasty is the surgical operation performed for the reconstruction of the eardrum (tympanic membrane) and/or the small bones of the middle ear (ossicles). • Ossiculoplasty : It is the surgical reconstruction of the middle ear bone to restore hearing

• Adenoidectomy : It is a surgical procedure to remove the adenoids • Mastoidectomy ; It involves incision , drainage and surgical repair of the mastoid process

NURSING DIAGNOSIS • Acute pain related to inflammation and increased pressure in the middle ear as evidenced by pain scale score • Disturbed sensory perception , Auditory related to inflammation and edema in the middle ear as evidenced by hearing acuity test • Deficient knowledge regarding the disease condition and therapeutic regimen as evidenced by frequent doubts • Impaired verbal communication related to decreased hearing as evidenced by frequently asking to repeat.

ACUTE PAIN • Assess the characteristics of pain- severity, type • Advice the client to lie down in side lying position with affected ear downwards and raise head with pillow. • Hot water bag • Ice pack application • Analgesics • Antibiotics

Disturbed sensor perception , Auditory • Assess the clients hearing ability • Reduce unnecessary environmental noise • Encourage the family members to speak in a loud and clear voice • Notify the changes in hearing ability • Reassure the patient hearing loss is not permanent and will resolve with treatment. • Strict adherence to the antibiotic treatment

CONCLUSION • Chronic otitis media is a long-standing, persistently draining perforation of the eardrum (tympanic membrane). Acute otitis media and blockage of a eustachian tube are among the causes of chronic otitis media. A flare-up may occur after a cold, an ear infection, or after water enters the middle ear.

EVALUATION • • • What is CSOM. What are the causes of CSOM. Enumerate the patho-physiology of CSOM. Enlist the clinical features of CSOM. Explain the management of CSOM.

REFERENCE • Smeltzer – Brunner & Suddharth Textbook of Medical Surgical Nursing, Wolters kluwer publishers, 12 th edition 2009. • Black – Medical Surgical Nursing, Elsevier publishers, 8 th edition 2009. • Nettina – Lippincott manual of Nursing Practice, Wolters kluwer publishers, 7 th edition 2014. • Lewis – Medical Surgical Nursing, Elsevier publishers, 10 th edition, 2017
- Slides: 33