Unit III Respiratory System Assessment Mrs Indumathi Lecturer






")







 odor consistency pattern of")














 and inspiration (right).")








- Slides: 42
Unit III: Respiratory System Assessment Mrs. Indumathi Lecturer YNC
Introduction • The respiratory system is situated in the thorax, and is responsible for gaseous exchange between the circulatory system and the outside world. Air is taken in via the upper airways (the nasal cavity, pharynx and larynx) through the lower airways (trachea, primary bronchi and bronchial tree) and into the small bronchioles and alveoli within the lung
Anatomy and physiology • The respiratory tract extends from the nose to the alveoli and includes not only the air-conducting passages also but the blood supply • The primary purpose of the respiratory system is gas exchange, which involves the transfer of oxygen and carbon dioxide between the atmosphere and the blood. • The respiratory system is divided into two parts: the upper respiratory tract and the lower respiratory tract
The upper respiratory tract includes • • The nose pharynx adenoids tonsils epiglottis larynx, and trachea.
The lower respiratory tract consists of • • • the bronchi, Bronchioles alveolar ducts and alveoli With the exception of the right and left mainstem bronchi, all lower airway structures are contained within the lungs.
• The right lung is divided into three lobes (upper, middle, and lower) • the left lung into two lobes (upper and lower) • The structures of the chest wall • (ribs, pleura, muscles of respiration) are also essential
Health History • History of trauma to the ribs or lung surgery • History of chest pain with deep breathing • History of persistent cough with or without producing sputum • History of allergies
• Environmental exposure to chemicals, asbestos, or smoke • History of smoking • History of lung disease in family members or self • History of frequent or chronic respiratory infections
• • • Family Health History Tuberculosis Emphysema Lung Cancer Allergies Asthma
Cough • Type – dry, moist, wet, productive, hoarse, hacking, barking, whooping • Onset • Duration • Pattern – activities, time of day, weather
• Severity – effect on ADLs • Wheezing • Associated symptoms • Treatment and effectiveness
sputum • • • amount color presence of blood (hemoptysis) odor consistency pattern of production
Physical assessment • The basic steps of the examination (can be remembered with the mnemonic IPPA): • • Inspection Palpation Percussion Auscultation
Inspection • Observe chest for color, shape, breathing patterns, and muscle development • Tracheal deviation (can suggest of pneumothorax) • The chest should be symmetric, with the transverse diameter greater than the anteroposterior diameter.
• Chest wall deformities • Kyphosis - curvature of the spine - anterior-posterior • Scoliosis - curvature of the spine - lateral
• Barrel chest - chest wall increased anteriorposterior; normal in children; typical of hyperinflation seen in COPD • Pectus excavatum(funnel chest): sunken appearance of the ches. • Pectus carinatum (pigeon chest): protrusion of sternum and chest.
• Observe for abnormal findings such as, • Increase in chest size and contour • Abnormal breathing patterns with use of accessory muscles (COPD) • Unequal chest expansion ( chest trauma & pneumonia) • Abnormal respirations.
Thoracoplasty with secondary changes in the spine
• Pectus exacavatum
• Kyphosis
Note the pursed-lip breathing
Palpation Tactile fremitus: is vibration felt by palpation. • Place your open palms against the upper portion of the anterior chest, making sure that the fingers do not touch the chest.
• Ask the patient to repeat the phrase “ninetynine” or another resonant phrase while you systematically move your palms over the chest from the central airways to each lung’s periphery. • You should feel vibration of equally intensity on both sides of the chest. Examine the posterior thorax in a similar manner.
• The fremitus should be felt more strongly in the upper chest with little or no fremitus being felt in the lower chest • Increased tactile fremitus suggests consolidation of the underlying lung tissues
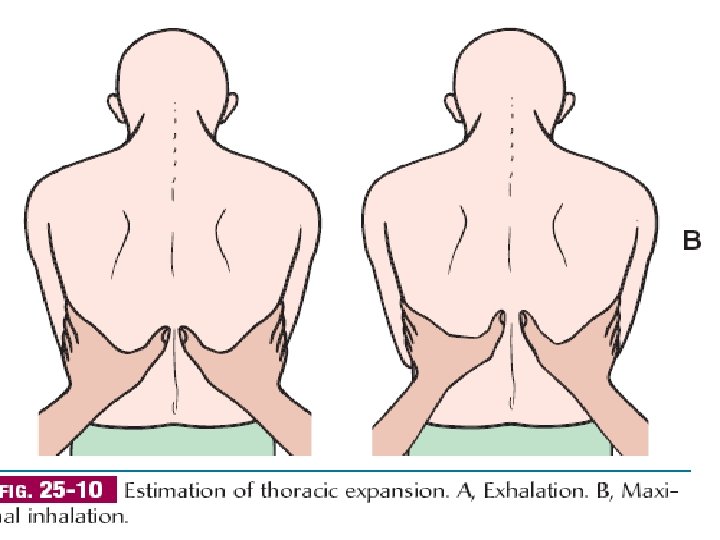
Chest expansion: is determined by placing the hands over the posterior chest wall, with the fingers at the level of T 9 or T 10. • Ask the patient to take a deep breath, and observe the movement of your thumbs. • The thorax should expand symmetrically
Assessing chest expansion in expiration (left) and inspiration (right).
Percussion Rational • To determine if underlying tissue is filled with air or solid material Procedure • Patient sitting • Tap starting at shoulder • compare right to left
Percussion: results • Resonance – drum like – Normal • Hyper-resonance – Too much air – Emphysema • Flatness / dull – – Fluid or solid Pleural effusion Pneumonia Tumor
Auscultation Purpose • Asses air flow through bronchial tree Procedure • Diaphragm of stethoscope • Superior inferior • Compare right to left
Auscultation: Results Normal • Vesicular – Lung field – Soft and low • Bronchial – Trachea & bronchi – Hollow and loud • Bronchovesicular – – Mixed Between scapulae Side of sternum 1 st & 2 nd intercostal space
Auscultation: Results Adventitious • Crackles – Rales – air bronchi with secretions • Fine crackles – Air suddenly reinflated – High pitched and soft • Course Crackles – Moist – Low pitched and louder
Auscultation: Results • Wheezes – Sonorous wheezes Deep low pitched Snoring > Expiration Caused by air narrowed passages • h secretions • • – Sibilant Wheezes High pitched Whistle-like I & E Caused by air narrowed passages • constriction • • – Asthma
Auscultation: Results • Pleural friction rub – inflammation of pleural membranes – Grating, creaking – I & E – Best heard • Anterior, Lower, lateral area
Auscultation: Results • Stridor – Crowing – Partial obstruction of the larynx or trachea