UNIT III PULMONARY TUBERCULOSIS Mrs Indumathi Lecturer YNC

UNIT III PULMONARY TUBERCULOSIS Mrs. Indumathi Lecturer YNC

OBJECTIVE • By the end of the session the student will be able to: • define tuberculosis • explain the epidemiological triad of tuberculosis • identify the mode of transmission and incubation period • discuss the clinical manifestations of tuberculosis

OBJECTIVE • explain the diagnostic measures used in early detection of TB • discuss the treatment modalities used in curative aspect of TB • enumerate the control and preventive measures • discuss the different Tuberculosis Control Program

Definition Tuberculosis is a specific infectious disease caused by M. tuberculosis that primarily affects the lung parenchyma.

It may also be transmitted to other parts of the body including the meninges, kidney, bones and lymph nodes.

Epidemiology: ♣ India accounts for nearly one third of global burden of tuberculosis. ♣ Every year approximately 1. 8 million persons develop tuberculosis of which about 0. 8 million are new smear positive highly infectious cases. ♣ About 4. 17 lakh people die of TB every year

S Prevalence of infection increased with the age, up to the age of 45 -54 years in males. In females the peak of TB prevalence is below 35 years. S Tuberculosis infection as well as disease is more or less uniformly distributed in urban, semi-urban and rural areas.

EPIDEMIOLOGICAL TRIAD

Agent Host Environment

Agent factors Agent Source of infection Communicability

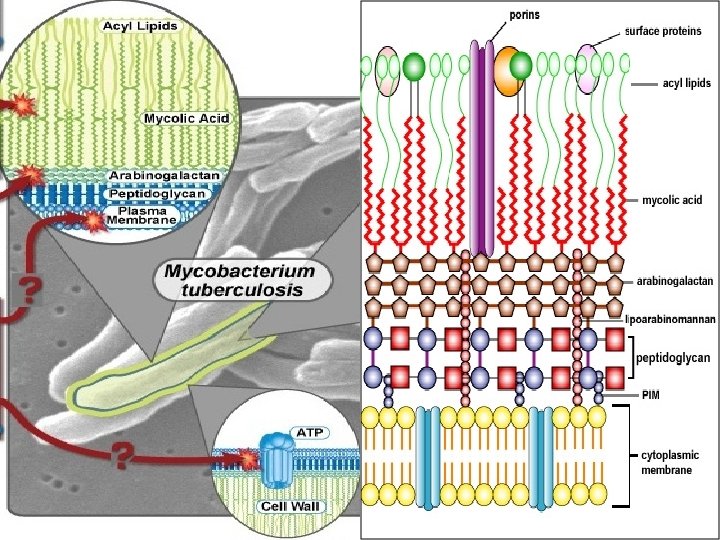
1. Agent factors : Agent M. tuberculosis is a rod-shaped, non-sporeforming, thin aerobic bacterium measuring 0. 5 µm by 3 µm.

Source of infection: There are 2 sources of infection:

2. Host factors: ô Age ô Sex ô Heredity ô Nutrition ô Immunity

3. Environmental factors:

Mode of transmission:

ô TB is not transmitted by fomites, such as dishes and other particles used by the patient. ô Patients with extra pulmonary TB or smear negative TB constitutes a minimal hazard for transmission of infection.

Incubation period: ü It ranges from 3 to 6 weeks and thereafter the development of disease depends upon the closeness of contact, extent of the disease and sputum positivity of the source case and host-parasite relationship. ü Thus the incubation period may be weeks, months or years.

Pathophysiology:

ØPrimary infection…. . îThe first time a client is infected with TB, the disease is said to be a primary infection. îPrimary TB infections are usually located in the apices of the lungs or near the pleura of the lower lobes.

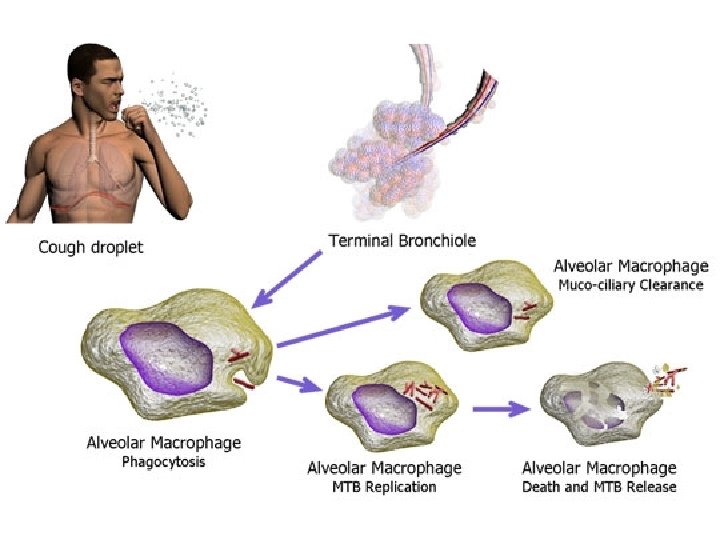
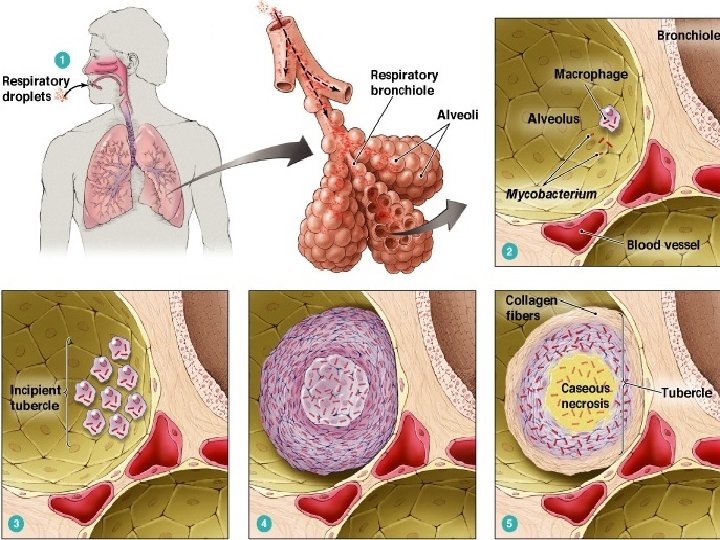
Stage 1 ♣ A susceptible person inhales droplet nuclei and becomes infected.

♣ Once nuclei are inhaled, the bacteria are nonspecifically taken up by alveolar macrophages. organism. ♣ The macrophages will not be activated, therefore unable to destroy the intracellular organism

Stage 2 ♣ Begins 7 -21 days after initial infection. ♣ MTB multiplies within the inactivated macrophages until macrophages burst.

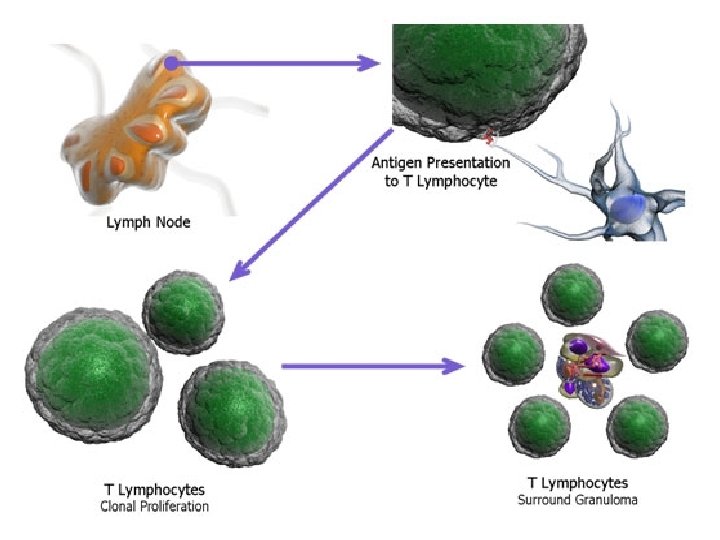
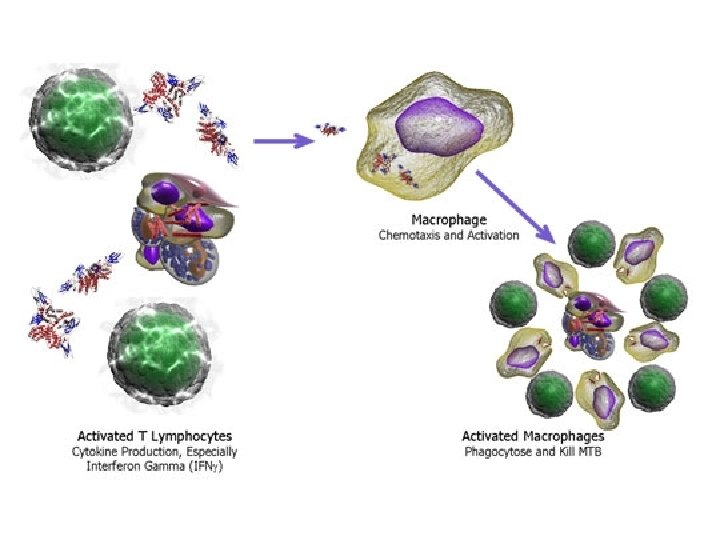
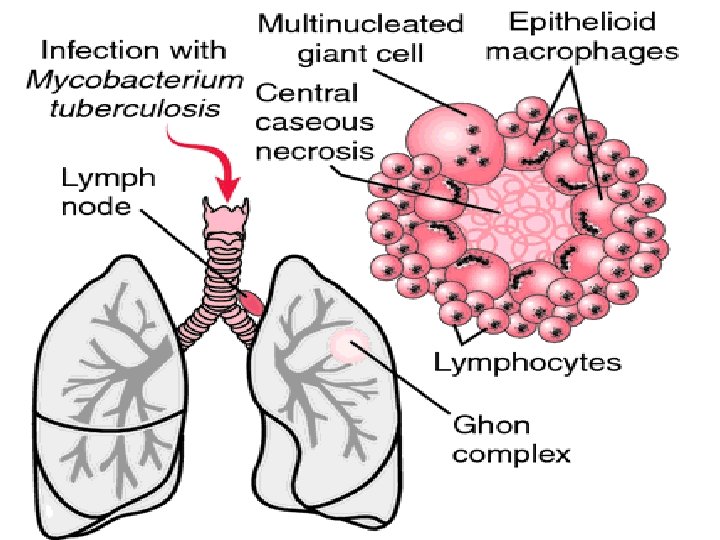
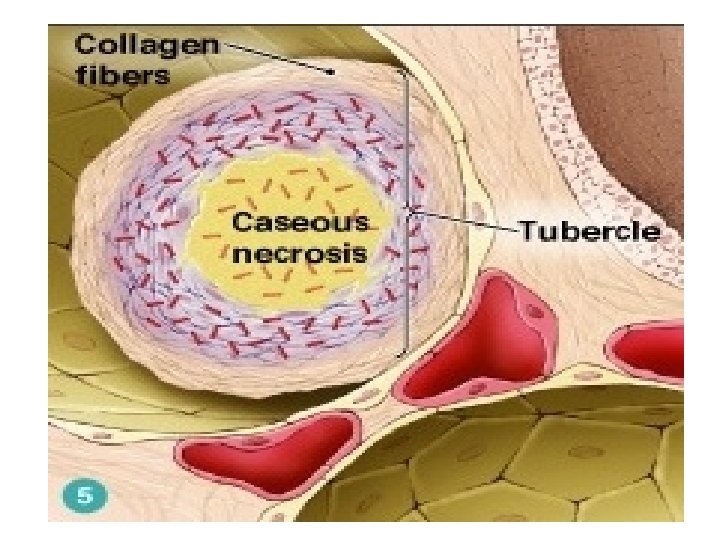
Stage 3: ♣ T cell recognition and release of cytokines and interferon ♣ Activation of macrophages and release of lytic enzymes and reactive intermediates ♣ Granulomas, new tissue masses of live and dead bacilli, are surrounded by macrophages, which form a protective wall around the Granulomas.

♣ The 10 infection site may or may not undergo a process of necrotic degeneration (caseation), which produces cavities filled with a cheese-like mass of tubercle bacilli, dead white blood cells (WBC’s) and necrotic lung tissue. ♣ This is called as “Ghon tubercle”. ♣ These lesions may contain living bacilli that can be reactivated, even after many years and cause secondary infection.

Stage 4: • Many macrophages are inactivated or poorly activated. • MTB uses these macrophages to replicate causing the tubercle to grow. • The growing tubercle may invade a bronchus, causing an infection which may spread to other parts of the lungs. • Spreading of TB may cause miliary tuberculosis, which can cause secondary lesions.

Stage 5: ♣ The caseous centers of the tubercles liquefy, may drain into the tracheobronchial tree and may be coughed up. ♣ The air filled cavities remain, and may be detected on X-ray study. ♣ This liquid is very crucial for the growth of TB, and therefore it multiplies rapidly (extracellularly). ♣ This later becomes a large antigen load, causing the walls of nearby bronchi to become necrotic and rupture.

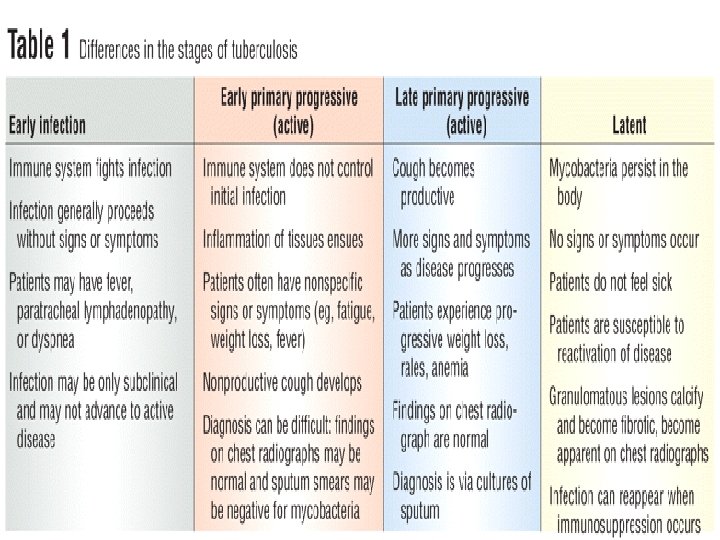
Secondary infection…. • After initial exposure and infection, the person may develop active disease because of compromised or inadequate immune system response. • Active disease also occurs with reinfection and activation of dormant bacteria. • It most commonly occurs within the lungs, usually in the apical or posterior segments of the upper lobes or the superior segments of the lower lobes.

Clinical manifestations:
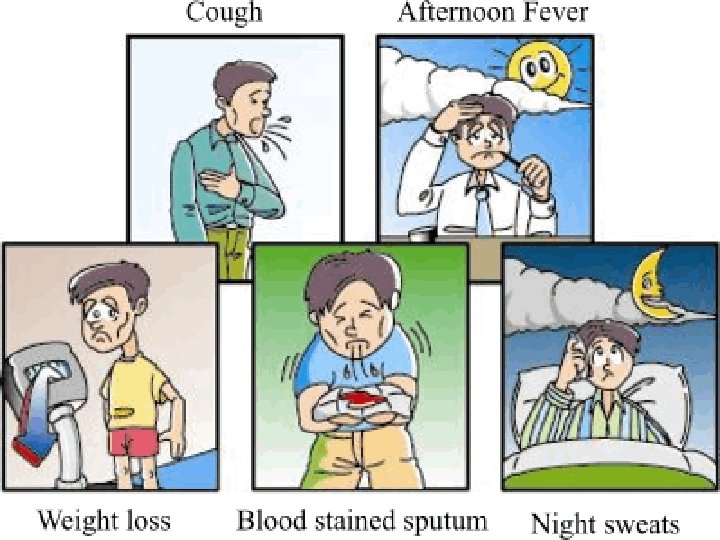
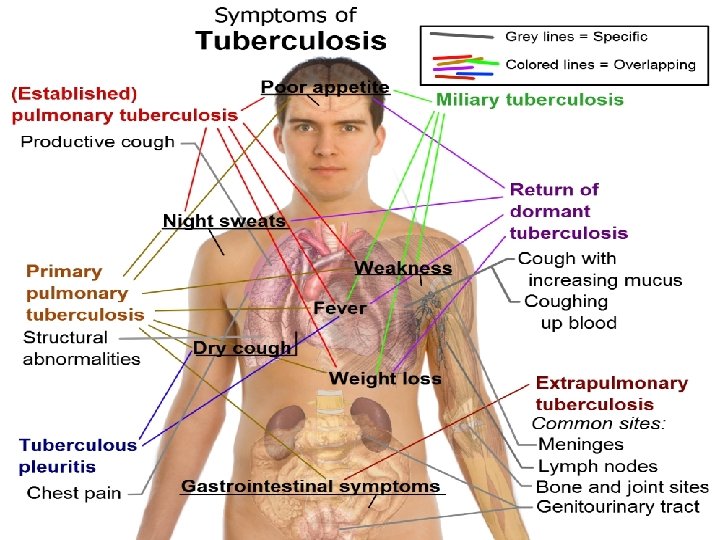

Physical findings…. õ Occasionally, rhonchi due to partial bronchial obstruction õ Systemic features include fever (often low-grade and intermittent) and wasting. õ In some cases, pallor and finger clubbing develop. õ Common hematologic findings are mild anemia and leukocytosis.

Diagnosis :

1. Tuberculin skin testing…

Induration Test results 0 -4 mm Not significant More than 5 mm Known or suspected HIV infection, IV drug users, people in close contact with a known TB case >10 mm Positive for clients in all other high risk groups. 15 mm and more Positive for clients in low risk groups.

2. Mycobacterial culture: Ø Isolation and identification of M. tuberculosis from a sputum specimen obtained from a patient with a productive cough. Ø 4 to 8 weeks may be required before growth is detected

3. AFB microscopy: Ø Microscopic examination of a diagnostic specimen such as a smear of expectorated sputum or of tissue Ø 3 sputum specimens, preferably collected early in the morning

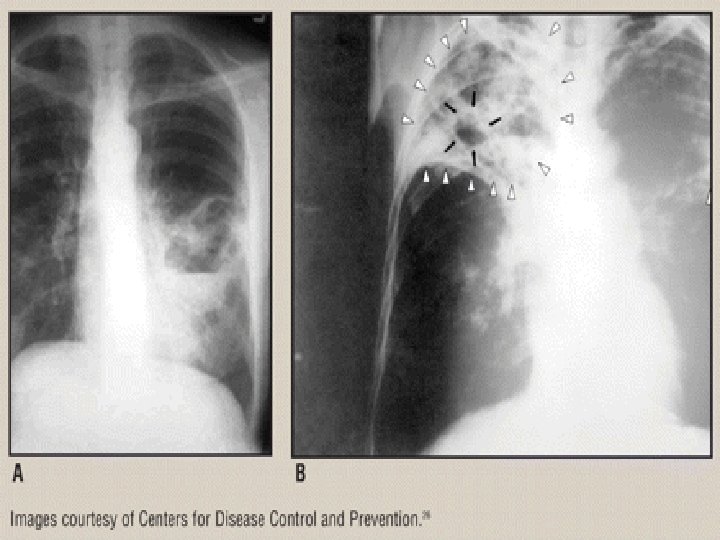
4. Radiographic studies: ü Classic picture is upper lobe disease with infiltrates and cavities

Classification of TB

CLS 0 1 2 Type Description -No Negative reaction to tuberculin skin test. exposure -Not infected -TB exposure Negative reaction to tuberculin test skin - No test. evidence of Infection -TB infection - No disease Positive reaction to tuberculin skin test. Negative bacteriologic studies (if done). No clinical or radiographic evidence of TB.
 or both")
CLS. Type Description 3 Current TB disease M. tuberculosis cultured (if done) or both a positive reaction to tuberculin skin test and clinical and/or radiographic evidence of current disease. 4 Previous TB disease 5 History of episode(s) of TB, abnormal stable radiographic findings in a person with a positive reaction to the tuberculin skin test, negative bacteriologic studies (if done) and no clinical or radiographic evidence of current disease. TB suspect Diagnosis pending

Medical management:

• The two aims of tuberculosis treatment are ü to interrupt tuberculosis transmission ü to prevent morbidity and mortality

Antituberculosis drugs:

An antitubercular drug should satisfy the following criteria: üHighly effective üFree from side effects üEasy to administer üReasonably cheap

ATT Bactericidal Rifampicin, Isoniazid, streptomycin and Pyrazinamide Bacteriostatic Ethambutol and thioacetazone

TREATMENT REGIMEN • Bacteriocidal agents: Drug Dose Rifampicin 10 -12 mg/ kg taken 1 hr. Before or 2 hr. After food 450 -600 mg Side effects • Gastritis • Thrombocyto penia • Nephrotoxicity
 4 – 5")
TREATMENT REGIMEN • Bacteriocidal agents: Drug Dose Side effects INH (ISONIAZID) 4 – 5 mg/kg (max. 300 mg) • Gastric Irritation • Neuropathy • Liver damage

TREATMENT REGIMEN Drug Dose streptomycin. 75 -1 gm in single injection Side effects • Vestibular damage • Nystagmus

TREATMENT REGIMEN Drug Dose Side effects Pyrazinamide 30 mg/kg • Liver divided into damage three doses • Hyperurice per day mia

Bacteriostatic drugs: They inhibit the multiplication of the bacilli and lead to their destruction by the immune mechanism of the host. It includes ü Ethambutol- dosage is 15 mg/kg body weight given in 2 to 3 doses ü Thioacetazone- usual dose is 2 mg/kg body weight

TREATMENT REGIMEN • Bacteriostatic agents: Drug Dose Ethambutol 15 mg/kg given in 3 doses Side effects Retrobulbar neuritis
 Dose 2 mg/kg Side effects")
TREATMENT REGIMEN Drug Thioacetazone (combination with INH is used) Dose 2 mg/kg Side effects ØNausea ØVomiting ØBlurring of vision ØUrticaria

Phases of anti-TB treatment:

The US centers for Disease Control and Prevention recommends a two-phase approach for treatment consisting of: Induction phase Continuation phase

Induction phase: It is a short aggressive or intense phase, early in the course of treatment, lasting 1 -3 months. During this phase, there is rapid killing of tubercle bacilli. Infectious patients become non-infectious within about two weeks. They mainly use 4 drugs.

Continuation phase: Usually use 2 drugs. The drugs eliminate the remaining tubercle bacilli. Killing the remaining bacilli prevents relapse after completion of treatment. the duration of treatment was not less than 18 months to achieve complete sterilization of the bacilli.

• Initial intensive phase with 4 drugs (INH, rifampicin and pyrazinamide, supplemented by either streptomycin or ethambutol) for a period of 2 months, Ø followed by 2 drugs in the continuation phase, (INH plus rifampicin or thioacetazone) given daily or intermittently
")
Directly observed treatment, short course chemotherapy (DOTS)

Dots is a strategy to ensure cure by providing the most effective medicine and confirming that it is taken. The strategy assures a compulsory and free availability of good quality drugs to all TB cases and It necessitates drug administration under direct supervision, thereby ensuring the requisite regimen-compliance.

How DOTS is carried out…? ? Intensive phase - a health worker or other trained person watches as the patient swallows the drug in his presence. Continuation phase - the patient is issued medicine for one week in a multiblister combipack

The drugs are provided in patient-wise boxes with sufficient shelf-life. In the programme alternate day treatment is used. The cases are divided into three types of categories- category I, category II and category III.

Prevention:

ü By far the best way to prevent tuberculosis is to diagnose infectious cases rapidly and administer appropriate treatment until cure. ü Additional strategies include : Ø BCG vaccination Ø Treatment of persons with latent tuberculosis infection

1. BCG vaccination:

õ BCG was derived from an attenuated strain of M. bovis, bacille Calmette Guerin, which was avirulent for man while retaining its capacity to induce an immune response. õ There are 2 types of BCG vaccine- the liquid (fresh) vaccine and the freeze dried vaccine. õ Freeze-dried vaccine is a more stable preparation than liquid vaccine. õ For vaccination, the usual strength is 0. 1 mg in 0. 1 ml volume intradermally. õ The dose to newborn aged below 4 weeks is 0. 05 ml.
:")
Multidrug resistant TB (MDR-TB):

Ø A case of TB caused by a strain of M. tuberculosis that is resistant to two or more antituberculosis drugs. Ø Some define MDR-TB as a case of TB caused by a strain of M. tuberculosis that is resistant to Isoniazid and rifampin. Ø XDR-TB (extensively resistant tuberculosis) refers to cases of TB that are resistant to Isoniazid, rifampin, the second line drugs, the fluoroquinolones, and at least one of three injectable drugs i. e. Amikacin. Ø It arise by spontaneous point mutations in the mycobacterial genome.

Drug-resistant tuberculosis may be either primary or acquired. ü Primary drug resistance is that in a strain infecting a patient who has not previously been treated. ü Acquired resistance develops during treatment with an inappropriate regimen. Reasons for secondary resistance are numerous and complex: Wrong drugs used in an improper way, failure to assess drug susceptibility patterns of the organism, large bacterial load especially in the case of cavitation, poor adherence to the treatment regimen

Treatment For strains resistant to Isoniazid and rifampin, combinations of a fluoroquinolone, ethambutol, pyrazinamide, and streptomycin given for 18 to 24 months and for at least 9 months after sputum culture conversion, may be effective. For patients with bacilli resistant to all of the first-line agents, cure may be attained with a combination of four second-line drugs, including one injectable agent. A duration of 24 months is recommended

Nursing management:

Nursing diagnoses: ♠Ineffective airway clearance related to copious tracheabronchial secretions ♠Imbalanced nutrition less than body requirement related to increased metabolic needs associated with infection ♠Activity intolerance related to fatigue, decreased intake of adequate nutrition and fever ♠Deficient knowledge about treatment regimen and preventive health measures ♠Ineffective health maintenance related to lack of understanding of resources

Patient education:




References… • Fauci, Braunwald, Kasper. Harrison’s principles of internal medicine. 17 th edition. New Jersey: Mc. Graw Hill • Kumar P. Clark. M. Kumar and Clark’s clinical medicine. 7 th edition. New Delhi: Saunders publication. • Black JM, Hawks JH. Medical-surgical nursing for positive outcomes. 8 th edition. Missouri: Elsevier publication. • Lewis, Heitkemper, Derksen. Medical surgical nursing: assessment and management of clinical problems. 6 th edition. Missouri: Mosby publication. • Manohan, Sands, Neighbors, Marek, Greek. Phipps medical surgical nursing: health and illness perspectives. 8 th edition. Missouri: Mosby publication.
- Slides: 85