Unit Eight Normal labor Labor is described as

Unit Eight Normal labor Labor is described as the process by which the fetus, placenta and membranes are expelled through the birth canal. Normal labor occurs at term and is Ph. D in MCH spontaneous in onset with the fetus presenting by the vertex. The process is completed within 18 hours and no complications arise. Dr. Areefa SM Albahri Ph. D in MCH

Initiation of labor: • The exact mechanism that initiates labor is unknown. Theories include the following: • Uterine stretch theory: uterus becomes stretched causes a release of prostaglandins. • Prostaglandin + oxytocin cause pressure on cervix stimulate more production of oxytocin). • There is increased production of prostaglandins by fetal membranes and uterine decidua as as pregnancy advances. • In later pregnancy, the fetus produces increased levels of cortisone which inhibit progesterone production from the placenta. • Placental aging and deterioration triggers the initiation of contractions.

General terms: • Lie: a comparison of the long axis of the fetus with the long axis of the mother. Fetal lie is either, longitudinal, transverse or oblique. In longitudinal lie either the fetal head presents or the buttocks present. In transverse lie, the shoulders present.

• Presentation: the part of the fetus deepest in the birth canal. Presentation may be vertex, face, brow, breech or shoulder.
.")
• Attitude: relationship of fetal parts to each other (normal flexion).

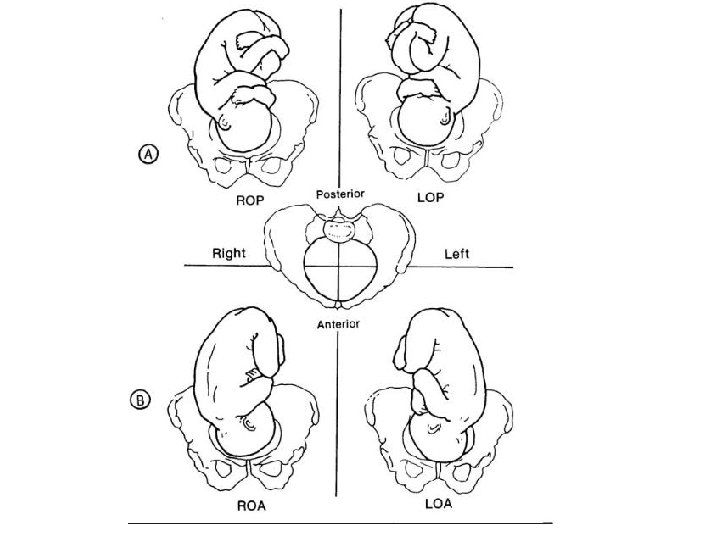
• • Position: Position refers to the location of a fixed reference point on the fetal presenting part in relation to a specific quadrant of the maternal pelvis. The presenting part can be right anterior, left anterior, right posterior, and left posterior. These four quadrants designate whether the presenting part is directed toward the front, back, right, or left of the passageway. It is the relationship of landmark on the fetal presenting part to the front (anterior = A) back (posterior = P) or side (transverse = T) of the mothers pelvis. Landmarks on the fetal presenting parts include head = occiput (O) buttocks = sacrum (S), shoulder = scapula or acromion (A), face = chin of mentum (M). • Example: a fetus presenting by the vertex with his occipit on the left anterior part of the woman’s pelvis would have his presentation and position described as LOA or lift occiput anterior.
 • Passageway (maternal pelvis) • Passenger (fetus")
Factors affecting labor: • Powers (physiological forces) • Passageway (maternal pelvis) • Passenger (fetus and placenta) • Passageway _ Passenger and their relationship (engagement, attitude, position) • Psychosocial influences (previous experiences, emotional status) • Successful labor and delivery depend on adequate pelvic dimensions, adequate fetal dimensions, presentation and adequate uterine contractions.

True and false labor contractions True labor contractions false labor contractions Result in progressive cervical Do not result in progressive dilation and effacement. cervical dilation and effacement. Occur at regular intervals. Occur at irregular intervals. Intervals-between Intervals remain the same or contractions decrease. increase. Intensity increases. Intensity decrease remains the same. or

Location mainly in back and Location mainly in groin and abdomen. Generally abdomen. intensified by Generally unaffected by walking. Not affected walking. by mild Generally relived by mild sedation. Dilation and effacement of There is no change in the cervix are progressive. cervix.

Pre-labor is the term given to the last few weeks of pregnancy A. Lightening, the setting of the fetus in the lower uterine segment occurs 2 -3 weeks before the onset of labor in the primigravida and later during labor in the multigravida. 1. The woman’s breathing becomes easier 2. Lordosis of the spine is increased, 3. Frequency of micturation
 Its presence often indicates that")
B. Vaginal secretions may increase. C. SHOW (bloody show) Its presence often indicates that labor will begin within 24 to 48 hours. D. Taking up of the cervix. it gradually merges into the lower uterine segment. The cervix becomes soft and effaced “thinned”. This softening and thinning is called cervical effacement E. False labor contractions may occur in last weeks of pregnancy. F. Membranes may rupture. G. As the pregnancy approaches term, most women become more aware o f Irregular contractions called Braxton-Hicks contractions. Note (regular U C+ CD+ bloody show ) this = onset of true labor women need admission

Stages of labor 1. The 1 st stage is that of dilation of the cervix. It begins with regular rhythmic contractions and is complete when the cervix is fully dilated 10 cm. 2. The 2 nd stage of labor is the expulsion of the fetus. It begins when the cervix is fully dilated and is completed when the baby is completely born. 3. The 3 rd stage of labor includes separation and expulsion of placenta and membranes. It lasts from the birth of the baby until the placenta and the membranes have been expelled. (about half an hour) 4. The 4 th stage lasts from delivery of the placenta until the postpartum condition of the woman has become stabilized “usually 1 -2 hour after delivery”

First stage consist of: 1. Latent phase: { cervical dilation is 0 -3 cm} Begins with the establishment of regular contractions (labor pains). Labor pains are often initially felt as sensations similar to painful menstrual cramping and are usually accompanied by low back pain. Contractions during this phase are typically about 5 minutes apart, last 30 to 45 seconds, and are considered to be mild. Usually, woman is excited about labor and talkative. It takes up to 10 -14 hours.

2. Active phase: cervical dilation is 4 -7 cm. The active phase of labor is characterized by more active contractions. The contractions become more frequent (every 3 to 5 minutes), last longer (60 seconds), and are of a moderate to strong intensity. While the length of the active phase is variable, nulliparous women generally progress at an average speed of 1 cm of dilation per hour and multiparas at 1. 5 cm of cervical dilation per hour.

3. Transitional phase: cervical dilation is 7 -10 cm The transition phase is the most intense phase of labor. Transition is characterized by frequent, strong contractions that occur every 2 to 3 minutes and last 60 to 90 seconds on average. Other sensations that a woman may feel during transition include rectal pressure, an increased urge to bear down, an increase in bloody show, and spontaneous rupture of the membranes (if they have not already ruptured).

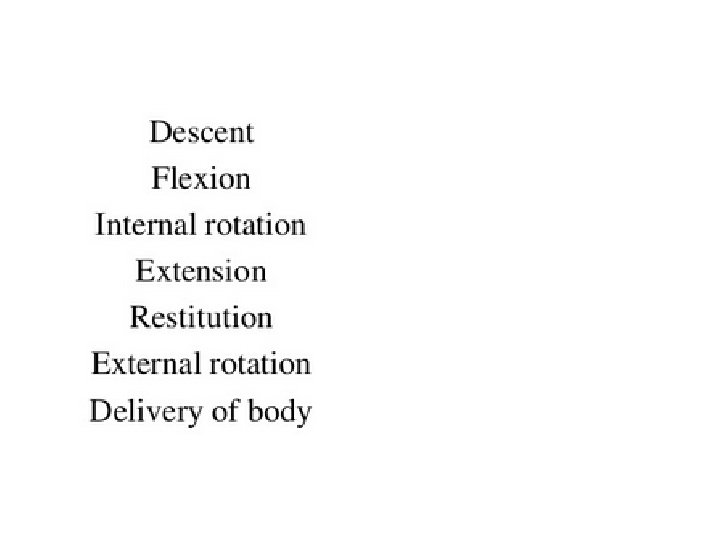
Mechanism of labor If the woman’s pelvis is adequate, size and position of the fetus are adequate and uterine contractions are regular and of adequate intensity, the fetus will move through the birth canal.


Nursing management during labor • • • Indications for vaginal exam • diagnosis of labor, dilation of the cervix Assessment: • identification of presentation. History taking and baseline data: {refer to your book} • To determine whether the head is engaged in case of doubt. Abdominal exam • Assess ruptured M or to rupture Vaginal exam them artificially. • To exclude cord prolapsed after rupture of membranes. • To assess progress or delay in labor. • To apply a fetal scalp electrode. When VE is contraindication?
 • Place fingertips gently on the funds.")
Assessing uterine contractions (Intensity, Frequency and Duration) • Place fingertips gently on the funds. • As contraction begins, tension will be felt under the fingertips. Uterus will become harder, then slowly soften. • The intensity may be described as follows: • Mild: the uterine muscle is somewhat tense. • Moderate: the uterine muscle is moderately firm. • Strong: the uterine muscle is so firm that it seems almost boardlike. • The frequency is measured in minutes, represents the time from the beginning of one contraction until the beginning of the next. • Duration of contraction is timed from the moment the uterus first begins to tighten until it relaxes again. • When the cervix becomes completely dilated, the contractions become very strong, last for 60 seconds and occur at 2 -3 minute intervals. •

Assessing fetal heart tones • Note location, rate and character. • Determine the position, presentation and lie of the fetus. • Place the fetal stethoscope on the abdomen over the back or chest of the fetus. • Listen and count the beat for one minute. • Check the rate before, during, and after a contraction to detect slowing or irregularities (110 -160 BPM normal) Differentiate between FHT and other abdominal sounds by: 1. FHT, very rapid, somewhat muffled ticking sound. 3. Maternal pulse (umbilical arteries) is synchronous with funic soufflé. ﺍﻟﺼﻮﺕ ﺍﻟﺴﺮﻯ ﺍﻭ ﺍﻟﺤﺒﻠﻰ Note: Check FHR immediately following rupture of the membranes. (why)

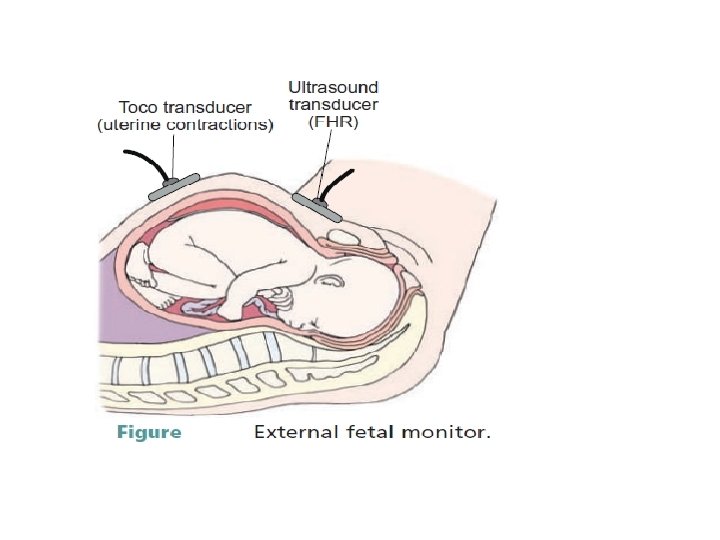
Fetal monitoring • • • The purposes of CFM during labor are: To monitor the progress of a women’s contraction pattern. To monitor the condition of the fetus in response to contractions. Women’s reaction to being monitored varies: Some women are reassured by hearing the continuous fetal heart sound. Some women experience discomfort because of the abdominal straps & their interference with movement as well as difficulty assuming a comfortable position. • • • External monitoring (indirect): Separate transducers are secured to the women’s abdomen. An ultrasound transducer translates fetal heart sound into electrical signals that are recorded on a strip chart. The ultrasound transducer device should be applied over the abdomen where the sharp fetal heart sound is heard. The measurement by external monitoring of the intensity of uterine contractions is not accurate.
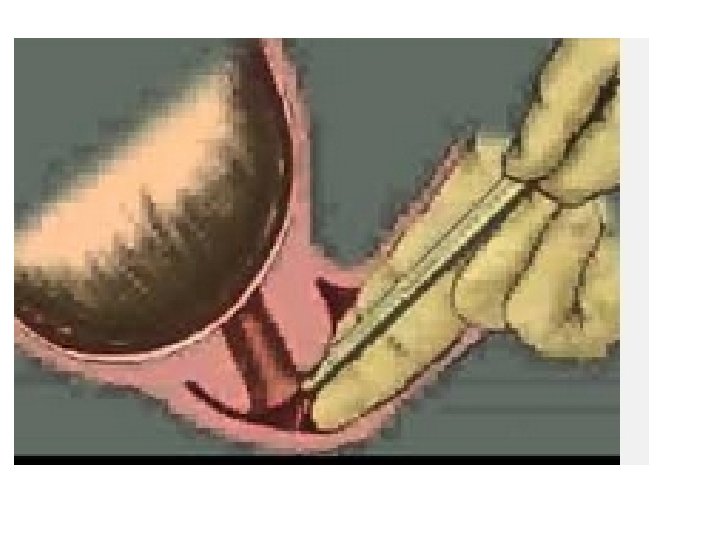
: A method of recording intrauterine pressure and")
• • • Internal monitoring (direct): A method of recording intrauterine pressure and FHR through internal measurement. More accurate than external monitoring. Note: The membranes must be ruptured. The cervix must be dilated 3 -4 cm. The station must be (-2) or lower. Uterine contractions are recorded by means of a catheter placed in uterine cavity behind the presenting part. • The catheter filled with distilled water and is connected to an external transducer that converts pressure to electronic signals. • Monitor strips record the quality of the uterine contractions and fetal heart patterns simultaneously. • • • Internal fetal monitoring is used for high-risk births or during a normal birth where the birth is having trouble keeping the baby on the monitor or the baby's reaction doesn't look great on the less accurate form of external fetal monitoring

• Interpretation: • FHR must be checked initially for rate in the absence of or in between contraction. • A change from the baseline is termed as fluctuation and is either acceleration or deceleration.

Documentation of CTG the documentation of the pattern should include: – woman’s name, date and time – estimated gestational age, – clinical indications for performing the FHR pattern, – maternal pulse rate. • The outcome of the FHR pattern should be documented both on the CTG and in the woman’s medical records at least every ½ hourly throughout labour. 27

FHR evaluation determine the risk Contractions baseline rate variability accelerations decelerations overall assessment (followed by a management plan) 28

Who should have continuous electronic FHR monitoring? • Antenatal risk factors – Prematurity – Pre-eclampsia/eclampsia – Diabetes – Growth restriction – Non-reassuring antenatal fetal welfare assessment – Multiple pregnancy – Malpresentation 29

Who should be have continuous electronic FHR monitoring? • Intrapartum risk factors – Syntocinon – Meconium – Epidural – Suspicious FHR on auscultation – Prolonged rupture of the membranes – Prematurity – Previous C/S 30

Practice Recommendations for intermittent auscultation • Healthy women with uncomplicated labour Pinards/Doppler recommended every 15 mins 1 st stage every 5 mins 2 nd stage • Continuous EFM is recommended if: § Baseline < 110 or >160 bpm; § Decelerations or intrapartum risk factors develop 31
 =")
Baseline rate • • • Normal = 110 – 160 bpm Bradycardia (moderate) = 100 – 109 bpm Bradycardia (abnormal) = < 100 bpm Tachycardia (moderate) = 161 – 180 bpm Tachycardia (abnormal) = >180 bpm (RCOG) 32

Variability • Greater than 5 bpm and less than 25 bpm • Increased variability is often seen following an acute hypoxic event. • Should settle after about 10 mins when the fetus returns to normal O 2 levels 33

• Acceleration or deceleration of the FHR are due to: • uterine pressure applied directly to the fetal head and / or umbilical cord. • Uterine pressure applied directly to the intervillous space ("space between the villi containing the vessels" of the mother and the embryo. . . ) which leads to decrease blood flow.

• An acceleration is defined as an increase in the FHR of 15 bpm above the fetal heart baseline that lasts for at least 15 to 30 seconds. • Accelerations are considered a sign of fetal well-being when they accompany fetal movement. • Thus, when a fetus is active in utero, accelerations are normally present. • accelerations are often noted as a response to the contraction. • Limited acceleration during sleeping fetus.

Deceleration : Early Deceleration. Begins near the onset of contraction Lowest level of FHR occurs at the peak of the intrauterine pressure (contraction). • FHR does not fall below 100 BPM. • Not usually cause change in acid-base balance. • Caused by v fetal head pressure (which cause vagal stimulation which decrease in HR) v May occur during vaginal examinations v uterine contractions, and during placement of the internal mode of Early decelerations. fetal monitoring. Bottom. Uterine contractions. • Need no intervention. • •

• Late deceleration: Begins later in contracting phase of uterus (as the contraction reaches its peak) and resolved when the contraction ends. • Usually less than 90 seconds in duration. • Passage of meconium may occur. • Associated with progressive fetal hypoxia and acidosis. • Due to acute uteroplacental insufficiency as a result of a decreased blood flow from the uterus to the placenta results in fetal hypoxia and late decelerations). v Should be reported immediately. Late decelerations.
 Careful maintenance of maternal pressure")
• Late deceleration can be avoided by: a) Careful maintenance of maternal pressure within normal limits b) Careful infusion of oxytocins and anesthetics. Late deceleration can be modified by : a) Discontinue oxytocin if being given. b) Chang the woman's position to the left side c) Administer oxygen and IV fluid d) Obtain fetal blood sample to measure degree of hypoxia and acidosis e) If persist, labor may be terminated by Cesarean or Forceps delivery

• Variable deceleration • Decelerations are variable in terms of their onset, frequency, duration, and intensity. • Due to umbilical cord compression • Non uniform and has no relation to contractions • In severe deceleration, FHR may fall by 70 BPM and last longer than 60 seconds. • Usually relieved by changing position of the woman to relieve pressure on the cord When sever cord prolapse should be suspected

• Tachycardia is generally defined as a sustained baseline fetal heart rate greater than 160 beats per minute for a duration of 10 minutes or longer. • A number of conditions are associated with fetal tachycardia: ü Fetal hypoxia ü Maternal fever ü Maternal medications ü Infection ü Fetal anemia ü Maternal hyperthyroidism • Bradycardia is defined as a baseline FHR of less than 110 to 120 bpm. Fetal bradycardia may be associated with: • Late hypoxia • Medications: (e. g. , propanolol) • Maternal hypotension • Prolonged umbilical cord compression


The stages of labor 1 st stage of labor • First stage divided into 3 phases • Latent phase (0 -3 cm). contractions (usually 5 -30 minutes apart, lasting 20 -40 second), fetal heart sounds every 1 -2 hours, temperature every 4 hours unless elevated. • Provide clear liquids if permitted • Allow the woman to walk. • Evaluate and teach breathing techniques helpful in coping with active and transitional phase of the 1 st stage and breathing • Provide support for the woman's care such as providing back massage and timing of contractions. • Provide privacy for in the periods of giving care. • Encourage the woman to void approximately every 2 hours to keep bladder empty
 • Contractions are usually 2 -5 minutes apart, lasting")
Active phase (4 -7 cm) • Contractions are usually 2 -5 minutes apart, lasting 30 -50 seconds • Monitor progress of labor, take and record vital signs, Contractions and fetal heart sounds every 30 minutes • Be aware that the woman may begin to feel unable to cope with discomfort and may begin to lose control • breathing and relaxation techniques with each contraction • Provide comfort measures: • Side-lying position is usually more comfortable • Provide sacral hand pressure and backrest • Change wet or soiled linen • Assist with mouth care • Continue to provide encouragement and information • Administer prescribed analgesia as prescribed • Maintain hydration and glucose level of woman. Low glucose level decrease intensity of contractions (I. V) fluid may be necessary
. • Contractions are usually 2 -3 minutes apart, lasting")
Transitional phase (7 -10 cm). • Contractions are usually 2 -3 minutes apart, lasting 50 -90 seconds • Generally it is the most difficult phase of the 1 st stage • Bloody show increases • Nausea and vomiting may occur because of reflex action as the cervix stretches and begins to retract over the fetal head • Woman may be restless and cry during feelings

Nursing Interventions in the first stage: • Monitor progress of labor, vital signs, contractions and fetal heart sounds every 15 minutes • Assist with controlled breathing as contractions occur • Discourage the woman from bearing down until cervical dilatation is complete • Encourage the women to rest between contractions to conserve energy • Provide concise and brief explanations because woman is irritable • Remind the woman that labor is nearing its end • Prepare the woman for movement to the delivery room

2 nd and 3 rd stage of labor • Characteristics: • Full cervical dilation occurs, infant is delivered • Usually primigravida has an average of 20 contraction and multigravida an average of 10 contraction

Nursing Interventions • Monitor FHR, contractions and blood pressure every 5 minutes • Encourage pushing, only with contractions using abdominal muscles • If the partner or support person is present, have him to support woman and see birth if desired • Cleanse vulva and perineal area • Check equipment needed for infant resuscitation • Keep the woman informed of progress of delivery • The woman may need to be catheterized, if bladder is full • When the vulvovaginal ring encircles the head, an episiotomy may be performed to prevent tearing of the perineum

Episiotomy is a surgical incision of the perineum that is performed to enlarge the vaginal orifice during the second stage of labor. Continue Nursing Intervention • When the baby is delivered, the infant is put in mother abdomen • Placenta usually separates and delivered within 15 -20 minutes following delivery of the baby. • Vaginal canal and cervix are inspected for lacerations or injury, • The woman’s perineal area is cleansed and a sterile perineal pad applied. • As the placenta separates from the uterine wall, it is important that the uterus continues to contract. attachment site. Failure of the uterus to contract adequately with separation of the placenta can result in excessive blood loss or hemorrhage. • To enhance the uterine contractions after expulsion of the placenta, oxytocin is often given (IV or IM). • Once the placenta has been delivered, the nurse carefully examines it to ensure that all cotyledons are intact. • If any part of the placenta is missing, the nurse immediately reports this finding to the attending physician.

• 4 th stage of labor • Considered to be the stage of recovery period but in the same time it is a critical period for the mother and the newborn • It is the first two hours post-birth, the mother starts readjustment to the non-pregnant state and body systems begin to stabilize • The primary danger for the mother is hemorrhage • The safety of the mother depends on frequent assessment and timely interventions of alert nurses • During is the first hour for physical assessment, all factors except temperature assessed every 15 minutes then every 30 minutes during the second hour

• Factors to be assessed: • Vital Sign • Fundus: firm and 2 cm below or at level of umbilicus, but if it was soft, message is done until firm • Bladder • Emotional status • Lochia: if blood comes in spurts, cervical tear is suspected • Perineum: assess sutures of episiotomy • Discomfort (after pain): as a result of uterine contraction

Potential for hemorrhage related to uterine atony and trauma • The fundus remains firm with gentle massage • Massaging expels blood and clots (uterus contract) • If uterus doesn't respond and bleeding continues, I. V Pitocin is administered • Lochia is bright red (scant, moderate, heavy) • Assess the amount of bleeding by checking the perineal pads and under buttocks Note : Saturated pad (tail to tail) =100 ml blood Loss of 100 ml blood/15 min is considered heavy Vital signs every 15 minutes Notify the physician

• For Episiotomy and Hemorrhoids: • Encourage side lying position • Apply ice packs for 2 hours • Administer analgesics as prescribed • Encourage self- relaxation techniques
 • • Is the")
Complications of labor and birth Premature Rupture of Membranes (PROM) • • Is the spontaneous rupture of fetal membranes one hour or more before the onset of labor. • Incidence: 10% of all pregnancies. • Causes: remains unknown in most cases. Risk factors: Polyhydaminos Cerculage Amniocentesis Placental abruption. Infection More common in twins gestation. • Seldom associated with trauma • • Complications: • Preterm delivery. • Maternal or fetal infections: – Chorioamniositis – endometrits clinically persisting after delivery. • Fetal distress – Umbilical prolapsed more common in cases of PROM. • Increase rate of stillbirths

Evaluating the patient with PROM Sterile speculum examination: -Visualize pool of fluid in vaginal fornix -Leakage of fluid through cervix. • p. H of amniotic fluid is 7. 1 to 7. 3 • Normal vaginal p. H is 4. 5 to 6 • • Nitrazine paper turns blue at p. H > 6. 5 Cervical dilation is assessed. Observe for prolapsed fetal part or umbilical cord. Collection of fluid for lung maturity Ultrasound is a final confirmatory step in some cases. Establish gestational age and fetal maturity Rule out infection& fetal distress. continuous fetal heart tone monitoring. Management and interventions: • Term patients: • Immediate induction is suggested. • Preterm patients: • Survival rate after 26 weeks is close to 50%. • If less than 34 weeks, efforts are directed toward maintaining pregnancy. • • • Tocolytic therapy (terbutaline) Antibiotics therapy Nurse monitors vital signs emotional support are provided prepares the mother for delivery, cesarean birth, a preterm neonate and potential loss of the fetus.

• Preterm labor • Is defined as rhythmic uterine contractions that produce cervical changes prior to completion of 37 weeks gestation. • Incidence: • 7% to 10% of infants are born prematurely. • Responsible for 75% of prenatal mortality and about 50% of neurological deficits. Etiology: Upper and lower extremes of age. Lower socioeconomical status. Smoking and drug abuse. Prolonged periods of standing. Fatigue and long hours at work. Reproductive history: Previous preterm delivery. Incompetent cervix. Spontaneous or induced abortion. Uterine anomalies e. g. leiomyomata. • - Multiple gestations. • - Premature rupture of membranes (most common cause). • Infection. • • •

• Assessment: • Cervical dilation. • Membranes: ruptured or not. • Presences of sever preeclampsia and hemorrhage. • Ultrasonography: to determine fetal gestational age, condition and weight. • Management and intervention: • Special prenatal care for high risk women. • Frequent visits for weeks 22 to 32. • Urine culture at 24 weeks. • Vaginal examination for p. H. • Education on nutrition and preterm labor. Observe Signs and symptom reinforced such as : 1. Increased or change in vaginal discharge. 2. Uterine contractions. 3. Vaginal bleeding or leaking fluid. • Provide Bed rest and hydration: • Continuous monitoring. • Tocolytics:

Cont, management • - Now most frequently used agents are magnesium sulfate and beta mimetic agents → acts on β 2 receptors on myometrium. • - Maternal transport: tocolytic therapy may improve outcomes by delaying delivery enough to facilitate transport. • Note : labor is not stopped if one or more of the following are present "exclusion criteria for tocolytic therapy": • 1. Advanced cervical dilation, usually > 6 cm. • 2. PROM. • 3. Abruption. • 4. Fetal distresses or death. • 5. Major fetal anomalies incompatible with life. • 6. PIH with HELLP syndrome. Fetal maturation therapy: glucocorticord therapy.

Nursing care: • • • - Placed on bed rest, lying on her side. - Uterine contractions are evaluated and monitored every 1 -2 hr. - Continuous monitoring of FHR. - Cervical consistency, dilation and effacement are evaluated. - Symptoms are evaluated for progress “increasing or decreasing". - I. V fluids started, intake and output are monitored. Once contraction have been stopped and women's condition has stabilized, she may be discharged and the following done to prevent subsequent occurrence: - Bed rest maintained. & vitamins supplement, especially vitamin C. - Usual activity level is evaluated and restricted if necessary. - Chronic illnesses are monitored closely, acute illnesses are treated promptly. - Oral medications may be continued at home. - Prenatal visits are made weekly for remainder pregnancy
 • Duration of pregnancy: 280 days or")
Postdate (post term pregnancy or prolonged pregnancy) • Duration of pregnancy: 280 days or 40 weeks from the first day of the LMP or 266 days from ovulation, based on 28 day cycle. • Post term: pregnancy lasting more than 2 weeks beyond the expected date of delivery “after day 294, 42 completed weeks or more" • Etiology: • most frequent cause is inaccurate dating of pregnancy. • The exact cause of postterm pregnancy is unknown. However, a possible cause may be related to a deficiency of placental estrogen and the continued secretion of progesterone. • Low levels of estrogen may result in a decrease in prostaglandin & reduced formation of myometrial oxytocin receptors.

• • Rare causes: - Fetal anencephaly, adrenal hypoplasia. - Lake of cervical prostaglandin production. Maternal problems: 1. Emotional stress. 2. Potential for delivery trauma. 3. Hemorrhage, infection, and labor abnormalities.

Infant problems : much more serious than those for this mother. 1. Oligohydramnios associated with cord compression, acute fetal hypoxia and SID. 2. Macrosomia birth trauma, obstructive labor, shoulder dystocia. 3. Meconium aspiration due to thick meconium as a result of oligohydramnios. • 4. Intraprtum fetal distress. • 5. Dysmaturity: at 37 weeks, there is no further growth of the placenta. It ages rapidly past the fortieth week of gestation; it becomes inefficient and cannot adequately support the fetus • 6. Neonatal problems may include asphyxia, meconium aspiration syndrome, hypoglycemia, polycythemia, respiratory distress, and dysmaturity syndrome.

Management: • Weekly vaginal examination, plan induction when cervix is favorable. • Antepartum fetal heart monitoring, non stress test, ultrasound scans. • Induction of labor, prostaglandins or oxytocin, forceps- or vacuum-assisted birth and cesarean birth • Fetal distress emergency cesarean section sometimes required.
 • Hypotonic labor is defined as less than 3 contractions")
Hypotonic uterine contraction (inertia) • Hypotonic labor is defined as less than 3 contractions of mild to moderate intensity occurring in a 10 minutes period during the active phase of labor. • The intrauterine pressure (IUP) is insufficient for the progression of cervical effacement and dilation. • Cervical dilation and descent of fetus slow greatly or stop.

• Etiology: • Such labor occurs when uterine fibers are overstretched from large baby, twins, hydramnios, or multiparity. • May also be caused by administration of sedations or narcotics. • Bowel or bladder distention.

Potential maternal effects: - Exhaustion. Postpartum hemorrhage. - Stress and psychological trauma. Infection. • Potential fetal effects: • - Fetal sepsis (Infection). • - Fetal and neonatal death. • •

• Medical management: • Walking and position changes in labor assist in fetal descent through the maternal pelvis and therefore need to be encouraged. • The use of relaxation techniques & massage can decrease the need for pharmacological agents for pain. • Oxytocic stimulation of labor or prostaglandin stimulation.

• Nursing intervention: • Pelvis is reevaluated for size. • IV fluids are provided to maintain hydration and electrolyte balance. • Oxytocin administration is started if pelvic size is adequate, fetal position and presentation is normal. • Monitor FHR and contractions, if contractions last more than 60 -70 seconds, decrease or stop infusion to prevent rupture of uterus and premature separation of the placenta and fetal hypoxia. • Observe IV drip, be certain that infusion is running at the prescribed rate. • Report any maternal or fetal distress immediately. • Amniotomy may be performed to augment labor. • Use anxiety-reducing measures to promote psychological and emotional status.

Hypertonic uterine contraction • usually occurs in the latent phase of labor, with an increase in frequency of contractions and a decrease in their intensity. • Contractions are strong and often painful but are ineffective in producing cervical effacement and dilation. • An increase in maternal catecholamine release (i. e. , epinephrine, norepinephrine) can result in poor uterine contractility. • Contraction may be uncoordinated and involve only portions of the uterus. • Usually occurs before 4 cm dilation. The cause is not yet known, may be related to fear or tension.

• Potential maternal causes: • Maternal anxiety (Primiparous labor, Loss of control, Sexual abuse, Lack of support, Cultural differences, Fear of pain) • Potential fetal causes: • occiput–posterior malposition
 if membranes are not ruptured and")
• Medical management: • Analgesic (morphine, meperdine) if membranes are not ruptured and fetalopelvic disproportion isn't present. • Natural labor with effective contractions often resumes after this simple intervention. • Nonpharmacological techniques to reduce anxiety such as relaxation techniques, massage, a warm shower or tub bath, and increased emotional support are also helpful for some women. • For a woman whose fetus is in an occiput–posterior position, the major goal of care is to facilitate rotation of the fetal head into a more favorable position (walk and change positions frequently).

• Nursing intervention: • Provide bed rest with end of sedatives to promote relaxation and reduce pain. • Provide fluids to maintain hydration and electrolyte balance. • Observe for normal contractions when woman awakens. • Oxytocin is not administered; it will increase the abnormal labor pattern. • Check intake and output every 2 hr. • Monitor vital signs and FHR. • If the condition is prolonged, check for CPD and malpresentation, if excluded, amniotomy and oxytocin infusion may be instituted. • Reduce anxiety; give psychological and emotional support measures.

• Uterine rupture is a spontaneous or traumatic rupture of the uterus. • Causes: • Rupture of the scar from a previous cesarean delivery or hystrotomy. • Uterine trauma • Congenital uterine anomaly. • Prolonged or obstructed labor. • Forced delivery of fetus with abnormalities e. g. hydrocephalus. • Internal or external version. • Application of forceps and extraction before cervical os has completely dilated. • Injurious use of oxytocin. • Excessive manual pressure applied to the fundus during delivery.

• • • • Clinical manifestation: 1. Complete rupture: - Sudden sharp abdominal pain during contractions. - Abdominal tenderness. – Cessation of contractions. - Bleeding into abdominal cavity and sometimes into vagina. - Fetus easily palpated, fetal heart tones cease. - Signs of shock. 2. Incomplete rupture: - Develops over a period of few hours. - Abdominal pain during contractions. - Contractions continue, but cervix fails to dilate. - Vaginal bleeding may be present. - Tachycardia, pale skin. - Loss of heart tones.

Management and nursing intervention: ü Emergency laparotomy is performed with complete rupture, usually the uterus is removed and attempts are made to save the baby. ü Administer IV fluids and blood as directed. ü Administer oxygen to the woman. ü Prepare the woman for emergency surgery. ü Monitor maternal & fetal vital signs until surgery begins. ü Uterus may be repaired if rupture is not extensive, if extensive hysterectomy is necessary.

Amniotic fluid embolism. • Is the accidental infusion of amniotic fluid in to the mother's blood stream under pressure from the contracting uterus. • Amniotic fluid containing fetal vernix, lanugo, meconium, and mucus enters maternal blood through defect's in to the placental attachment, these particles become emboli in the mother’s general circulation causing acute respiratory, circulatory collapse, hemorrhage and corpulmonale as they block the vessels of her lungs. • These particles stimulate abnormal coagulating, initiating DIC. • Amniotic fluid embolism is rare and usually fatal (mortality rate is as high as 80% for mothers & approximately 50% of neonates)

Clinical manifestations: Ø Sudden dyspnea and chest pain. Ø cyanosis. Ø tachycardia. Ø - Pulmonary edema. Ø Prolonged shock due to: • 1. Anaphylaxis, which cause vascular collapse. • 2. Uterine bleeding with development of hypofibrinogenemia.
.")
Management and nursing intervention: • Emergency measures are instituted immediately including, cardiopulmonary resuscitation (CPR). • 1. Improving tissue perfusion and cardiopulmonary function. • 2. Administer O 2 as soon as possible, when situation is recognized. • 3. Provide assisted ventilation. • 4. Maintaining fluid volume and correction of DIC. • 5. Administer fresh whole blood and fibrinogen. • 6. Administer IV fluids and plasma. • 7. Provide continuous monitoring of maternal and fetal status. • 8. Delivery of fetus. • 9. Since fetus is in great danger, cesarean approach is used. • 10. Care for the neonate and provide family members with comfort and information about the status of mother and infant.

• Prolapsed Umbilical Cord • Umbilical cord prolapse occurs when a loop of the umbilical cord slips down below the presenting part of the fetus.
, occurs at any time during")
• Types • Occult prolapse (hidden; not visible), occurs at any time during labor whether or not the membranes have ruptured— the cord lies beside the presenting part in the pelvic inlet. • Complete prolapse, the cord descends into the vagina, where it is felt as a pulsating mass on vaginal examination. It may or may not be seen. • Frank (visible) prolapse most commonly occurs immediately after rupture of membranes as gravity washes the cord in front of the presenting part.

• Causes: – Rupture of membranes, when the presenting part is not engaged in the pelvis. – More common in shoulder & foot presentation. – Prematurely: As small fetus allows more space around presenting part. – Hydramnios: greater amount of fluid to be related with greater force when membranes rupture. – Contracted pelvis. – Placenta previa.

• Clinical Manifestation: • Cord may be seen protruding from vagina, or can be palpated in the vaginal canal cervix. • Signs of fetal distress: the cord is compressed between the presenting part and bony pelvis. • If cord is exposed to cold room air, there may be reflex constriction of umbilical vessels, restricting oxygen flow to fetus. • Fetal heart rate pattern may be irregular with periodic fetal bradycardia.

Management • Maintaining oxygen supply to fetus: • -all women whose membranes have ruptured should remain on bed rest. • -At the time of spontaneous rupture or amniotomy, FHR is assessed continuously, if bradycardia is noticed, assess for cord prolapse. • -Place the women in recovery or knee-chest position. • -Administer oxygen to the women. • -Place sterile gloved hand in vagina and push the fetal head up ward to relief compression of the cord. • -Prepare of immediate vaginal delivery if cervix is dilated. • -Prepare of immediate cesarean delivery if cervix is not deleted. • -In home situation, cover-protruding cord with clean wet dressing. Elevate the woman's hips and transports to hospital immediately.

 is a rare but")
Uterine Inversion • Uterine inversion (uterus is turned inside out) is a rare but potentially life-threatening complication. • Possible causes: • Most common cause is excessive pulling on the umbilical cord in an attempt to hasten the third stage of delivery. • Other contributing factors include vigorous fundal pressure, uterine atony, and abnormally adherent placental tissue. • Clinical Manifestations: • When complete inversion occurs, a large, red, globular mass (that may contain the still-attached placenta) protrudes 20 to 30 cm outside the vaginal introitus. • A partial or incomplete inversion is not visible; instead, a smooth mass is palpated through the dilated cervix. • Maternal symptoms include pain, hemorrhage, and shock.
 by")
• Management • Involves manual replacement of the fundus (under general anesthesia) by the physician, followed by oxytocin to facilitate uterine contractions and antibiotic therapy to prevent infection. • Prevention (by not pulling strongly on the cord until the placenta has fully separated) is the safest and most effective therapy.

Induction of Labor • Is the initiation of uterine contractions before their spontaneous onset. • Is the use of physical or chemical stimulants to initiate or intensify uterine contractions. • The need for initiating labor may arise from maternal or fetal sources. E. g. PIH, post-term pregnancy, D. M, PROM, I. U. F. D (intra Uterine Fetal death). • Elective induction may be indicated for the woman who has a history of precipitate labor to avoid unexpected out of hospital birth. • There a number of medically approved methods to induce labor; they include chemical induction with prostaglandins, oxytocin and mechanical as rupture of membranes.

• Prostaglandins • A prostaglandin gel for local application to the cervix has been formulated to soften the cervix and induce labor. • For those women whose cervix is unfavorable, induction using PGE is more effective than using oxytocin. • routine assessment for, dilation of cervix is required. • A 30 minutes electronic monitoring of FHR and uterine contractions is done to establish base line data. • The physician instills 0. 5 mg of PGE intracervically using a plastic catheter. The catheter is then removed.

• The woman remains in bed for 30 minutes, then may ambulate. • FHR, BP and pulse are monitored at least every 30 minutes. • Contractions usually begins 1/2 hour after administration of gel, the time of contraction is recorded. • An amniotomy is performed at 4 cm of cervical dilation and internal fetal monitoring is applied. • Progress of labor is recorded. • Any hypertonic contractions of the uterus are reported immediately. • If the woman doesn`t deliver within 24 hours, the cervix is reassessed an induction using oxytocin is done if indicated. • Because prostaglandin administration is effective, free of side effects and non invasive, some authorities believe it will replace amniotomy and oxytocin as the method of choice for induction of labor. • The woman is kept informed of the progress of labor.

• Oxytocin • May be used either to induce the labor process or to augment a labor that is progressing slowly because of inadequate uterine contraction, or to assess fetal response to the stress of contractions. • Indications: • Prolonged pregnancy. • Preterm delivery in diabetic mother. • Severe Preeclampsia, Abruptio placenta or I. U. F. D. • Multigravida with a history of precipitate labor. • Prolonged rupture of membrane. • Management of abortions.

• • • Contraindications: Fetopelvic disproportion. Fetal distress. Previous uterine surgery. Over distended uterus e. g. multiple pregnancy.

Hazards: – Maternal: titanic contractions, Abruptio placenta, Postpartum hemorrhage, infection, DIC, Amniotic fluid embolism, anxiety and fear. – Fetal: Asphyxia, Hypoxia, physical injury and Prematurity. – 10 IU of oxytocin is added to 1 L of 5% dextrose or saline solution. – Initial dose 2 milliunits/minute via constant infusion pump. – Dose is increased every 15 -20 minutes until dose is 20 milliunits per minute. – Monitor the woman's BP, P, respiratory rate, contractions and FHR every 15 minutes. – If FHR indicate distress or if contractions last 70 seconds or more, reduce or discontinue administration immediately. – Increase IV solution without oxytocin, give O 2, turn on her left side and call the physician. – Satisfactory labor has usually been initiated when the woman has 3 contractions in 10 minutes. – Reduce anxiety.

• Amniotomy • Transcervical amniotomy or artificial rupture of membranes can be used to stimulate labor. • Simple rupture of the membranes using sharp instrument passes over a finger into the cervix will allow the discharge of amniotic fluid. • Procedure is explained to the woman, FHR recorded. • Note and record amount and quality of fluid (clear, color, bloody, meconium…). • Artificial rupture of the membranes is often done to augment labor already in progress, since the membranes serve as a barrier against infection. • Delivery is usually accomplished soon after the membranes have been ruptured artificially. • Some obstetricians prefer to first stimulate the uterus with IV oxytocin and as soon as good contractions are evident, rupture the membranes. Others prefer merely to rupture the membranes. • Reduce anxiety.
- Slides: 94