Understanding Trauma Practicing With a Trauma Focused Lens











 Good health; history of adequate development")






 Collaboration between Kaiser Permanente’s Department of Preventative Medicine")








 12 10 Abused Alcohol or Drugs 8")







 25")









 “Trauma-Informed Care is a strengths-based framework that is grounded in")












- Slides: 61
Understanding Trauma: Practicing With a Trauma Focused Lens Whitnei A. Pryor, PMP Director of Training
Training Objectives Understanding Trauma Impact of Trauma on the Developing Brain Research and Implications for Trauma. Informed Practice
What is Trauma…Really? Children and adolescents experience trauma under two different sets of circumstances. � ACUTE � COMPLEX
Acute Trauma single traumatic event that is unpredictable and overwhelms a child’s ability to cope. Common examples of acute events that may be traumatic for the young child are: � Natural disasters such as hurricanes, fire, floods � Serious accidents � Bodily injury � Illness, especially when accompanied by a very high fever � Hospitalization, surgery, or painful medical procedures � Forced separation from the parent/caregiver
Complex Trauma Multiple or prolonged exposure Repeated Physical & sexual abuse Domestic violence Wars and other forms of political violence
What is Child Traumatic Stress? Exposure to traumatic events or situations that prevent a child from coping with the experience
Traumatic Events War, battles, combat Natural disasters Catastrophe, accident Violent attack Abuse
Sanctuary Trauma The traumatic events that occur in mental health and other human service settings. Consumers report retraumatization in both institutional and community service settings. Psychiatric inpatient settings, where coercive practices replicate the dynamics of their original trauma “Primum non nocere”
Reactions to Traumatic Stress Children respond to traumatic stress in different ways. � Signs of intense distress: disturbed sleep, difficulty paying attention, anger and irritability, etc. � Psychiatric conditions such as PTSD, depression, anxiety, and a variety of behavioral disorders. Post Traumatic Stress Disorder (PTSD) � Characterized by three clusters of symptoms Intrusive Symptoms Avoidant Symptoms
“The world breaks everyone and afterwards many are strong at the broken places. ” - Ernest Hemingway
Resilience: “Bouncing Back” The ability to show positive adaptation in spite of significant life adversities and challenging life experiences Even though distressed, individuals can manage negative situations, face disappointments, and engage positively despite their situations Turns victims into survivors and allows survivors to thrive
Protective Factors (US Gov. Health and Human Services) Good health; history of adequate development Above average intelligence Hobbies and interests Positive peer relationships Easy temperament, active coping style, positive self esteem Access to health care and social services Parents model good coping skills Household rules & structure Extended family / caregiver support
Still Face Experiment http: //www. youtube. com/watch? v=Btg 9 Pi. T 0 s. Zg
Impact of Trauma on the Brain
Fight or Flight Brain During Stress Frontal executive functioning areas are disengaged Subcortical fight or flight areas are engaged This response can lead to impulsive, even violent behavior; increased anxiety, depression, substance abuse, learning disorders, & increased
Early Childhood Brain Development In early childhood, trauma can be associated with reduced size of the cortex. � The cortex is responsible for many complex functions, including memory, attention, perceptual awareness, thinking, language, and consciousness. Trauma may affect “cross-talk” between the brain’s hemispheres, including parts of the brain governing emotions. � These changes may affect IQ, the ability to regulate emotions, and can lead to increased fearfulness and a reduced sense of safety
School Age Children Brain Development In school-age children, trauma undermines the development of brain regions that would normally help children: � Manage fears, anxieties, and aggression � Sustain attention for learning and problem solving � Control impulses and manage physical responses to danger As a result, children may exhibit: � Sleep disturbances � New difficulties with learning � Difficulties in controlling startle reactions � Behavior that shifts between overly fearful and overly aggressive
Adolescent Brain Development In adolescents, trauma can interfere with development of the prefrontal cortex, the region responsible for: � � � Consideration of the consequences of behavior Realistic appraisal of danger and safety Ability to govern behavior and meet longer-term goals As a result, adolescents who have experienced trauma are at increased risk for: � � Reckless and risk-taking behavior Underachievement and school failure Poor choices Aggressive or delinquent activity
The Adverse Childhood Experiences Study (ACE) Collaboration between Kaiser Permanente’s Department of Preventative Medicine in San Diego and the Center for Disease Control and Prevention
What is the ACE Study? Decade long - 17, 000 people involved. Looked at effects of adverse childhood experiences over the lifespan. Largest study ever done on this subject.
Adverse Childhood Experience Categories Abuse of Child Recurrent Severe Emotional abuse Recurrent Physical abuse Contact Sexual abuse Trauma in Child’s Household Substance abuse Parental separation or divorce Mentally ill or suicidal household Mother treated violently Imprisoned household member Loss of parent Neglect of Child Abandonment Physical/emotional needs unmet
ACE Study Findings Of the 17, 000 HMO Members: 1 in 4 exposed to 2 categories of ACEs 1 in 16 was exposed to 4 categories. 22% were sexually abused as children. 66% of the women experienced abuse, violence or family strife in childhood.
ACEs are Common CHILDHOOD ABUSE Psychological Abuse Physical Abuse Sexual Abuse TRAUMA IN HOUSEHOLD Substance Abuse Parental Separation/Divorce Mental Illness Battered Mother Criminal Behavior NEGLECT Emotional Neglect Physical Neglect 11% 28% 21% 27% 23% 17% 13% 6% 15% 10%
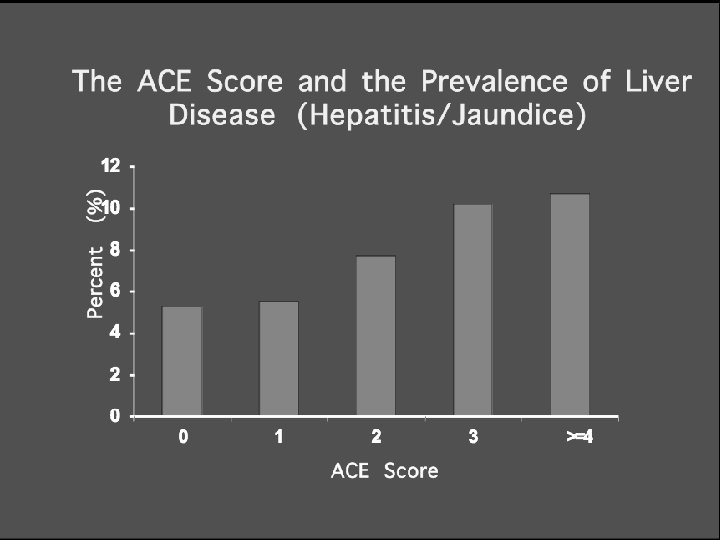
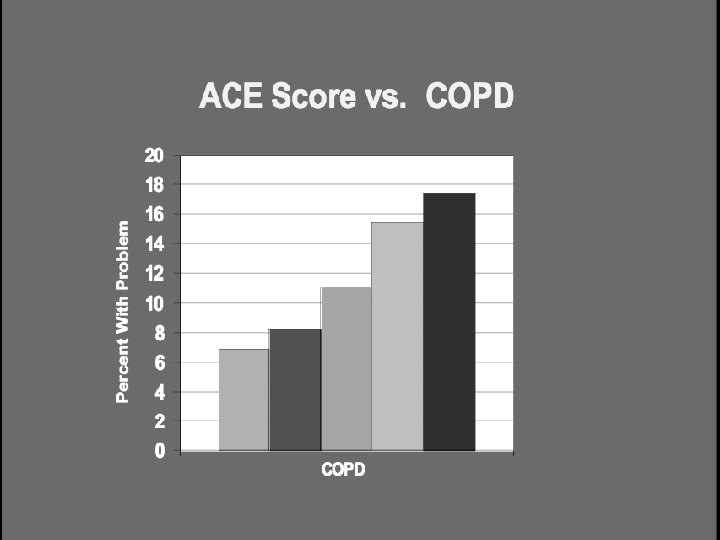
The Higher the ACE Sore , the greater the likelihood of: Severe and persistent emotional problems Health risk behaviors Serious social problems Adult disease and disability High health and mental health care costs Poor life expectancy The following information and slides are from September 2003 Presentation at “Snowbird Conference” of the Child Trauma Treatment Network of the Intermountain West, by Vincent J. Felitti, MD. And from Lanius/Vermetten Book Chapter 6/2007
Emotional Problems
Childhood Experiences Underlie Chronic Depression
Childhood Experiences Underlie Suicide 4+ 3 2 0 1
ACE Score and Hallucinations Ever Hallucinated* (%) 12 10 Abused Alcohol or Drugs 8 No 6 Yes 4 2 0 0 1 2 3 4 5 6 ACE Score *Adjusted for age, sex, race, and education. >=7
Health Risk Behaviors
Adverse Childhood Experiences and Current Smoking 20 18 16 14 12 10 % 8 6 4 2 0 0 1 2 ACE Score 3 4 -5 6 or more
Childhood Experiences and Adult Alcoholism 4+ 3 2 1 0
Basic cause of addiction is experiencedependent, not substance-dependent Significant implications for medical practice and treatment programs Where there’s smoke…
Serious Social Problems
Childhood Experiences Underlie Rape 4+ 2 1 0 3
Adverse Childhood Experiences and Likelihood of > 50 Sexual Partners
ACE Score and Indicators of Impaired Worker Performance Prevalence of Impaired Performance (%) 25 20 ACE Score 0 1 2 3 4 or more 15 10 5 0 Absenteeism (>2 Serious Financial days/month Poblems Serious Job Problems
Adult Disease & Disability
Adverse Childhood Experiences and History of STD
Poor Life Expectancy
Effect of ACEs on Mortality Age Group
Impact of Trauma Over the Life Span ACE Study - effects are neurological, biological, psychological and social in nature, including: � Changes in neurobiology � Social, emotional and cognitive impairment � Adoption of health-risk behaviors as coping mechanisms � Severe and persistent behavioral health, physical health, social problems, and early death
The Take Home Message Trauma is pervasive The impact of trauma is broad and touches many life domains The impact of trauma is often deep and life-shaping Trauma affects the way people approach helpful relationships Trauma does occur in the service context itself
Traditional Approach vs. Trauma Theory Traditional approach � You are sick � You are bad � You are sick and bad Trauma theory � You are not sick or bad � You are injured
from “WHAT IS WRONG WITH YOU? ” to “WHAT HAPPENED TO YOU? ”
Understanding of Service Relationship Traditional Hierarchical staff / patient relationship The patient is seen as passive recipient of services The patient’s feelings of safety and trust are taken for granted Trauma-Informed A collaborative relationship between the patient and the provider of her / his choice Both the patient and the provider are assumed to have valid and valuable knowledge bases The patient is an active planner and participant services The patient’s safety must be guaranteed and trust must be developed over time
Trauma Informed Care (TIC) “Trauma-Informed Care is a strengths-based framework that is grounded in an understanding of and responsiveness to the impact of trauma, that emphasizes physical, psychological, and emotional safety for both providers and survivors to rebuild a sense of control and empowerment. ” (Hopper et al, 2010) “Trauma-informed organizations, programs, and services are based on an understanding of the vulnerabilities or triggers of trauma survivors that traditional service delivery approaches may exacerbate, so that these services and programs can be more supportive and avoid retraumatization. ” (SAMHAS)
What does Trauma Informed Care offer? Improves our desired outcomes Supports trauma recovery by � � Reducing re-traumatization Providing “corrective emotional experience” Decreases our own vicarious trauma or compassion fatigue
Core Principles of Trauma Informed Care � Awareness: Everyone knows the role of trauma � Safety: Ensuring physical and emotional safety � � Trustworthiness: Maximizing trustworthiness, making tasks clear, and maintaining appropriate boundaries Choice: Respect and prioritize consumer choice and control Collaboration: Maximizing collaboration and sharing of power with consumers Empowerment: Prioritizing consumer empowerment
Tips for Practicing TIC � Recognize adaptive behaviors serve a purpose � Why is a person chronically miss morning appointments? Is the morning the only time she can sleep? Does she have a traumatic brain injury that prevents her from remembering things? � Make adjustments to help that person succeed. Set appointment times for the afternoon. � Include everyone in your agency � From receptionist to treatment staff � Provide trauma training to every employee
Quick & Easy � Offer support and validation � Communicate care and concern � Avoid passing judgment � Ask questions � Find � out about life experiences Listen for understanding � Resist interrupting � Make sure your body language is receptive � Offer information and assistance � Give resources
Guiding Values of Trauma-Informed Care “Healing Happens in Relationship”
TOP TEN SIGNS YOU’RE PROVIDING TRAUMA INFORMED CHILD WELFARE SERVICES Thanks to David Letterman
You know you’re providing trauma informed services when… 10. …you recognize the presence of secondary trauma and the importance of self care for you and your staff 9. …you are conducting full trauma assessments on all consumers 8. …you are designing collaborative service plans with the input of the consumer to maximize their voice and choice
You know you’re providing trauma informed services when… 7. …you proactively seek training in the implementation of trauma informed care and trauma specific services 6. …you engage parents, guardians, and other identified supports in the healing process by educating them on the presentation of traumatic stress 5. …you research the best trauma treatment model that will work with your agency’s population
You know you’re providing trauma informed services when… 4. …you aid consumers in identifying coping strategies that acknowledge trauma history and reinforces an understanding of behavior 3. …you help consumers and families build their community supports to aid in their ability to “bounce back” and develop resilience in all domains of development 2. …you are aware of sanctuary trauma and work with agency staff (clinical and direct care) to mitigate re-traumatizing youth in care
And the #1 way you know if you’re providing trauma informed services is… …you assume that all consumers that you are working with (and the individuals connected to them) are coping with the effects of trauma, and modify your approach in every way to ensure you’re practicing through a trauma focused lens
“If you think you’re too small to make a difference, try sleeping in a room with a mosquito. ” African Proverb
Professional Resources ACE Study. The Centers for Disease Control and Prevention reports on the Adverse Childhood Experiences (ACE) Study one of the largest investigations ever conducted on the links between childhood maltreatment and later-life health and wellbeing. www. cdc. gov/nccdphp/ace National Center for Posttraumatic Stress Disorder, http: //www. ncptsd. org National Child Traumatic Stress Network, http: //www. nctsn. org The National Working Group on Evidence-Based Health Care. www. evidencebasedhealthcare. org.