Understanding the interrelated cardiorenalmetabolic CRM systems EDUCATIONAL SLIDE
 systems EDUCATIONAL SLIDE MODULE Date of preparation: July 2020")
Understanding the interrelated cardio-renal-metabolic (CRM) systems EDUCATIONAL SLIDE MODULE Date of preparation: July 2020 Version 1. 0

Contents Introduction to the interrelated cardio-renal-metabolic systems Changing the outcomes of cardio-renal-metabolic conditions Cardio-renal-metabolic conditions in guidelines for patients with T 2 D 2

Contents Introduction to the interrelated cardio-renal-metabolic systems Changing the outcomes of cardio-renal-metabolic conditions Cardio-renal-metabolic conditions in guidelines for patients with T 2 D 3
 systems are interrelated The heart is the most “metabolically demanding” organ,")
The cardio-renal-metabolic (CRM) systems are interrelated The heart is the most “metabolically demanding” organ, susceptible to changes in volume and metabolism 1, 2 Regulation of energy metabolism by liver, pancreas and fat is essential for healthy function of organs, especially the heart and kidneys 1– 4 The kidneys play a key role in glucose and volume homeostasis, and blood pressure regulation 5, 6 CRM, cardio-renal-metabolic 1. Lopashuk GD & Ussher JR. Circ Res 2016; 119: 1173; 2. Song MK et al. J Diabetes Res. 2014; 2014: e 313718. 3. Connell AW et al. J Am Soc Hypertens 2014; 8: 604; 4. de Boer IH & Utzschneider KM. Nephrol Dial Transplant 2017; 32: 588; 5. García-Donaire JA & Ruilope LM. Int J Nephrol 2011; 2011: 975782; 6. Alsahli M & Gerich JE Diabetes Res Clin Pract 2017; 133: 1 4

The CRM systems are interrelated; acute or chronic dysfunction in the heart, kidneys or metabolic system may induce dysfunction in the other 1– 4 Each dysfunctional organ has the ability to initiate and perpetuate disease in the other organs through haemodynamic, neurohormonal and immunological/biochemical feedback pathways 1, 2 T 2 D is a risk factor for diseases related to the cardiac and renal systems 3 CRM, cardio-renal-metabolic 1. Song MK et al. J Diabetes Res 2014; 2014: e 313718; 2. Rangaswami J et al. Circulation 2019; 139: e 840; 3. House AA et al. Kidney Int 2019; 95: 1304; 4. Raghavan K et al. Cardiorenal Med 2019; 9: 240 5

Diseases of the CRM systems share many of the same risk factors 1 Progression of interrelated diseases (T 2 D, CV disease, HF and CKD) can occur due to dysfunction of the CRM systems, which, in turn, may lead to an increased risk of CV death 2– 4 = Diabetes and metabolic risk factors = Kidney disease = CV disease CRM, cardio-renal-metabolic; LV, left ventricular Adapted from Dzau VJ et al. 5 1. Sarafidis PA et al. J Cardiometab Syndr 2006; 1: 58; 2. Ronco C. Contrib Nephrol 2010; 164: 33; 3. Banerjee S and Panas R. Hellenic J Cardiol 2017; 58: 342; 4. Leon BM and Maddox TM. World J Diabetes 2015; 6: 1246; 5. Dzau VJ et al. Circulation 2006; 114: 2850 6

Metabolic dysfunction adds to cardiac and renal burden Metabolic abnormalities affect cardiac and renal disease progression and outcomes* Energy metabolism Hyperglycaemia 1 Dyslipidaemia 2, 3 Insulin resistance 2 Altered hormonal milieu 2 Adipokines 2 Fluid retention 4, 5 Albuminuria 2 Declining kidney function 2 Heart failure 3 Vascular dysfunction 2 Atherosclerosis 3 *Pathophysiological effects shown are an example and not exhaustive 1. Song MK et al. J Diabetes Res 2014; 2014: e 313718; 2. Connell AW & Sowers JR. J Am Soc Hypertens 2014; 8: 604; 3. Lopashuk GD & Ussher JR. Circ Res 2016; 119: 1173; 4. Ronco C et al. J Am Coll Cardiol 2008; 52: 1527; 5. Cabundugama PK et al. Med Clin North Am 2017; 101: 129 7

Cardiac dysfunction adds to renal and metabolic burden Cardiac abnormalities affect renal and metabolic disease progression and outcomes* Cardiac Neurohormonal activation 1, 2 Hypoperfusion 2 Volume overload 2 Arterial resistance 3 Change in substrate utilisation 4 Autonomic dysfunction 1, 2 Insulin resistance 1 FFA and dyslipidaemia 4 Hypertension 1, 2 Albuminuria 1, 2 Declining kidney function 1 *Pathophysiological effects shown are an example and not exhaustive FFA, free fatty acids 1. Connell AW & Sowers JR. J Am Soc Hypertens 2014; 8: 604; 2. Ronco C et al. J Am Coll Cardiol 2008; 52: 1527; 3. Cabundugama PK et al. Med Clin North Am 2017; 101: 129; 4. Lopashuk GD & Ussher JR. Circ Res 2016; 119: 1173 8

Renal dysfunction adds to cardiac and metabolic burden Renal abnormalities affect cardiac and metabolic disease progression and outcomes* Renal 1, 2 Activation of the RAAS and SNS Sodium and fluid retention Hypertension Arterial calcification Oxidative stress Insulin resistance 1 Abnormal glucose levels 1 *Pathophysiological effects shown are an example and not exhaustive RAAS, renin–angiotensin–aldosterone system; SNS, sympathetic nervous system 1. Connell AW & Sowers JR. J Am Soc Hypertens 2014; 8: 604; 2. Ronco C et al. J Am Coll Cardiol 2008; 52: 1527 Ventricular hypertrophy 2 Heart failure 1 Vascular dysfunction 1, 2 Atherosclerosis 2 9

Patients with T 2 D have multiple risk factors that contribute to CRM diseases • ~55% of patients with T 2 D have NAFLD 1 • Over half of patients with T 2 D are reported to be obese 2 • T 2 D reduces life expectancy by ~6 years*3 CV disease/ HF T 2 D • T 2 D further reduces life expectancy in patients with cardio–renal comorbidities 3, 4 CKD *Average for men and women aged 60 years CRM, cardio-renal-metabolic; NAFLD, non-alcoholic fatty liver disease 1. Younossi ZM et al. J Hepatology 2019; 71: 793; 2. Masmiquel L et al. Cardiovasc Diabetol 2016; 15: 29; 3. The Emerging Risk Factors Collaboration. JAMA 2015; 314: 52; 4. Wen C et al. Kidney Int 2017; 92: 388 10

Patients with T 2 D are at increased risk of complications such as CV disease and HF • Approximately one in three patients with T 2 D has CV disease 1 • There is a 2 - to 5 -fold increased risk of HHF* in patients with T 2 D† 2 • CV disease is the leading cause of mortality in patients with T 2 D 3, 4 *Versus those without T 2 D; †Patients with T 2 D aged <55 years HHF, hospitalisation for heart failure 1. International Diabetes Foundation. Diabetes Atlas 9 th Edition. http: //www. diabetesatlas. org (accessed June 2020); 2. Rosengren A et al. Diabetologia 2018; 61: 2300; 3. Morrish NJ et al. Diabetologia 2001; 44(Suppl. 2): S 14; 4. Davies MJ et al. Diabetes Care 2018; 41: 2669 11

The presence of CKD increases the risk of CV morbidity and mortality • Up to 67% of patients with HF are estimated to have CKD 1 • Risk of CV death increases as kidney function declines 2 • Presence of CKD in patients with HF increases risk of mortality by ~25– 28%3 1. Sarraf M et al. Clin J Am Soc Nephrol 2009; 4: 2013; 2. Matsushita K et al. Lancet 2010; 375: 2073; 3. Ather S et al. J Am Coll Cardiol 2012; 59: 998 12

Patients with T 2 D are at increased risk of complications such as CKD • CKD affects up to 40% of patients with T 2 D 1, 2 • Diabetes and/or hypertension is the cause of >80% of ESKD cases worldwide 1 • Life expectancy is reduced in patients with T 2 D and early CKD by 16 years – 10 more years than CKD alone*3 *Average of men/women and compared with those without diabetes or CKD ESKD, end-stage kidney disease 1. International Diabetes Foundation. Diabetes Atlas 9 th Edition. http: //www. diabetesatlas. org (accessed June 2020); 2. Umanath K & Lewis JB. Am J Kidney Dis 2018; 71: 884. 3. Wen C et al. Kidney Int 2017; 92: 388 13

Contents Introduction to the interrelated cardio-renal-metabolic systems Changing the outcomes of cardio-renal-metabolic conditions Cardio-renal-metabolic conditions in guidelines for patients with T 2 D 14

Multifactorial management of the CV risk factors is well established as standard of care for patients with T 2 D 1, 2 ADA and ESC guidelines focus on reducing the risk of CV death in patients with T 2 D 1, 2 Target Treatment Glucose control Targets are individualised – for many patients Hb. A 1 c <7%1, 2 • Metformin, SGLT 2 inhibitors*, GLP-1 receptor agonists†, DPP-4 inhibitors, sulphonylureas, thiazolidinediones, insulin 1, 2 Blood pressurelowering For individuals with T 2 D and hypertension, a blood pressure target of: • <130/80 mm. Hg if at higher CV risk‡ 1 • <140/90 mm. Hg if at lower risk for CV disease§ 1 • RAAS blocker (ACEi/ARB), calcium channel blocker, thiazide-like diuretics 1, 2 • Dual therapy is recommended as first-line treatment 2 LDL cholesterollowering • <1. 8 mmol/l (<70 mg/dl) with LDL-C reduction of ≥ 50% if at high CV risk 1, 2 • <2. 6 mmol/l (<100 mg/dl) if at moderate CV risk 2 • Statins, ezetimibe or PCSK 9 inhibitor 1, 2 Weight loss and smoking cessation 1, 2 • Diet 1, 2 • Physical activity 1, 2 • Behavioural therapy 1 Individualised diet and lifestyle For full recommendations, please refer to the individual references *Empagliflozin, canagliflozin and dapagliflozin reduce CV events in patients with diabetes and CV disease or who are at very high/high CV risk; †Liraglutide, semaglutide and dulaglutide reduce CV events in patients with diabetes and CV disease or who are at very high/high CV risk; ‡Existing ASCVD or 10 -year ASCVD risk ≥ 15%; § 10 -year ASCVD risk <15%. ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ASCVD, atherosclerotic cardiovascular disease; PCSK 9, proprotein convertase subtilisin/kexin type 9; RAAS, renin-angiotensin-aldosterone system 1. American Diabetes Association. Diabetes Care 2020; 43: S 1; 2. Cosentino F et al. Eur Heart J 2020; 7: 255 15

SGLT 2 inhibitors and GLP-1 RAs provide benefits across the CRM systems, complementing the effects of standard of care treatment • • Metabolic effects Cardio–renal benefits†‡ Reduction of: • MACE • CV death • HHF • Hard kidney outcomes • Albuminuria • e. GFR worsening Statins 1, 2 MRA 3 ACEi/ ARBs 1, 4 SGLT 2 inhibitors 3, 5 GLP-1 RAs 3, 5 Reduce albuminuria* CV benefits Cardio–renal benefits Metabolic effects Cardio–renal benefits†‡§ Reduction of: • MACE • CV death • Albuminuria *Effect with statins has been modest and variable across studies; †SGLT 2 inhibitors have an ‘A’ level of evidence and GLP-1 RAs have a ‘C’ level of evidence for kidney disease recommendations; 3 ‡For specific agent characteristics, see relevant local label; §In patients with T 2 D and ASCVD where MACE is the gravest threat, the level of evidence is greatest for GLP-1 RAs. 6 ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ASCVD, atherosclerotic CV disease; CRM, cardio-renal-metabolic; HHF, hospitalisation for heart failure; MRA, mineralocorticoid receptor antagonist. 1. Ponikowski P et al. Eur Heart J 2016; 37: 2129; 2. Shen X et al. Lipids Health Dis 2016; 15: 179; 3. American Diabetes Association. Diabetes Care 2020; 43: S 1; 4. KDIGO. Kidney Int Suppl 2012; 2: 405; 5. Zelniker TA et al. Circulation 2019; 139: 2022; 6. Buse JB et al. Diabetes Care 2020; 43: 487 16

Limited CV benefits have been observed with intensive glycaemic control in patients with T 2 D Meta-analysis of the ACCORD, ADVANCE, UKPDS and VADT studies* Objective: to generate precise estimates of the effects of glucose-lowering therapy on major CV events Patients with T 2 D (N=27, 049) allocated to ‘More intensive’ or ‘Less intensive’ glycaemic control Major CV events (CV death or non-fatal stroke or non-fatal MI) Modest benefit HR 0. 91 (0. 84, 0. 99) All-cause mortality No effect HR 1. 04 (0. 90, 1. 20) *The trials differed in glucose-lowering and cardioprotective therapies at follow-up. The studies used metformin, insulin, sulphonylurea, acarbose, glinide and thiazolidinedione as glucose-lowering agents Turnbull FM et al. Diabetologia 2009; 52: 2288 17

Despite treating to goal, a significant residual risk for kidney disease progression remains Primary kidney outcome in patients treated to predefined targets for Hb. A 1 c, BP and lipids* Primary composite endpoint† (%) 50 40 RR 0. 43 (95% CI 0. 21, 0. 86) 30 <3 treatment targets attained ~60% risk reduction 20 ≥ 3 treatment targets attained 10 Residual risk 0 0 5 10 15 20 25 Follow-up (months) *Predefined protocol/targets were: Hb. A 1 c <7%; BP <130/80 mm. Hg; LDL-C <2. 6 m. M; triglyceride <2 m. M; persistence with RAAS inhibitors; †Death and/or ESKD, defined as dialysis or the need for dialysis, or plasma creatinine level ≥ 500 µmol/l RAAS, renin–angiotensin–aldosterone system; RR, relative risk Chan JC et al. Diabetes Care 2009; 32: 977 18

Multifactorial control of CV risk factors reduced CV risk in patients with T 2 D Steno-2: Intensive multifactorial control* of CV risk factors reduces CV risk in patients with T 2 D and microalbuminuria 1, 2 All patients received intensive control at 7. 8 years 100 Death or CV disease event† (%) 21 -year follow up: Unadjusted HR 0. 55 (95% CI 0. 39, 0. 77); p<0. 001 Conventional (51 events) 75 50 Intensive (35 events) 25 0 0 No. at risk Intensive 80 Conventional 80 4 66 61 7. 8 8 12 Years since randomisation 56 40 49 27 16 20 41 18 31 13 Changes in key clinical and biochemical variables at 7. 8 years 2 Variable Conventional (n=63) Intensive (n=67) p-value Systolic BP (mm. Hg) -3± 3 -14± 2 <0. 001 Diastolic BP (mm. Hg) -8± 2 -12± 2 0. 006 LDL cholesterol (mg/dl) -13± 6 -47± 5 <0. 001 Hb. A 1 c (%) 0. 2± 0. 3 -0. 5± 0. 2 <0. 001 BMI (men) 0. 4± 0. 4 0. 7± 0. 4 0. 61 BMI (women) 1. 3± 1. 3 2. 3± 1. 2 0. 29 -6 -5 0. 73 Current smoker (no. of patients) Treatment benefit was observed after ~4 years; the continuing beneficial effects over time were a direct consequence of early intervention intensification in patients *Intensive multifactorial control consisted of reduced targets for blood pressure, cholesterol, triglycerides and Hb. A 1 c, as well as treatment with aspirin and ACEi; †Composite secondary endpoint: time to incident CV disease, number of CV events, mortality and CV disease rates ACEi, angiotensin-converting enzyme inhibitor, BMI, body mass index; LDL, low-density lipoprotein 1. Gaede P et al. Diabetologia 2016; 59: 2298; 2. Gaede P et al. N Engl J Med 2003; 348: 383 19

CV death: only empagliflozin and liraglutide have shown a significant risk reduction in CVOTs in patients with T 2 D Drug class Trial (study drug) SGLT 2 inhibitor GLP-1 receptor agonist HR (95% CI) p-value EMPA-REG OUTCOME 1 (empagliflozin) 0. 62 (0. 49, 0. 77) <0. 001* CANVAS Program 2 (canagliflozin) 0. 87 (0. 72, 1. 06) NR† DECLARE-TIMI 583 (dapagliflozin) 0. 98 (0. 82, 1. 17) NR† ELIXA 4 (lixisenatide) 0. 98 (0. 78, 1. 22) 0. 85 LEADER 5 (liraglutide) 0. 78 (0. 66, 0. 93) 0. 007* SUSTAIN-66 (inj. semaglutide) 0. 98 (0. 65, 1. 48) 0. 92 PIONEER 6‡§ 7(oral semaglutide) 0. 49 (0. 27, 0. 92) NR† EXSCEL§ 8 (exenatide) 0. 88 (0. 76, 1. 02) NR† Harmony Outcomes 9 (albiglutide) 0. 93 (0. 73, 1. 19) 0. 578 REWIND§ 10 (dulaglutide) 0. 91 (0. 78, 1. 06) 0. 21 0, 25 0, 5 Favours study drug 1 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Empagliflozin is FDA approved to reduce the risk of CV death *Nominal p-value; †p-value not reported in publication; ‡PIONEER 6 only had 45 total CV death events and was an exploratory outcome due to MACE superiority not being achieved in the statistical testing hierarchy; §Includes death from unknown cause. NR, not reported See slide notes for full list of references 2 Favours placebo 21
 SGLT 2 inhibitor GLP-1 receptor agonist HR (95% CI)")
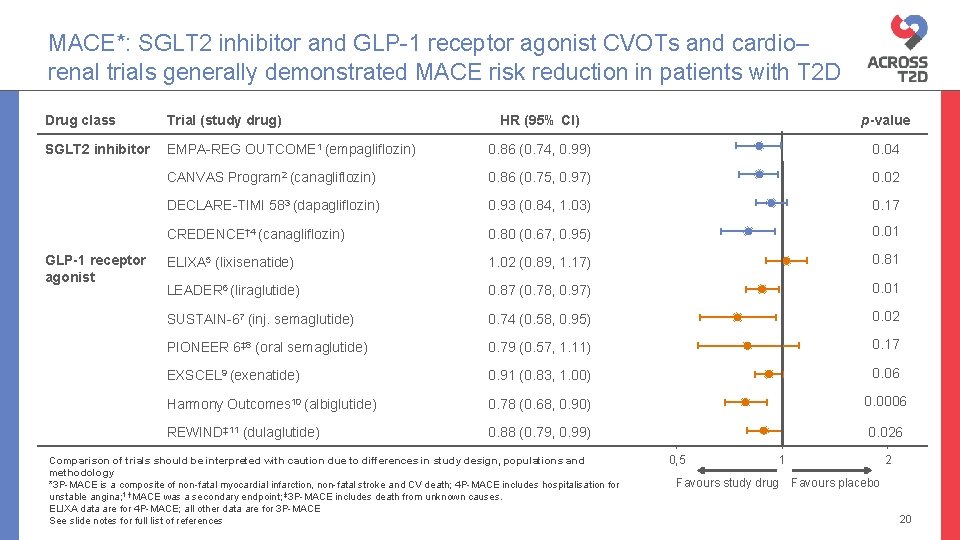
Drug class Trial (study drug) SGLT 2 inhibitor GLP-1 receptor agonist HR (95% CI) p-value EMPA-REG OUTCOME 1 (empagliflozin) 0. 65 (0. 50, 0. 85) 0. 002† CANVAS Program 2 (canagliflozin) 0. 67 (0. 52, 0. 87) NR‡ DECLARE-TIMI 583 (dapagliflozin) 0. 73 (0. 61, 0. 88) NR‡ CREDENCE 4 (canagliflozin) 0. 61 (0. 47, 0. 80) <0. 001 DAPA-HF§ 5 (dapagliflozin) 0. 70 (0. 59, 0. 83) NR‡ ELIXA 6 (lixisenatide) 0. 96 (0. 75, 1. 23) 0. 75† LEADER 7 (liraglutide) 0. 87 (0. 73, 1. 05) 0. 14† SUSTAIN-68 (inj. semaglutide) 1. 11 (0. 77, 1. 61) 0. 57† PIONEER 69 (oral semaglutide) 0. 86 (0. 48, 1. 55) NR‡ EXSCEL 10 (exenatide) 0. 94 (0. 78, 1. 13) NR‡ REWIND¶ 11 (dulaglutide) 0. 93 (0. 77, 1. 12) 0. 46†

Hard kidney outcomes: SGLT 2 inhibitor and GLP-1 receptor agonist CVOTs and cardio–renal trials in patients with T 2 D* Patients Events Weights (%) HR (95% CI) CREDENCE (canagliflozin)2 4401 377 – 0. 66 (0. 53, 0. 81) EMPA-REG OUTCOME (empagliflozin) 6968 152 20. 9 0. 54 (0. 40, 0. 75) CANVAS Program (canagliflozin) 10, 142 249 34. 0 0. 60 (0. 47, 0. 77) DECLARE-TIMI 58 (dapagliflozin) 17, 160 365 45. 1 0. 53 (0. 43, 0. 66) ELIXA (lixisenatide) 6063 76 9. 5 1. 16 (0. 74, 1. 83) LEADER (liraglutide) 9340 184 23. 4 0. 89 (0. 67, 1. 19) SUSTAIN-6 (inj. semaglutide) 3297 32 4. 0 1. 28 (0. 64, 2. 58) 12, 914 519 63. 1 0. 88 (0. 74, 1. 05) HR (95% CI) SGLT 2 inhibitor* † 1 GLP-1 receptor agonist*‡§ 1 EXSCEL (exenatide) 0, 25 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology p-value for subgroup differences between SGLT 2 inhibitors and GLP-1 receptor agonists was <0. 001 (excluding CREDENCE) *Hard kidney outcomes (excluding albuminuria, including e. GFR decline) were most commonly doubling of serum creatinine or need for chronic dialysis, ESKD and death due to kidney causes; †Q statistic=0. 59; p=0. 74, I 2=0% (excluding CREDENCE); ‡Q statistic=2. 18; p=0. 54, I 2=0%; §PIONEER 6 did not report any kidney outcomes ¶Doubling of serum creatinine, initiation of dialysis, renal transplantation or creatinine >6. 0 mg/dl; **Sustained ESKD, sustained ≥ 40% decrease in e. GFR from baseline or death from kidney failure See slide notes for abbreviations and references 0, 5 Favours study drug 1 2 Favours placebo 23

Composite kidney outcomes: SGLT 2 inhibitor and GLP-1 receptor agonist CVOTs and cardiorenal trials in patients with T 2 D Patients Events Weights (%) HR (95% CI) EMPA-REG OUTCOME (empagliflozin) 6185 913 24. 9 0. 61 (0. 53, 0. 70) CANVAS Program (canagliflozin) 10142 847 25. 0 0. 57 (0. 50, 0. 66) DECLARE-TIMI 58 (dapagliflozin) 17160 1675 50. 1 0. 66 (0. 60, 0. 73) CREDENCE (canagliflozin)‡ 2 4401 585 – 0. 70 (0. 59, 0. 82) ELIXA (lixisenatide) 5286 375 20. 0 0. 84 (0. 68, 1. 02) LEADER (liraglutide) 9340 605 32. 2 0. 78 (0. 67, 0. 92) SUSTAIN-6 (inj. semaglutide) 3297 162 7. 7 0. 64 (0. 46, 0. 88) EXSCEL (exenatide) 14752 773 40. 1 0. 88 (0. 76, 1. 01) REWIND (dulaglutide)3 9901 1338 – 0. 76 (0. 68, 0. 84) HR (95% CI) SGLT 2 inhibitor* † 1 GLP-1 receptor agonist*§¶ 1 0, 25 0, 5 Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology Favours p-value for subgroup differences between SGLT 2 inhibitors and GLP-1 receptor agonists was 0. 01(excluding CREDENCE and REWIND) *Composite kidney outcomes were mostly new-onset macroalbuminuria, sustained doubling of serum creatinine or a 40% decline in e. GFR, ESKD or death due to kidney causes; †Q statistic=2. 99; p=0. 22, I 2=33. 2% (excluding CREDENCE); ‡Primary outcome; §Q statistic=3. 60; p=0. 31, I 2=16. 6% (excluding REWIND); ¶PIONEER 6 did not report any kidney outcomes See slide notes for full list of references study drug 1 2 Favours placebo 24

Summary of CV, HF and kidney outcomes with drugs used for the management of patients with T 2 D SGLT 2 i 1– 5 GLP-1 RA 6– 14 ACEi 15, 16 ARB 17– 20 P P MACE CV death Empagliflozin only Statins 21– 24 Liraglutide only* HHF Hard kidney outcomes† Albuminuria All-cause mortality Empagliflozin only Liraglutide only* P P Comparison of trials should be interpreted with caution due to differences in study design, populations and methodology *PIONEER 6 (oral semaglutide) was not powered to show a CV death risk reduction or reduction in all-cause mortality (CV death=45 events; all-cause mortality=68 events); †Most commonly doubling serum creatinine, ESKD, renal death; ‡Effect has been modest and variable across studies ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNi, angiotensin receptor-neprilysin inhibitor; HHF, hospitalisation for heart failure ‡ P 25

Effects of SGLT 2 inhibitors on the CRM systems may be mediated via multiple mechanisms SGLT 2 inhibitors 1, 2 Intermediate effects 3– 8 Diuresis Glucose excretion Myocardial sodium content due to inhibition of Na+/H+ exchange receptors Intraglomerular pressure Downstream observed effects 9, 10 Afterload (improved vascular function) CV events Kidney disease LV wall stress/ LV mass Preload (decreased interstitial volume) Blood pressure Body weight Natriuresis Bioenergetics Inflammation and oxidative stress (fibrosis) Haematocrit Hb. A 1 c CRM, cardio-renal-metabolic; LV, left ventricular 1. Vallon V & Thomson SC. Diabetologia 2017; 60: 215; 2. Heise T et al. Clin Ther 2016; 38: 2265; 3. Verma S et al. Circulation 2019; 140: 1693; 4. Verma S et al. JAMA Cardiol 2017; 2: 939; 5. Abdelgadir E et al. J Clin Med Res 2018; 10: 615; 6. Rajasekeran H et al. Kidney Int 2016; 89: 524; 7. Baartscheer A et al. Diabetologia 2017; 60: 568; 8. Garg V et al. Prog Cardiovasc Dis 2019; 62: 349; 9. Zinman B et al. N Engl J Med 2015: 373: 2117; 10. Wanner C et al. N Engl J Med 2016; 375: 323 26

Effects of GLP-1 receptor agonists on the CRM systems GLP-1 receptor agonists 1– 3 Intermediate effects 2, 4 Insulin secretion 1, 2 CV events Glucagon suppression 1, 2 Albuminuria Inflammation 2 Coagulation 4 Natriuresis 3 Diuresis 3 Appetite suppression 1, 2 Downstream observed effects 2, 5 Blood pressure Postprandial lipids 2 LV function 2 Body weight Hb. A 1 c CRM, cardio-renal-metabolic. Adapted from Drucker 1 and Rizzo et al. 2 1. Drucker DJ. Cell Metab 2018; 27: 740; 2. Rizzo M et al. Biochim Biophys Acta Mol Basis Dis 2018; 1864: 2814; 3. Greco EV et al. Medicina 2019; 55: 233; 4. Cameron-Vendrig et al. Diabetes 2016; 65: 1714; 5. Zelniker TA et al. Circulation 2019; 139: 2022 27

Contents Introduction to the interrelated cardio-renal-metabolic systems Changing the outcomes of cardio-renal-metabolic conditions Cardio-renal-metabolic conditions in guidelines for patients with T 2 D 28

A holistic approach to T 2 D care addresses the cardio, renal and metabolic aspects of disease Reduce MACE 4 Reduce CV events 1– 4 Reduce CKD progression 3– 5 Reduce CV events in patients with high CV risk/established ASCVD 3, 4 Reduce HHF 3, 6 Control risk factors for disease progression 4 For full recommendations, please refer to the individual references and guidelines or the AT 2 D module ‘Evolving evidence-based recommendations in T 2 D’ HHF, hospitalisation for heart failure; LV, left ventricular Adapted from Dzau VJ et al. 7 See slide notes for full list of references Reduce risk of CV death 3, 4 29

Since 2016, guidelines and societies have been recommending the use of SGLT 2 inhibitors and/or GLP-1 receptor agonists for their CRM benefits … 2015 2016 2018 2019 Glycaemic control 1, 2 CV and mortality benefits Benefits in ASCVD and chronic HF 7 Nephroprotection in T 2 D + CKD + DKD ADA/EASD: SGLT 2 inhibitors and GLP-1 RAs recommended as glucose-lowering agents only CDA: Empagliflozin recommended to reduce the risk of CV and all-cause mortality (Feb)3 ESC: Empagliflozin recommended to prevent or delay the onset of HF and prolong life (May)4, 5 ADA: Empagliflozin and canagliflozin recommended as agents with proven benefit on MACE and CV death; liraglutide has ASCVD benefit only ERA–EDTA and ESC/EASD recommended use of SGLT 2 inhibitors with evidence for cardio- and nephroprotection; 8 to reduce progression of DKD 9 Use GLP-1 RAs if SGLT 2 inhibitors not tolerated 8 2020 Independent of Hb. A 1 c; ASCVD, HF or CKD predominates 10 ADA: recommended GLP-1 RAs or SGLT 2 inhibitors with proven CVD benefit if ASCVD predominates SGLT 2 inhibitors with evidence of reducing HF and/or CKD if HF or CKD predominates CDA: Liraglutide recommended to reduce the risk of MACE (Sep)6 For full recommendations, please refer to the individual references and guidelines or the AT 2 D module ‘Evolving evidence-based recommendations in T 2 D’ ADA, American Diabetes Association; ASCVD, atherosclerotic cardiovascular disease; CDA, Canadian Diabetes Association; CRM, cardio-renal-metabolic; DKD, diabetic kidney disease; EASD, European Association for the Study of Diabetes ; ERA-EDTA, European Renal Association-European Dialysis and Transplant Association; ESC, European Society of Cardiology; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HHF, hospitalisation for heart failure See slide notes for full list of references 30

Dedicated heart failure and kidney outcomes trials with SGLT 2 inhibitors will add to the body of evidence 2018 2019 2020 2021 DAPA-CKD 6 CREDENCE 1 (dapagliflozin, stopped early for efficacy) (canagliflozin, stopped early for efficacy) DAPA-HF 2 (dapagliflozin, completed) SOLOIST*3 (sotagliflozin) EMPEROR-Reduced(Q 3)4 EMPEROR-Preserved(Q 4)5 2022 2023 2024 SCORED*8 (sotagliflozin) EMPA-KIDNEY 9 FLOW 10 (empagliflozin) (semaglutide) DELIVER 7 (dapagliflozin) (empagliflozin) Heart failure outcomes trial (patients with and without T 2 D) Kidney outcomes trial (patients with T 2 D only) Kidney outcomes trial (patients with and without T 2 D) Markers on the timeline represent estimated trial completion dates, except for CREDENCE and DAPA-HF 1. Perkovic V et al. N Engl J Med 2019; 380: 2295; 2. Mc. Murray J et al. N Engl J Med 2019; 381: 1995; 3. Clinical. Trials. gov. NCT 03521934; 4. Clinical. Trials. gov. NCT 03057977; 5. Clinical. Trials. gov. NCT 03057951; 6. Clinical. Trials. gov. NCT 03036150; 7. Clinical. Trials. gov. NCT 03619213; 8. Clinical. Trials. gov. NCT 03315143; 9. Clinical. Trials. gov. NCT 03594110; 10. Clinical. Trials. gov. NCT 03819153; 11. Lexicon Pharmaceuticals, Inc. Press release. 2020. http: //www. lexpharma. com/ (all websites accessed June 2020) 31

Understanding the interrelated CRM systems: summary The CRM systems are interrelated; dysfunction in one organ or system can induce or contribute to dysfunction in the others 1 T 2 D, CV disease, HF and CKD are interrelated and the presence of T 2 D is associated with cardiac and renal disease progression 2– 6 A holistic approach to T 2 D care is necessary to address the CV, renal and metabolic aspects of disease 7 Guidelines and societies recommend the use of agents with CRM benefits, such as SGLT 2 inhibitors and GLP-1 receptor agonists for the treatment of patients with T 2 D 8, 9 CRM, cardio-renal-metabolic See slide notes for full list of references 32
- Slides: 32