Understanding the Biological Basis of Psychotropic Drugs Drug

Understanding the Biological Basis of Psychotropic Drugs Drug Classes and Specific Drugs Nursing Implications Suzy Dalgarn RN, MSN, CNE NURS 135

Nursing responsibilities • • Assess for expected effects Know safety profiles…contraindications Recognize SE and adverse reactions Reinforce teaching points Therapeutic drug monitoring Assess for undiagnosed illnesses… Drugs that can induce psych symptoms Drug interactions…. inhibit or potentiate action

Principles • Medications are prescribed for target symptoms of psychiatric disorders • No drug just affects target symptoms • All drugs have unwanted effects some worse then others; side effects versus adverse reactions • Pay careful attention to black box warning

Pharmacodynamics; what drugs do to the body • Psychiatric meds primarily target the CNS at the cellular, synaptic level; – At either the receptor, ion channel, enzyme or carrier protein level

Drugs modify receptor by binding/or attaching to site can act as agonist to the receptor (initiate the response), or antagonist (inhibit the response) Benzodiazepines act as agonists for GABA Most antipsychotic drugs are antagonists to dopamine 5

At the ion channels, drugs can act to excite or inhibit response (potassium, calcium, sodium, chloride) 6
 and excretion/elimination")
Pharmacokinetics; what the body does to the drugs Absorption, distribution, metabolism (biotransformation) and excretion/elimination

Absorption Most absorption of oral drugs occurs in small intestine Food or antacids may slow rate/or change amount of drug absorbed bioavailability represents amount of the drug that actually reaches systemic circulation.

Distribution Amount of the drug found in various tissues. Factors affecting distribution; amount of blood flow, anatomic barriers (blood brain barrier), fat/protein content of organs Most psychotropic meds are lipohillic and highly protein bound unbound/free portion is active What is the potential problem if you are geriatric or malnourished?

Metabolism Most metabolism occurs in the liver…liver disease is a problem first pass effect : drugs metabolized by (cytohrome)P 450 enzyme system. only a fraction of the drug reaches systemic circulation inducer of the enzyme speeds up the metabolism of the drug inhibitor slows it down Example; Nicotine is a potent inducer for the enzyme that helps metabolize Clozapine, results in a decreased plasma level of the drug ****Genes play a part in the enzyme system Drug interactions…. SSRI’s, grapefruit juice, some typical antipsychotics inhibit liver enzymes. . ST Johns wort, tegretol potent inducers

Elimination/Excretion Clearance Half life Most psych drugs excreted through the liver and bile system Notable exception is lithium; excreted by the kidneys…kidney disease is a problem…

Geriatric Patient More sensitive to psychotropics Decreased intracellular water, decreased protein binding, low muscle mass, decreased metabolism, increased body fat concentration Tend to take multiple medications (increased risk for drug interactions) More likely to develop toxicity Start low go slow 12

3 T’s Tolerance taper down to avoid withdrawal symptoms Toxicity bloodstream levels poisonous to body…several factors increase likelihood Therapeutic index: relative measure of toxicity lithium lowest therapeutic index of psych drugs

The Brain weighs 2. 2 lbs Emotional regulation abstract and concrete thought language Motor regulation memory Blood Pressure, HR, BT Appetite, sleep Sexual Behavior Uses 25 % of glucose and O 2 Monitor of external world Arousal

Neural Plasticity • Brain develops/changes throughout life – neurodevelopment, drugs, infections, psychological experiences – Pruning of unneeded circuitry occurs in adolescence • several factors involved in the origin of mental illness but there will be eventually a change in cerebral function that accounts for the disturbances in clients behavior and mental experiences

Neuroanatomy implicated in psychiatric disturbances – Abnormalities in structure of the brain or in its ability to communicate can cause or contribute to mental disturbance – Mesolimbic/mesocortical pathways, HPA axis, cerebral cortex, neurotransmitter dysfunction all implicated

Neurotransmitters as Messengers

NEUROTRANSMITTER DEFICIENCY Each neurotransmitter has it’s own receptor site some have several; dopamine D 1, D 2, D 3, D 4, D 5)

Research is now looking at conditions/gene expression, protein synthesis “upstream”

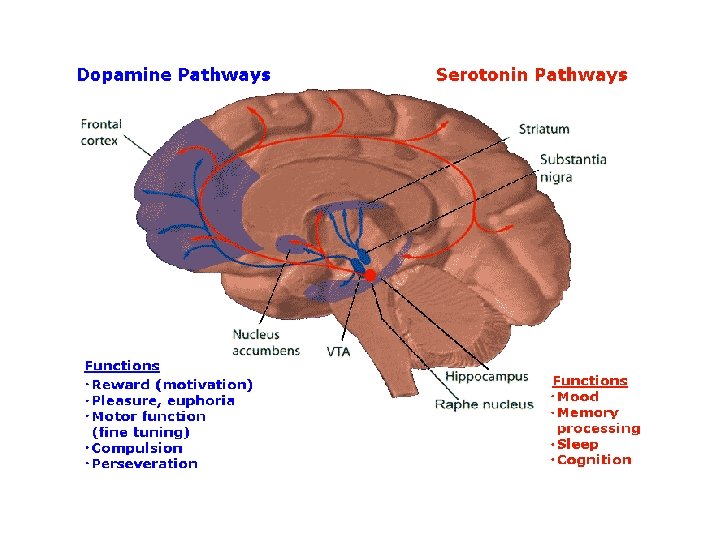
Dopamine Hypothesis in Schizophrenia • Dopamine antagonists decrease positive symptoms • Drugs that increase brain dopaminergic activity induce psychosis 21

PET SCAN: SCHIZOPHRENIA • Radioactive tracer settles in areas of high activity. • Functional assessment

Depression – Deficiency of norepinephrine – Deficiency of serotonin – Deficiency of both

Schizophrenia – Excess transmission of dopamine • Plays a role in integration of thoughts and emotions, too much is implicated in thought disturbances • Also plays a role in movement and regulation; so medications that are antagonistic have a potential to produce disturbances of movement
 • Potentiation of GABA action should result")
Anxiety – Deficiency of g-aminobutyric acid (GABA) • Potentiation of GABA action should result in anxiety reduction 25

Acetylcholine • neurotranmitter • Plays a role in learning and memory. • Drugs geared to prevent destruction of ACH by acetylcholinesterase would result in higher levels of acetylcholine with the potential for improved memory 26

Basis of Side Effects of Psychotropic Drugs • A particular transmitter is often used by different neurons to carry out different activities • Alterations in mental status, whether arising from disease or medication, are often accompanied by changes in basic drives, sleep patterns, body movement, and autonomic functions • Drugs come with side effects some can be beneficial, others not

Drug choice Factors to be considered; • Side effect profile • Ease of administration – What would be benefit of long acting drug for a client with schizophrenia? • History of past response • Co-morbid conditions – What drug is contraindicated for a patient with pre-existing heart disease?

Antipsychotic Drugs; sometimes called neuroleptics • For the treatment of schizophrenia and bipolar psychosis – For acute exacerbations – For prevention/mitigation of relapse – When a client stops taking a med, psychotic symptoms usually reoccur. – With each relapse it takes longer to gain a remission leading to a possibility that client becomes unresponsive to treatment

Indications And Evidence For Effectiveness • Positive Symptoms Of Schizophrenia – Hallucinations, delusions, disorganized thought processes and paranoia • Negative Symptoms Of Schizophrenia – Withdrawal, lack of initiative, failure to maintain hygiene, lack of interest – Traditional antipsychotics do not help well with the negative symptoms
 Antipsychotic Drugs • Strong antagonists (blocking agents) – Bind to D 2")
Conventional (First-Generation) Antipsychotic Drugs • Strong antagonists (blocking agents) – Bind to D 2 receptors – Block attachment of dopamine – Reduce dopaminergic transmission – Amphetamines/cocaine/ritalin/levodopa cause increase of dopamine. Can cause signs of psychosis – Newer drugs; less side effects, increase neurocognitive functioning – Disadvanatages • Side effects; EPS, zombie feeling, affective flattening, sedation, Advantages, low cost, available in depot form, improve positive symptoms

First Generation • Haldol, Prolixin Deconate, Thorazine • Block dopamine in both the limbic and basal ganglia • Dystonia (muscle stiffness) antiparkinson meds can help (benzatropine) 32
 Antipsychotic Drugs • Antagonists of receptors for – Acetylcholine; muscarinic receptor blockade")
Conventional (First-Generation) Antipsychotic Drugs • Antagonists of receptors for – Acetylcholine; muscarinic receptor blockade (dry mouth) – Norepinephrine (BP drop) – Histamine (sedation, weight gain) – Some adjust to side effects, for others it effects compliance
 • tardive dyskinesia • Lower")
Side Effects • EPS symptoms (akathisia, dystonia, and pseudoparkinsonism) • tardive dyskinesia • Lower seizure threshold • Neuroleptic malignant syndrome

EPS symptoms • Acute dystonia; muscle cramps of the head, neck • Akathisia; internal restlessness, and external restlessness (pacing inability to remain at rest) • Pseudoparkinsonism; stiffening of muscular activity in the face, body, arms and legs (frequently appears within first month, mimics parkinsons disease) • Treatment; change/lower drug, • Give Artane, or benztropine, or benadryl, or symmetrel. • Patients on typical antipsychotics are prescribed an anticholinergic to mitigate the EPS symptoms

Tardive Dyskinesia • Result of Prolonged treatment • More serious usually not reversible • Involuntary tonic muscular spasms (tongue, fingers, toes, neck) • AIMS scale (page 411)

Neuroleptic Malignant Syndrome • Results from acute reduction in dopamine activity • Fatal in 10 % of cases • Increasing muscle stiffness; leading to rigidity • Decreased loc, increased muscle tone, hyperpyreixa, labile HTN, tachycardia, tacyapnea • Dc antipsychotic, reduce temp, parlodel, dantrolene

Physiological Function of Dopamine • Inhibits release of prolactin from the anterior pituitary gland – Antagonism Leads to increased pituitary secretion of prolactin • In women – Antagonism leads to • Amenorrhea (absence of menses) • Galactorrhea (milk flow) • In men – Antagonism leads to Gynecomastia (development of male mammary glands)

Atypical Antipsychotics • Bind to dopamine receptors in the limbic system – Binds Preferentially over dopamine receptors in the basal ganglia – Fewer motor side effects – Also acts as antagonists for 5 HT 2 receptors (treats negative symptoms)

Clozapine first atypical – Possibly fatal side effects Agranulocytosis, convulsions, myocarditis – Other side effects Drowsiness, sedation, hypersalivation, tachycardia, dizziness

Agranulocytosis • Signs of infection should be reported to physician ASAP. • Clients on therapy should initially have WBC’s measured weekly

Risperidone – Side effects orthostatic hypertension, sedation Now available in long acting Consta (a good choice over prolixn deconate; traditional antipsychotic)
 • Haldol • fluphenazine")
Long Acting preparations • Consta (risperdal) • Haldol • fluphenazine
")
Others • Quetiapine: seroquel, sometimes diverted • Zyprexa: Olanzapine (now available in injectable; zydis) SE weight gain, good for agitation • Ziprasidone: geodon (take with food) • Aripiprazole; Ablifiy , less metabolic syndrome

Mood Stablizers • Treatment of bipolar disorder • Bipolar I; several meds, but mood stablizer is considered lifelong/maintenance for most • Overexcitement of neurons in some parts of the brain may lead to symptoms • Lithium and depakote are the 2 primary mood stabilizing drugs • Lithium a positively charged ion may act by affecting electrical conductivity in neurons. – Interacts with sodium and potassium to stabilize electrical activity – May take 7 -14 days to reach effective dose

Lithium • Adverse effects: cerebral convulsions, motor tremor • Has potential to affect electrical conductivity elsewhere besides the brain: includidng cardiac dysrhythmias, Lowest therapeutic index of almost any drug (ratio of lethal dose to effective dose) Signs of lithium toxicity; diaphoresis, slurred speech, moderate nausea (unrelieved by food)

Lithium • Regular monitoring • Initially biweekly until therapeutic levels have been reached • Narrow therapeutic window; 0. 4 to 1. 4 m. Eq/l • Elderly start low go slow
 drugs – Carbamazepine (Tegretol) – Divalproex (Depakote) – Lamotrigine")
Mood Stabilizers • Antiepileptic (anticonvulsant) drugs – Carbamazepine (Tegretol) – Divalproex (Depakote) – Lamotrigine (Lamictal) – Membrane stabilizing effect may account for the drugs ability to reduce mood swings

Antidepressant drugs • Treatment of major depressive disorders • Target symptoms: appetite/sleep disturbances, impaired concentration, fatigue, anhedonia (loss of pleasure) • Deficiency in monoamine; serotonin, nor epinephrine

ANTIDEPRESSANTS: POSSIBLE EFFECTS OF RECEPTOR BINDING
 • MAO (monoamine oxidase) enzyme")
Major classes • Tricyclic antidepressants; TCA (Elavil, Tofranil, pamelor) • MAO (monoamine oxidase) enzyme inhibitors • Selective Serotonin Reuptake Inhibitors (Prozac, Zoloft, Paxil, Celexa, Lexapro)
 Venlafaxine (Effexor) Duloxetine (Cymbalta)")
Antidepressant Drugs • Newer antidepressants – Serotonin-norepinephrine reuptake inhibitor (SNRIs) Venlafaxine (Effexor) Duloxetine (Cymbalta) Mirtazapine (Remeron) Trazodone (Desyrel) – Dopamine-norepinephrine reuptake inhibitor Bupropion (Wellbutrin/Zyban)
 • Start low, go slow • Sedation")
Tricyclic Antidepressants • First Antidepressants (Tofranil, Elavil) • Start low, go slow • Sedation Causes Improved Sleep Patterns. Take med at night • Antidepressant Effect Seen In Four To Six Weeks • Also Used For Panic Disorder, Obsessive Compulsive Disorder and Psychotic Depression

Side Effects of TCA drugs • • • Blurred Vision Dry Mouth Rapid Heart Rate Constipation Urinary Retention • • • Weight Gain Sedation Hypotension Postural Hypotension Dizziness

Selective Serotonin Reuptake Inhibitors • Excellent Antidepressant Effect • First Line Medications For Depressed Individuals • More Expensive • Prozac, Zoloft, Lexapro, Paxil

SSRI’s • Valuable In Treating Other Conditions • Effective In Two – Four Weeks • Serotonergic Syndrome: Rare and Serious Interaction Usually With MAOI

Side Effects • SSRI’S ARE THE BEST TOLERATED ANTIDEPRESSANTS, but MAY CAUSE: – Anxiety, agitation – Headaches – Gastrointestinal (N/V/D) – Sexual dysfunction – Serotonergic Syndrome

Monoamine Oxidase Inhibitors • Tried When Tricyclics And SSRI’s Fail • Treat Panic Disorder, Anxiety Disorders And Bulimia • Effective In 3 -4 Weeks
 Decongestants")
Serious Drug Interactions with MAOI’s • • Other Antidepressants Narcotic Analgesics (Especially Demerol) Decongestants and Cold Medicines May Cause Hypertension, Fever, Coma, and Even Death

Serious Food Interactions with MAOI’s • Foods Containing Tyramines (More Than 25 Mg / Serving • Sharp Cheddar Cheese • Salami • Sauerkraut • Beer and Wine (with yeast) • Ripe Avocados

Antianxiety/anxiolytic • Neurotransmitter GABA has inhibitory effect on neurons in parts of the brain • Drugs that enhance this effect exert a sedative hypnotic action • Benzodiazepines – Useful for short treatment, – Dependence, tolerance can develop

Side Effects • • Decreased Heart Rate Hypotension Dizziness/Syncope Anticholinergic Symptoms Central Nervous System Symptoms Sexual Dysfunction Weight Gain

NON-BENZODIAZEPINE ANTIANXIETY AGENTS • Buspirone Hydrochloride Buspar – Alleviates anxiety. Less sedating than the benzodiazepines. Does not appear to produce physical or psychological dependence. Requires 3 weeks or more to be effective. Good for GAD.

ACTION OF BUSPIRONE

Panic Disorder • SSRI’s are first line drugs for the treatment of panic disorder • Paroxetine, sertaline • Non addicting, relatively low incidence of unpleasant side effects 65
 • • Sertraline Zoloft Fluoxetine Prozac Paroxetine Paxil Fluvoxamine")
SSRI’S (SELECTIVE SEROTONIN REUPTAKE INHIBITORS) • • Sertraline Zoloft Fluoxetine Prozac Paroxetine Paxil Fluvoxamine Luvox – Used to treat OCD, panic, agoraphobia, generalized anxiety disorder. Effective with mixed anxiety and depression

BETA BLOCKERS • Propranolol Inderal – For Performance Anxiety • “Speaker secret”

Drugs For Treating Sleep Disorders • Most Commonly Benzodiazepines • Buspirone, Antidepressants, Beta Blockers • Antihistamines, Barbiturates, Antipsychotics • Illegally Obtained Drugs • Alcohol

Interactions And Side Effects • • • Alcohol Is Addictive With Sedative Effects Can Be Fatal Main Side Effect Is Sedation Occasionally Amnesia May Cause Physical Dependence

Drugs Used To Treat Substance Abuse and Dependency • Methadone- Oral Methadone Substituted For Heroine Injection • Disulfiram- Causes Extreme Discomfort When Alcohol Ingested • Nicotine Replacement • Opioid Receptor antagonist (Nalaxone Reverses Symptoms Of Narcotic Overdose)

ADHD Attention Deficit hyperactivity disorder • Stimulant Drugs – Adderal and Ritalin – May Be Useful As Antidepressants – Useful In Narcolepsy and ADD – Long Term Administration To Children Has Caused Controversy

Alzheimers Disease • For Alzheimer's disease • Anticholinesterase drugs showing some efficacy in slowing the rate of memory loss – Tacrine (Cognex) – Donepezil (Aricept) Memantine (Namenda)

Herbal Medicine • Major concerns – Potential long-term effects Nerve damage Kidney damage Liver damage – Possibility of adverse chemical reactions With other substances With conventional medications

Pharmacogenetics Differences in drug responses among ethnic groups • Lithium – Greater toxicity in African Americans than in whites • Haloperidol – Same dose, but plasma concentrations 50% higher in Asian group than in caucasion • Clozapine – Life-threatening side effect, agranulocytosis, more prevalent in Ashkenazi Jews than in other ethnic groups

HPA axis

Function of Cerebral Cortex
- Slides: 76