Understanding Evidence Based Practice From Research to Practice

Understanding Evidence Based Practice: From Research to Practice Marquetta Flaugher, Ph. D, ARNP-BC April, 2015

“In a service profession like nursing, research without practice is sterile and irrelevant, practice without research is ritualistic and intellectually empty” Sanil Varghese, 2013

Question: You have a patient experiencing a new c/o back pain described as muscular in nature (he just started rehab therapies). He asks if he can have a hot or cold pack to use. Which would you recommend?

Answer to Question Hot vs Cold Pacs

Question: You are asked by a family member if cognitive behavioral therapy is good to treat patients who suffer from PTSD. What do you say…is your recommendation Evidenced Based?

Answer to Question Use of CBT in treatment of PTSD

Objectives: At the end of this presentation, attendees will be able to: --define and differentiate evidence based practice (EBP) and nursing research -- describe ways to incorporate EBP and research into clinical practice --analyze the importance of EBP and research in clinical practice settings

Health spending is projected to grow at an average rate of 5. 8% from 2012 -2022 http: //www. cms. gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and -Reports/National. Health. Expend. Data/downloads/proj 2012. pdf

It is projected the United States will spend $5 Trillion in Health care spending by 2022 Forbes, 2015

Approval of thrombolytics for MI patients Male vs. Females?

Examples • Fewer than half of adults >50 years of age received recommended screening tests for colorectal cancer. • Inadequate care after a heart attack results in 18, 000 unnecessary deaths per year. • 40% of US people (2 million between ages 5785) were informed by their pharmacist the drugs that were prescribed could cause an interaction American Cancer Society 2014, IOM 2003, Drug. Watch, 2015

IOM Vision for the Future Be full partners, with physicians and other health care professionals, in redesigning health care in the United States

AHRQ's mission includes both translating research findings and providing health care leaders and policymakers with information to make critical decisions about health care. As healthcare leaders, nurses can use the translated research to improve health outcomes for our patients.

Why is EBP and Research Important to Nurses? "No man, not even a doctor, ever gives any other definition of what a nurse should be than this-'devoted and obedient'. This definition would do just as well for a porter. It might even do for a horse. It would not do for a policeman. " Florence Nightingale, 1860

Healthcare System in the U. S. • • Private not-for-profit Private for profit Public Third party reimbursement (private, governmental) • Uninsured • Veteran Healthcare • CMS (Medicare reimbursement)

How Do We Know What We Know? • • • Personal experiences Peers What we were taught in nursing school Conferences/In-services Policies and Procedures AND what we learn from our patients

Why be interested in EBP and Research? • Need for up-to-date information • Remove the disparity between clinical practice and current knowledge • Validate or change current practice • Generate new findings to improve practice
")
What are Differences and Similarities with EBP and Research? (What about QI? )

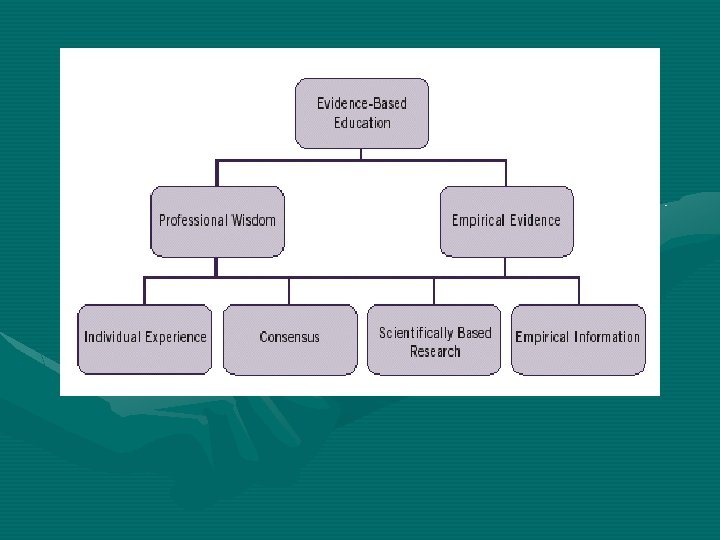
EBP “The conscientious and judicious use of current best evidence to guide health care decisions for improving patient outcomes” Titler, 2006

EBP a collaborative process using scientific evidence, patient preference, and practitioner experience integrated with clinical decision making to improve patient care, processes, and outcomes Newhouse, Dearholt, Poe, Puch & White, 2007 a paradigm and life-long problem solving approach to clinical decision making involving conscientious use of best evidence with one’s own clinical expertise, patient values, and preferences to improve outcomes for individuals, groups, communities, and systems Melnyk & Fineout-Overholt, 2011

The Purpose of EBP • • • Translate research into practice Increase the effectiveness of treatment Encourage some consistency in practice Utilize interdisciplinary approaches Encourage practice that is not based on tradition
 • Level I: Evidence obtained from")
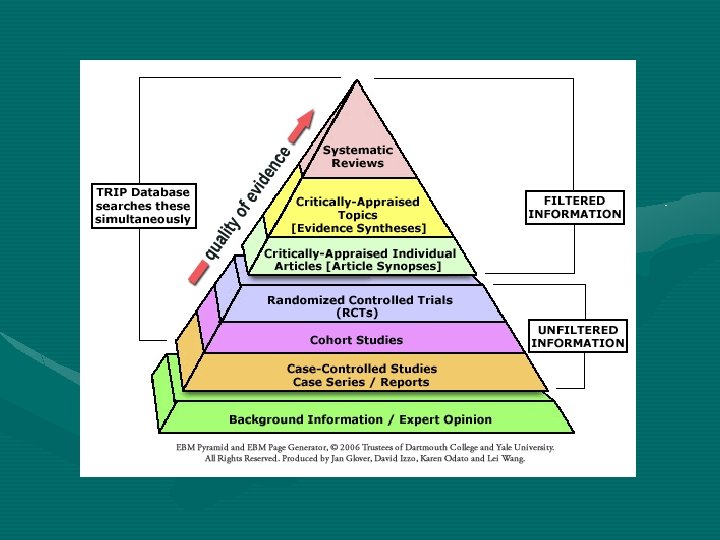
Grading EBP (U. S. Preventive Services Task Force) • Level I: Evidence obtained from at least 1 properly designed randomized controlled trial • Level II-1: Evidence obtained from well designed controlled trials without randomization • Level II-2: Evidence obtained from well designed cohort or case control analytic studies, preferably from more than one center or research group • Level II-3: Evidence obtained from multiple time series with or without the intervention. • Level III: Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees.
 • Level A: Good scientific evidence suggests")
Grading EBP (US Preventive Service Task Force) • Level A: Good scientific evidence suggests that the benefits of the clinical service substantially outweighs the potential risks. Clinicians should discuss the service with eligible patients. • Level B: At least fair scientific evidence suggest that the benefits of the clinical service outweighs the potential risks. Clinicians should discuss the service with eligible patients. • Level C: At least fair scientific evidence suggests that there are benefits provided by the clinical service, but the balance between benefits and risks are too close for making general recommendations. Clinicians need not offer it unless there are individual consideration. • Level D: At least fair scientific evidence suggests that the risks of the clinical service outweighs potential benefits. Clinicians should not routinely offer the service to asymptomatic patients. • Level I: Scientific evidence is lacking, of poor quality, or conflicting, such that the risk versus benefit balance cannot be assessed. Clinicians should help patients understand the uncertainty surrounding the clinical service.
 • Patient Population – who will be studied or benefit from the proposed")
PICO(T) • Patient Population – who will be studied or benefit from the proposed change • Intervention of Interest- what are you interested in looking at or learning more about • Comparison intervention or statuswhat proposed change will the intervention have • Outcome- what was the results; should the intervention be maintained or

Example of PICOT • Population: Study Geriatric patients with functional deficits • Intervention: Employ Restorative Program once patients have completed KT/PT program • Compare: Are other programs being utilized and how do they compare to a restorative program • Outcome: Was a difference noted or did the intervention (restorative program) enhance the functional ability of the geriatric patient compared to normal treatment • Time: May, 2015 to August, 2015

Steps to EBP • • • Select a topic to be studied Critique current evidence Adapt the evidence into practice (if needed) • Implement the EBP • Evaluate the outcome (either on patient or process)

Research Definition • Systematic inquiry that uses disciplined methods to answer questions or solve problems. • Generates new knowledge or validates knowledge. • Generalizable.

Differences: EBP • Interventions are stricter and more prescriptive than QI protocols but not as strict as research • Data collection may not be rapid and involves varying resources

Differences: Research • Has tight controls for extraneous variables to provide confidence that outcomes occur as a result of defined intervention and not chance • Not rapid and involves the use of resources that may vary according to scope of the study

Quality Improvement Definition • To improve internal processes and practices within a specific patient group or organization.
 • • • Protocols less formal; less rigorous Data collection")
Differences: Quality Improvement (QI) • • • Protocols less formal; less rigorous Data collection usually rapid Involves minimal time and resources

QI Method Sample Organizational analysis Unit level EBP Research Level of Evidence Qualitative, Quantitative Patient Population Generalizable Human Subjects - No IRB Data Collection Evaluation Purpose No Results Improve process Impact Implications Change Process Change Practice Dissemination Unit/Agency YES Search & Appraise Validity Add to body of knowledge Understanding change Practice Standards Scientific Community

When Should Research & EBP be Utilized? NOW Nursing requires the use of research to identify gaps in evidence for practice. American Nurses Association, 2011

Barriers to Healthcare Providers Utilizing EBP • • Time Money Too Much Reading Don’t Understand Research Don’t Know Where to Go to Find EBP Articles Not Interested Not having proper skills Thinking Researchers are not Directly Involved with Patient Care • No organizational support

Barriers to Research • • • Knowledge Too many and too few EBPs Attitude barriers Practice Barriers Few Incentives to Change Cost Higa and Chorpeta

Research Misperceptions • Nurses don’t feel comfortable performing research • IRB forms long and tedious • Nothing changes once research is completed

Change Can Be Messy

Research Methods Used • • • Descriptive cross-sectional designs Qualitative methods Randomized designs Case reports Partnership models

Translational Research: Two Areas of Translation • Process of applying discoveries generated during research in the laboratory, and in preclinical studies, to the development of trials and studies in humans. • Enhancing the adoption of best practices in the community. Costeffectiveness of prevention and treatment strategies is also an important part of translational science. NIH, 2011
 Special Category: How many scientists does")
From Phil Lee (p. lee#No. Spam. barnsley. org) Special Category: How many scientists does it take to screw in a lightbulb Q: How many scientists does it take to change a light bulb? A: The current theory is one but new theories are being put forward all the time and with experimentation the old theory may be discredited.
? The conduct and synthesis of research comparing the")
What is Comparative Effectiveness Research (CER)? The conduct and synthesis of research comparing the benefits and harms of different interventions and strategies to prevent, diagnose, treat and monitor health conditions, as well as the delivery of health care in “real world” settings.
? Research to improve health outcomes by developing and")
What is Patient-Centered Outcomes Research (PCOR)? Research to improve health outcomes by developing and disseminating evidence-based information to patients, clinicians, and other decision-makers, responding to their expressed needs, about which clinical and health system design interventions are most effective for which patients under

• • • • Databases to Identify Evidence CINAHL Medline National Guidelines Clearinghouse (AHRQ) Cochrane Library Organizational Guidelines The Janet Doe Lectures Joanna Briggs Institute U. S. Preventative Taskforce http: //healthlinks. washington. edu/clinical/guidelines www. hml. org/WWW/ebpws. html Up-to-Date Summaries (Expert Opinion) Research by Businesses, Pharmaceutical Companies

Funding Agencies in the U. S. Translation Science • Agency for Healthcare Research and Quality • Veterans Health Administration is the largest healthcare delivery system in the U. S. • CMS • RWJ • NIH (fairly new area)

Evaluate the Organization • Does it support a culture of inquiry? - Journal clubs - Adoption of EBP model - Research mentors & champions - EBP education in nursing schools or graduate residencies - Organization recognizes EBP projects - EBP/Research Nursing Councils

Evaluate Yourself • Did you ask the right question? Was it clearly defined? • Evaluate your ability to search for EBP articles • Evaluate your ability to critique articles • Evaluate how the intervention or change was implemented? Did it go smoothly? (Change often doesn’t) • Evaluate yourself as a teacher to others re: EBP • Evaluate your performance in continuing professional development

Ways to Incorporate EBP and Research in the “Real World” • • “Do it” “Use it” “Replicate it” “Evaluate it” • Did it change behavior? • Did it have an impact of practice? • Did it have an impact on pt care and/or pt satisfaction?

Resources to Facilitate EBP • • Journal Clubs Systematic Reviews Evidence Based Practice Guidelines Conducting Clinical Research

Core Competencies for Health Professions • • • Provide patient centered care Work in interdisciplinary teams Employ EBP Apply QI Utilize Informatics IOM Health Professions Education, 2003

FROM TRANSLATION TO DISSEMINATION TO DIFFUSION

Question: Why do nurses choose certain interventions for reducing risk or treating pressure ulcers? What are these interventions? How is the choice of intervention decided upon?

Case Study 1 What interventions are best in preventing or treating pressure ulcers in patients?
 Pressure relieving overlays on operating")
Ulcers Beneficial: Foam Alternatives (compared with standard foam mattresses) Pressure relieving overlays on operating tables Likely to be Beneficial: Low Air Loss beds and Medical Sheepskin Overlays (compared with standard care) Unknown Effectiveness: Alternating Pressure Surfaces, Different Seat Cushions, Electric Profiling Beds **Repositioning, & Topical lotions and dressings Likely to be Ineffective or Harmful: Air filled vinyl boots with foot cradle & low air

What does AHRQ say about PREVENTION of Pressure Ulcers? A=good evidence & support B=fair evidence to support recommendation C=recommendation based on expert opinion and panel consensus. Routine skin inspections: C Using hot water and mild soap: C Using Moisturizers: C Avoid massaging bony prominence: B Frequent repositioning: B Positioning Devices such as Pillows: C Pressure Reducing Devices for Chairs: C

Case Study 2 What are the best screening techniques for colorectal cancer?
 Colonoscopy every 5 years starting at age 40 or")
Beneficial: Fecal immunochemical test (FIT) Colonoscopy every 5 years starting at age 40 or ten years earlier than age of youngest affected relative at time of diagnosis Likely to be Beneficial: Flexible Sigmoidoscopy —followed by Colonoscopy if Sigmoid is positive Unknown Effectiveness: Double contrast Ba Enema **FOBT and CT colongraphy only when patient declines colonoscopy or has uncomplicated colonoscopies National Guidelines Clearinghouse, 2013

Case Study 3 A patient has a grand mal seizure. He has no prior hx of seizures, and no head trauma. He drank ETOH once or twice a week and had not had ETOH on the day of the seizure. PE is Negative. The pt is given a loading dose of Phenytoin IV and the drug is continued orally. A CT head is normal. EEG shows only nonspecific findings. The pt asks what is his risk of recurrence of seizures.
,")
After a Literature Search on Grateful Med ($2. 68 and one half hour later), the clinical evidence demonstrates the risk of recurrence at one year is between 30 -43%. After a seizure free period of 18 months, the risk of recurrence would be under 20%. The patient now leaves with a clear idea of his prognosis.

Summary: Outcomes of EBP & Research • • • Improved Patient Outcomes Personal Growth & Satisfaction Loss of “Sacred Cow” & “GOBSAT” Organizational support Generating new Knowledge or Validating Existing Knowledge

• • • Summary: How Do We Incorporate EBP and Research into Practice? ? ? Journal Clubs SOC review of Policies & Procedures Communication Mass Media Opinion Leaders: Change Champions Educational Support

Summary: Changing the Infrastructure of Your Facility • Organizational Support • Changing culture – Vision toward Excellence • Teamwork – staff participation • Synthesizing/Implementation • Communication of Findings • Internships/Mentorships

Summary: How Can We Sustain EBP & Research? • Ensure results are reported to staff • Summarize interventions into policies, procedures, guidelines, and competencies • Incorporate change into unit orientation programs • Disseminate results at unit & departmental educational forums • Report results at performance improvement councils and/or committee meetings

Research & EBP Every time you utilize findings of completed research to change or validate your practice this is EBP. These two concepts are not interchangeable but are directly related.

Closing Thoughts: Nurses Transform Healthcare

Questions? Thanks for your attention and enjoy your conference.
- Slides: 79