Understanding and Living Well with Chronic Pain Pierre





































 • NSAID (Ibuprofen/Advil) • Narcotics/Opioids")



























. Assessment and management of chronic")
- Slides: 68
Understanding and Living Well with Chronic Pain Pierre Morin, MD, Ph. D
Basel
Medical Models • • • Bio-medical model Social determinant model Bio-psycho-social model Psychodynamic model Positive psychology (Seligman), Positive health model (Antonovsky) • Indigenous model • Recovery/Self-management model • Process model (Mindell)
Bio-medical model Environment • • • Biologic predisposition Psychology Disease Clinical Outcome Illness • • Characteristics: unilinear; disease fully explains the illness; biological determinants are both necessary and sufficient for disease its diagnosis and cure; psychology may be a secondary influencing factor. There is no explanation for illness without disease.
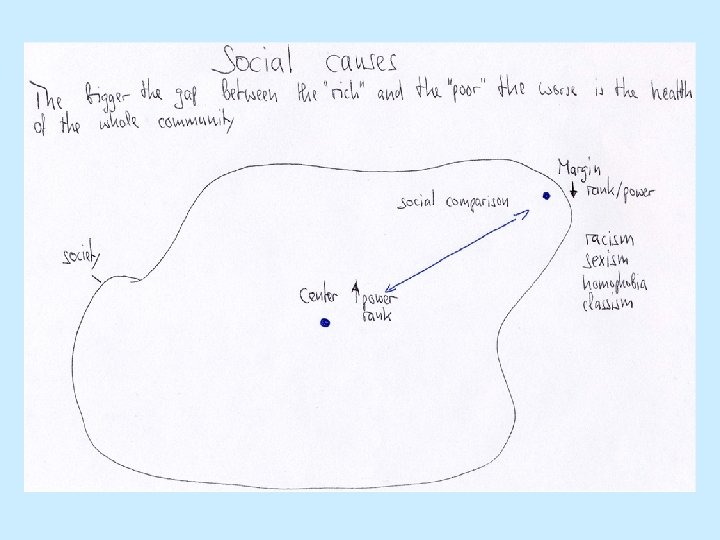
Social determinant model Diseases are influenced and caused by social processes: Social status, Rank, Social dynamics of prejudice and marginalization based on gender, race, sexual orientation etc… create ongoing stress which cause disease.
Bio-psycho-social model • • Environment Psychosocial modifiers Biologic/ predisposition Disease Clinical Outcome Psychological Illness • Illness and disease result from simultaneously interacting systems at the cellular, tissue, organ, and interpersonal and environmental levels
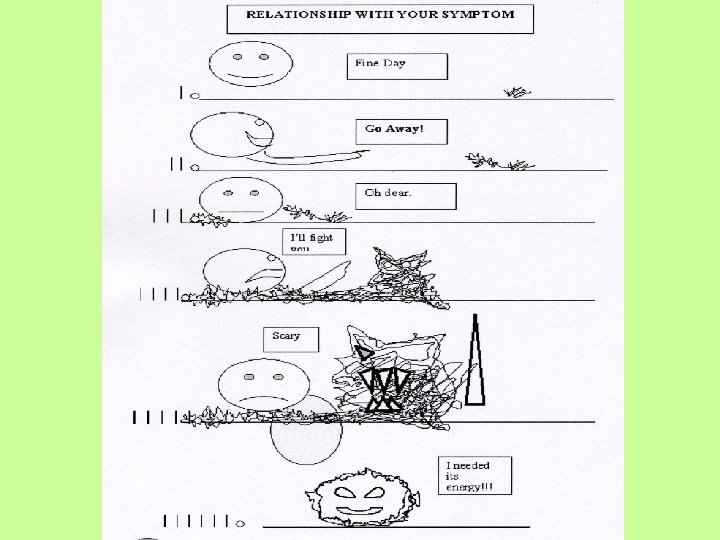
Psychodynamic model Illness and disease have an adaptive function. They are meaningful processes that are embedded in a person’s individual and collective life and environment. They are the best solution so far and promote healing and growth. Physiologic states are metaphors for individual and social processes.
Positive psychology/ Positive health model What prevents us from getting ill physically and mentally? What are the characteristics of people who stay healthy despite adverse circumstances? What are the strengths and virtues that act as buffers against illness? How do we amplify and foster these strengths and virtues? Instead of focusing on curing/treating pathologies positive psychology/health sees health as a continuum and is interested in the factors (resilience, sense of coherence, meaningfulness) that give our lives purpose, allow us to stay healthy and cope with our limited health.
Indigenous model • Relationship to Nature, the ancestors, the spirit world is relevant for staying healthy. • Relationship dynamics are a relevant factor for causing disease: jealousy, the evil eye, being “outcasted” by the tribe etc…
Recovery/Self-Management Model I Recovery is an individual’s journey of healing and transformation to live a meaningful life in a community of his or her choice while striving to achieve maximum human potential.
Recovery/Self-Management Model II • Clients have primary control over decisions • Based on concepts of strength and empowerment • Provide education • Living with Symptoms instead of getting rid of them • A meaningful life is possible despite serious/chronic symptoms • Adaptation to issues of diversity
Recovery/Self-Management Model III • Increasing knowledge about illness • Engaging in activities that promote health • Coping more effectively and reducing distress from symptoms • Reducing social exclusion • Increasing self-confidence
Process Model of Medicine • Procrustes and his bed: ignoring/marginalizing dreamlike and creative qualities of life allows us to create a consensual everyday reality and function in life. Marginalized realities reappear imbedded in things we call problems and symptoms.
Pain
Pain/Chronic Pain Definition • An unpleasant sensation and an emotional experience associated with a real or potential damage to tissue, or the equivalent of such damage. • Pain without apparent biological value that has persisted beyond the normal tissue healing time (usually taken to be 3 months)
Names Amplified Musculoskeletal Pain, Reflex Neurovascular Dystrophy, Reflex Sympathetic Dystrophy, Sympathetically Maintained Pain, Fibromyalgia, Algodystrophy, Complex Regional Pain Syndrome Types I and II, Causalgia, Sudeck’s Atrophy, Shoulder-Hand Syndrome, Repetitive Strain Injury, Plantar Fasciitis, Localized or Diffuse Idiopathic Musculoskeletal Pain, Neuropathic Pain, Central Pain, Psychogenic Pain, Psychosomatic Pain
Epidemiology/Prevalence/Impact • 9 - 11% of the U. S. population suffer from moderate to severe chronic pain. • Women are more likely to suffer chronic pain than men. • On average it is present almost 6 days in a typical week. • Only ½ of chronic pain sufferers say their pain is pretty much under control. • Chronic pain is the most common complaint made by patients to their Primary Care Providers. • It accounts for an estimated $75 -$100 billion a year in the U. S. in lost productivity and health care costs.
Specificity Theory of Pain: • The intensity of pain is directly related to the amount of associated tissue injury. For instance, pricking one’s finger with a needle produces minimal pain, whereas cutting one’s hand with a knife causes more tissue injury and is more painful. This theory is generally accurate when applied to certain types of injuries and the acute pain associated with them. It is inadequate to explain chronic pain.
Gate Control Theory: • Perception of physical pain is not a direct result of activation of pain receptor neurons, but instead is modulated by interaction between different neurons. Before they can reach the brain pain messages encounter “nerve gates” in the spinal cord that open or close depending upon a number of factors (possibly including instructions coming down from the brain). When the gates are opening, pain messages “get through” more or less easily and pain can be intense. When the gates close, pain messages are prevented from reaching the brain and may not even be experienced.
Loesser’s Onion Theory of Pain: • This says that the pain mechanism is a series of nested layers, like the ones of an onion. The nerve stimulus or damage is at the centre, the next layer is the perception of pain, then come suffering, pain behavior, and finally interaction with the environment.
Nociceptive Pain: • Pain that is a result of tissue irritation, impending injury, or actual tissue injury sensed by pain receptors. Pain receptors are the nerves which sense and respond to parts of the body which suffer from damage. When activated, they transmit pain signals (via the peripheral nerves as well as the spinal cord) to the brain. The pain is typically well localized, constant, and often with an aching or throbbing quality. Visceral pain is the subtype of nociceptive pain that involves the internal organs. It tends to be episodic and poorly localized.
Neuropathic Pain: • Can occur as a result of injury or disease to the nerve tissue itself. This can disrupt the ability of the sensory nerves to transmit correct information to the thalamus, and hence the brain interprets painful stimuli even though there is no obvious or known physiologic cause for the pain. Neuropathic pain is the disease of pain. It is not the sole definition for chronic pain, but does meet its criteria.
Referred Pain: • Is a phenomenon used to describe pain perceived at a site adjacent to or at a distance from the site of an injury's origin. One of the best examples of this is during heart attack. Even though the heart is directly affected the pain is often felt in the neck, shoulders and back rather than the chest.
Sympathetically Maintained Pain: • This condition used to be called a reflex sympathetic dystrophy. It is also known as algodystrophy, Sudeck’s atrophy and a host of other names. It is now called, by the International Association for the Study of Pain, a “complex regional pain syndrome”. Sympathetically maintained pain is believed to be maintained by the sympathetic nervous system or by circulating catecholamine.
Peripheral and Central Sensitization: • Amplification of pain stimuli produces secondary heightened sensitivity.
Hyperalgesia: • Lowered pain threshold, which in one form is caused by damage to pain receptors in the body's soft tissues. Conditioning studies have established that it is possible to experience a learned hyperalgesia.
Allodynia: • Meaning "other pain", is the perception of pain caused by usually nonpainful stimuli, such as touch or vibration. An example of allodynia is when a person perceives light pressure or the movement of clothes over the skin as painful, whereas a healthy individual will not feel pain. Several studies suggest that injury to the spinal cord might lead to loss and re-distribution of pain receptors and pain modulating neurons leading to the new response.
Pain and Memory: • Conditioning and sensitization can be seen as a learning process at different levels. In addition, memory traces of pain get stuck in the brain’s prefrontal cortex which controls emotion and learning. Abnormal implicit memories of pain and emotional associations will influence associative learned behaviors, e. g. avoiding certain movements which will increase the chance to develop chronic pain.
Hebbian or Associative Learning • Any two cells or systems of cells that are repeatedly active at the same time will tend to become 'associated', so that activity in one facilitates activity in the other.
Long-term Potentiation • Long-lasting enhancement in communication between two neurons that results from stimulating them simultaneously. Since neurons communicate via chemical synapses, and because memories are believed to be stored within these synapses, LTP and its opposing process, long-term depression, are widely considered the major cellular mechanisms that underlie learning and memory.
Fear-Avoidance Model
Pain and Trauma/Abuse • Beliefs that trauma and pain are unpredictable and uncontrollable. • Sense of feeling victimized by pain. • Fears and avoidance of activities that will be painful. • Avoidance behaviors lead to inactivity that will worsen pain.
Regaining Ownership/Control • Chronic pain as a trauma that needs to be re-conquered. • Integrating “Painmaker” and “Traumatizer” • Like Native Americans used to inflict themselves with a wound once they had been wounded by an adversary.
Psychological Assessments • Pain Questionnaire/Inventory • Depression/Learned Helplessness • Anxiety Sensitivity (fear of anxiety-related bodily sensations) • • • Cognitive & Behavioral Avoidance Coping Styles Beliefs and Expectations Self-efficacy/Sense of Coherence PTSD Checklist/Abuse
DSM IV/Somatoform Disorder • Conversion disorder, hypochondriasis, body dysmorphic disorder, pain disorder, undifferentiated somatoform disorder, somatization disorder. • (Not factitious disorder, malingering).
Multidisciplinary Pain Treatment/Management • • Medication/Pharmacotherapy Physical Therapy, Occupational Therapy Psychology Retraining the Nervous System Alternative/Complementary Medicine Interventional Medicine Self-management/Education
Medication • Over the Counter Medication (Acetaminophen, Tylenol, Paracetamol) • NSAID (Ibuprofen/Advil) • Narcotics/Opioids (Morphine, Methadone, Oxycontin, Fentanyl) • N-Type Ca-Channel Blocker (Sea snail venom) • Na-Channel Blockers (Antikonvulsant) • Vanilloid/Capsaicin Receptor Blockers (Chili pepper) • Antidepressants
Interventional Pain Management • Nerve Blocks • Spinal Cord Stimulation • Implantable Opioid Pumps
Ramachandran/Phantom limb/Mirror box • A mirror box is a box with two mirrors in the center (one facing each way) to help alleviate pain. • The non-painful limb is projected onto the hurting side in order to retrain the brain, and thereby eliminate the learned paralysis/pain.
Retraining the Brain • Vigorous exercise and talk therapy are used to retrain patient’s brain to recognize pain signals differently.
Self-management • • Allopathic Medicine Complementary Medicine Allostasis/Stress-management/Relaxation Advocacy/Empowerment/Rank/Leadership Education/Behavioral changes Family/Peer/Community support Psychology/Picking up the energy (painmaker/traumatizer)
Hierarchy and Health • Marmot’s Whitehall Study of British Civil Servants • Hierarchy and Social Inequality leads to more illness and early death • Allostasis/Allostatic Load: The burden of cumulative adversity • Coping: Sense of Coherence
Health Disparity • Relative poverty • Disparity between the rich and the poor: High gap correlates with poor population health. • Social comparison: Feelings of humiliation, resignation and shame affect our stress physiologies.
Health Olympics/US Ranking • • • Life Expectancy: Teen Birth: Educational Opportunities: Child Poverty: Child Abuse Death Rates: Child Injury Death Rates: 29 28 21 25 26 23
Rank • Rank reflects the underlying power differences of the many hierarchies we use on a daily basis to compare ourselves (Fuller, 2003). • Conscious or unconscious, social or personal ability or power emerging from areas of sociocultural influence, personal psychology, and/or spiritual ties (Mindell, 1995).
Subjective Rank and Health
Rank Dimensions • Social Rank • Psychological Rank • Spiritual/Transpersonal Rank • Contextual Rank
Social Rank Depends on one’s position in regard to mainstream values in the areas of sociocultural influence like gender, sexual orientation, age, class, health/disability, religion, ethnic identity/race etc…
Psychological Rank Includes self-love, self-confidence and self -knowledge. It also stresses good relationships skills, high in-group status, and a loving support network.
Spiritual or Transpersonal Rank Reflects one’s sense of connectedness with something spiritual and divine or with something greater than yourself (e. g. God, Nature).
Contextual Rank Derives from one’s momentary roles in a given situation: as a teacher, health care provider, parent, bank teller etc. . .
Signals of the Clinicians’ Higher Rank An attitude of: • I know what is wrong with you! • You are sick, I am in good health! • I decide about the content, the setting and the course of our interaction or therapy! • I can be empathic! • I decide how much of myself I reveal in the relationship! • Detached and objective tone of voice, that reflect our sense of superiority, self-confidence, selfesteem.
Signals of the Clinicians’ Higher Rank • In our capacity to sit back and relax; feel at ease, comfortable and confident. • In our capacity to be verbally articulate and expressive. • In our feeling of entitlement. • When we marginalize or dismiss our patient’s thoughts and feelings, in comments like “don't take it so personally, ” “you are too sensitive”, etc. • When relationship issues arise and we think it is the patient’s problem. We can't understand. We think the patient is crazy, illogical, disturbed or angry.
Signals of the Patients’ Lesser Rank • A tendency to settle for the way things are. • Feeling cloudy and unable to think. • Self-doubt, blame and insecurity, low self-esteem and feeling of inferiority. • Adaptive behavior. • A tendency to placate, elevate, and compliment the other person. • Signals of fear, like shaking, sweating, not able to look the other in the eye. • Feelings of paranoia. • Body signals of agitation. • Feelings of revenge, jealousy, and anger. Tendency to be emotional, upset, angry, loud, to feel misunderstood, and to feel emotionally desperate.
Signals of the Patients’ Lesser Rank • Difficulty in taking a stand for oneself. • One feels overlooked, neglected and unnoticed. • One feels like one’s position is insignificant and no one else feels the same. • Little or no eye contact. • Shy or reserved. • Many pauses in the speech flow or not much talking at all. • Poor motivation and compliance. • Stubbornness or insistence on one’s position.
Circumstances with Innate Rank Issues • With women who feel underprivileged in their relationships. • With foreigners from underprivileged parts of the world. • With people with the sexual orientation of a minority. • With people with an obvious physical sign that characterizes them as belonging to a disenfranchised group of society (e. g. skin color, other physical stigmas) • With children and adolescents • With people suffering from chronic pain or other chronic health problems
Barriers to Effective Pain Management Patient Attitudes Clinician Attitudes Cultural/Societal Attitudes
Cultural and Personal Context of Chronic Pain • Pain as a sub-culture experience • Chronic pain patients feel marginalized from mainstream culture • Loss of social rank/status is a co-factor in chronic pain • Sense of feeling traumatized by pain; past history of abuse/trauma
Somebodies and Nobodies • Sense of being a nobody in social comparison to others • Loss of status/rank because of illness and other marginalizing processes • Sense of shame and humiliation, loss of respect and dignity • Independent of individual psychology • Power of internalized social values
Cultural Metaphors • Blameworthy ill-health versus responsible health • Health and illness as an individual process • Juvenile “good-looking” body equals success; metaphor fitness and attractiveness and standard for social acceptance and recognition • The body as a commodity
Biases and Stereotypes • Beliefs about addiction/”Opiophobia” • Beliefs about functional versus real disease • Beliefs about health and healing • Beliefs about how much pain is ok • Beliefs about other healing modalities • Beliefs about good patient and bad patient
Clinician-Patient Relationship • • • Cultural competence/sensitivity Rank awareness Awareness of one’s biases/stereotypes Communication skills Awareness of individual and social beliefs
Difficult/Complex Patient/Client • • • Hostile or defiant patient Demanding patient Patient with multiple chronic problems Patient who somatizes Patient with “functional”/ psychological overlay
Clinical Competency in Chronic Pain Treatment • • • Knowledge of systemic and social determinants. Knowledge of beliefs and barriers to treatment. Ability to mediate and facilitate complex issues. Works as part of a multidisciplinary team. Is an expert in communicative and interpersonal skills. • Educates and chares decision making.
REFERENCES • • Institute for Clinical Systems Improvement (ICSI). Assessment and management of chronic pain. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); 2005 Nov. 77 p. Assessment and Treatment of Chronic Pain: By John Mark Disorbio, Ed. D, Daniel Bruns, Psy. D, and Giancarlo Barolat, MD. Practical Pain Management, March 2006. Provider-Patient Interaction: Understanding Unconscious Interpersonal Defensive Responses in a Chronic Pain Practice to Improve Interactions. By Ron Lechnyr, Ph. D. , DSW; Terri Lechnyr, MSW, LCSW. Practical Pain Management, Mar/Apr 2004. Fuller, R. W. Somebodies and Nobodies. Overcoming the Abuse of Rank. Gabriola Island, BC: New Society Publishers, 2003. Mindell, A. Sitting in the Fire: Portland: Lao Tse Press, 1995. pierre@creativehealing. org www. creativehealing. org