Ultrasound Guided Peripheral Nerve Blocks for Chronic Pain

Ultrasound Guided Peripheral Nerve Blocks for Chronic Pain James Jarman FANZCA, FFPMANZCA, PG Cert US Anaesthetist and Pain Specialist Joondalup and SJOG Midland Hospitals, Perth

Ultrasound Learning Resources • YOUTUBE IS YOUR FRIEND! • Lots of great videos available on youtube • Sonosite have a great youtube channel • “Essential Anatomy” app – demonstration to follow

Ultrasound skills: • US blocks are composed of 2 skills o Identifying the nerves o Manipulating the needle • Identifying nerves: o KNOW YOUR ANATOMY o Practice scanning yourself o Nerves frequently run with arteries – look for an artery and nerve if often nearby- eg ilioinguinal, adductor canal, SSNB, popliteal tibial. o Nerves also tend to run in fascial planes – if you get your LA into the right plane it will usually work o Proximal nerves are mostly “nerve” (=fat=black) with little white connective tissue. As you move distally and branches are given off, nerves become a more speckled white colour due to higher proportion of connective tissue. Proximal nerves are more vulnerable to injury than distal nerves and blocks are associated with a higher risk of nerve injury o If unsure what you see is a nerve, scan proximally and distally- nerves will stay present, tendons and other things will tend to get bigger/ smaller/ disappear o If still unsure, stimulate the nerve eg 50 hz with RF needle (note RF needles can be very hard to see with US, especially for deep blocks
 brachial plexus (interscalene). Lots of dark nerve, little connective tissue Right: (Distal)")
Left: (Proximal) brachial plexus (interscalene). Lots of dark nerve, little connective tissue Right: (Distal) - Median nerve (M) in forearm. Little nerve, lots of white connective tissue

Ultrasound skills • Identifying nerves: Nerves vs vessels o Arteries and pulsatile and incompressible o Veins are non pulsatile and compressible o Nerves and not pulsatile or compressible o Can also use colour doppler (NB red vs blue is flow away/ towards transducer) • Needle manipulation: o can be practiced on gel phantoms or on chicken legs / breasts: can see nerves in them o PRACTICE!
 vs out of plane (RIGHT):")
Ultrasound technique • In plane (LEFT) vs out of plane (RIGHT):

In plane vs out of plane • In plane vs out of plane: • I do all my blocks in plane o o Allows you to see both the needle tip and the nerve and ensure no contact With out of plane run risk of spearing the nerve In plane does require more practice to perfect Of needle and ultrasound beam in same plane can see a “false” tip of the needle: giveaway in that will not see the whole needle shaft- if not seeing whole shaft likely that beams aren’t alligned • Only advance the needle when you can see the tip!

Technique: Hand-screenhands • Common problem with ultrasound beginners is “screen fixation”: leads to needle plane and probe plane diverging • Correct eye movements is hands-screen-hands-screen

Tips: Anisotropy Ulnar nerve at the forearm

Ultrasound and Anisotropy • Anisotropy: As transducer is tilted backwards and forwards nerve can come in or out of view • Most noticable anisotropy: popliteal sciatic nerve: o As tilt probe backwards and forwards nerve appears and disappears o For this block, aiming beam a little towards patients head helps

Needle insertion point: close and steep or far and shallow?

US technique: needle insertion point • Needle insertion site relative to probe: Close and steep vs far and shallow o Short needle inserted next to probe= Steep angle = poor needle view BUT needle easier to control o Long needle inserted further away from probe= shallow angle and better needle view but hard needle to steer: need to pull right back to skin then re-angle. Also allows free movement and rearrangement of probe without bumping into needle o I broadly tend to use close and steep for shallow blocks (1 -2 cm depth), an inbetween position for medium depth and far and shallow for deeper blocks (>5 cm)

Technique: Maximising screen real estate

Screen setup • I position target at the edge of the screen not the middle o Makes use of the whole screen o Can always move the probe further away from the needle to see the rest, but can’t move the probe closer to the needle if it’s hitting it! o Allow whole path of needle to be seen o Forces flatter needle trajectory meaning better visualisation

Equipment setup • Get rid of any air in the syringe / needle / line o Even a tiny amount to air will destroy the ultrasound image and make the block impossible

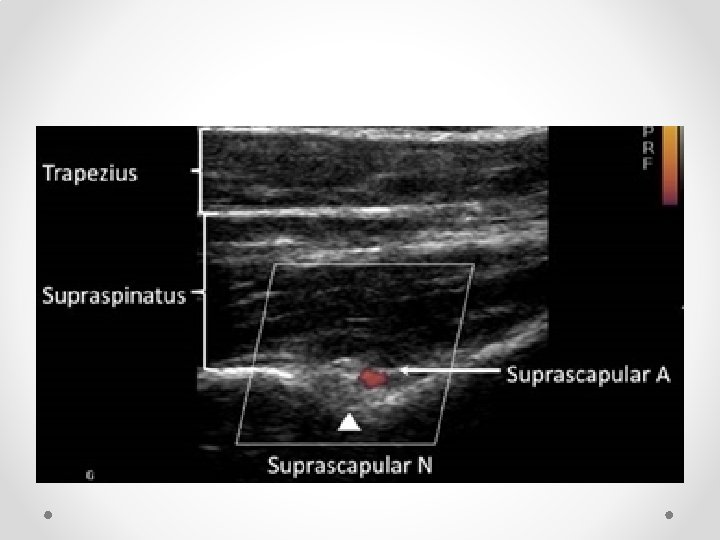
Can’t see needle? • Eg Suprascapular block on obese patient with RF needle • Try small boluses of saline / dilute local anaesthetic to visualise tip location

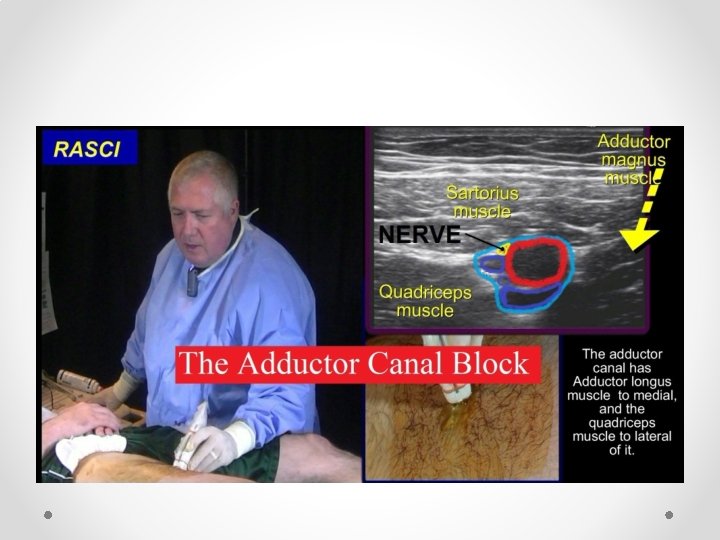
Saphenous block • Saphenous nerve supplies knee and strip of skin over medial calf • Recent cadaver studies suggest may also provide some innervation to medial ankle joint • Can be blocked at adductor canal in mid thigh (US), by SC infiltration at level of tibial plateau or distally at ankle


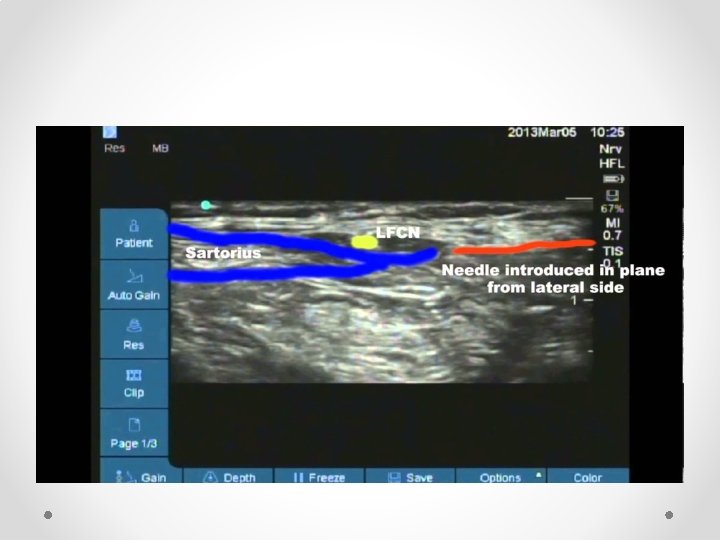
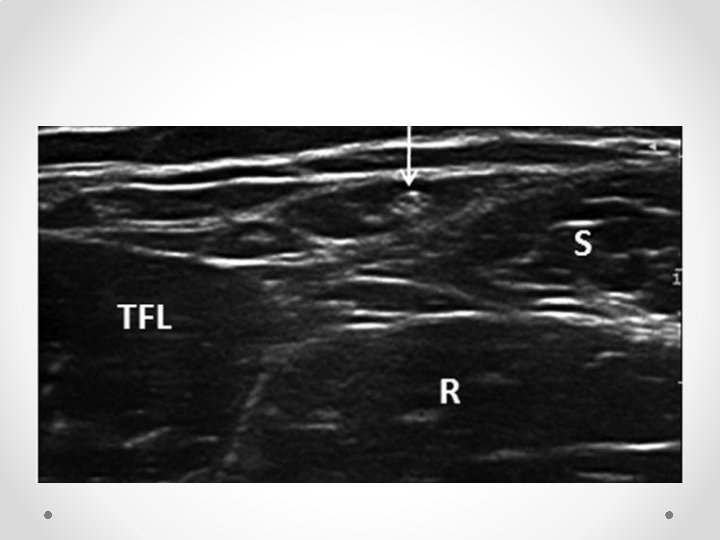
Needle entry from Anterior-Lateral

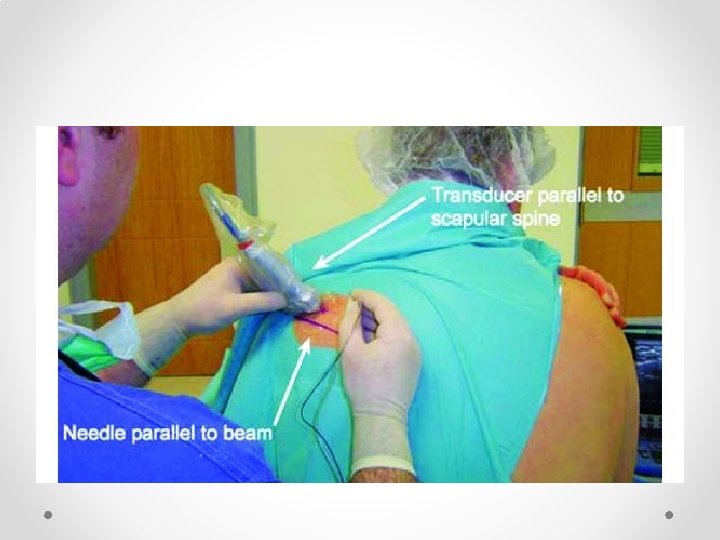
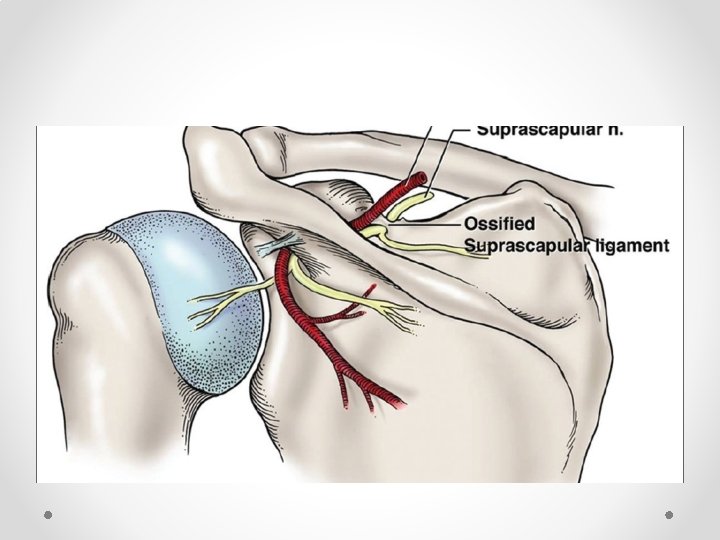
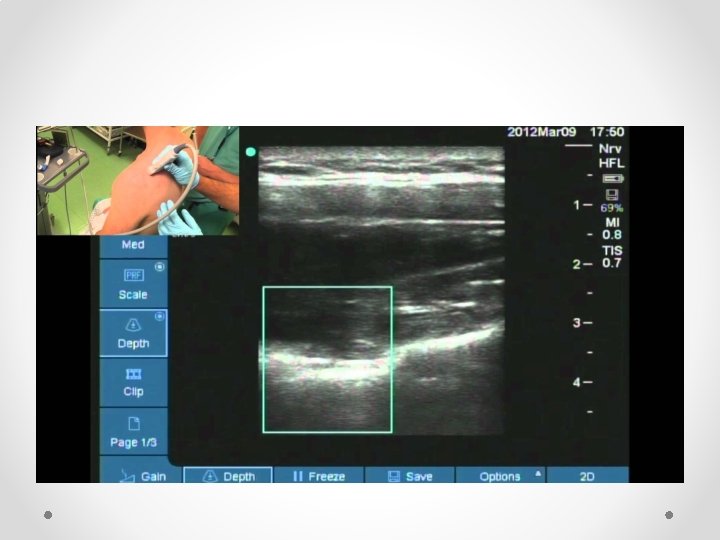
Suprascapular nerve block • So much easier than using II • Can add pulsed RF fairly easily, or thermal (eg in elderly who are not candidates for surgery) • Practical tips (just one way of doing it): o Sit patient in a chair (if not liable to faint). Can also be done prone. o Arm must be hanging by side: if arm is abducted acromion get in the way of the US probe o I use a 100 mm block needle with block or RF needle if using RF. RF is hard to see on US. If using RF seek out the stimulation o In some patients may need to angle the probe (heel-toe) laterally to peek under the bone o Make sure you are looking lateral enough: most common failure to see the dip and ligament in not being lateral enough o Nerve very hard to see, as is artery: if can get it under the ligament it will work o Seeing the ligament lift up is a very good sign

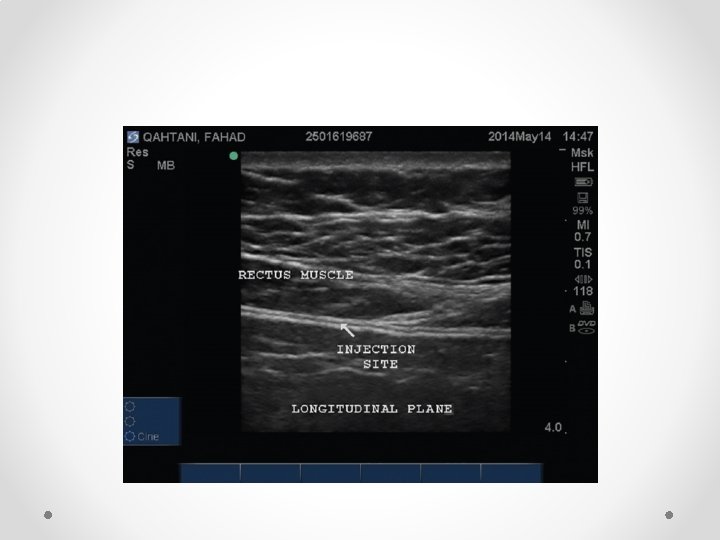
Rectus Sheath block for ACNES

Abdominal Cutaneous nerve entrapment syndrome • Estimated incidence of 1: 2000 or up to 25% of all undiagnosed chronic abdominal pain o o Van Assen, Brouns et al, Scan J Trauma 2015 Srinivasan R, Greenbaum et al, Am J Gastoent 2002; 97: 824 -30 • More common in women • Patients present with localised abdominal pain- can put their finger on the area of pain • Typically lies at lateral border of rectus muscle • May follow surgery / trauma – eg around laparoscopic port sites. • Worse on contracting abdominal muscles (Carnett sign) • Area of altered skin sensation around painful area (hyper/ hypoaesthesia) • RCT of 48 patients to lignocaine or saline injection showed 4/22 improved in saline group compared to 13/22 in lignocaine group at 2 week follow up o Boelens OBA British Journal of Surgery 2012; 99

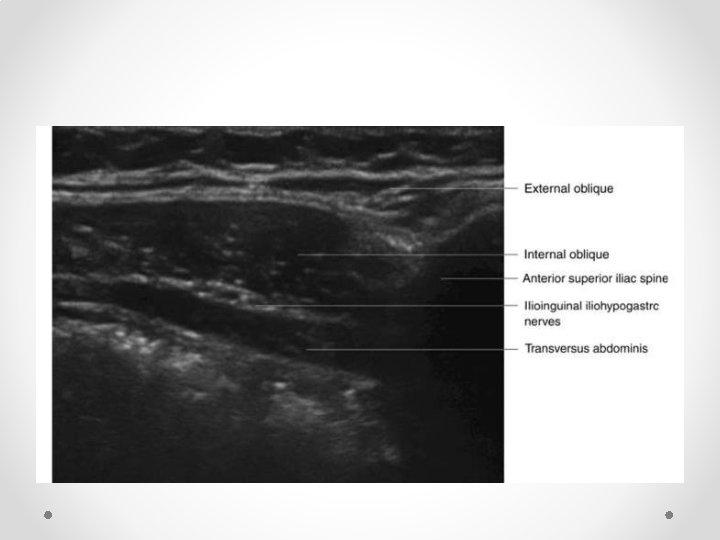
Nerves run between IOM and Transversus abdominus, then posterior to rectus muscle before perforating through it to skin
 and below arcuate line NB below arcuate line (5 -10 cm below")
Above (top) and below arcuate line NB below arcuate line (5 -10 cm below umbilicus) is no fascial sheath deep to rectus abdominus


Lateral Femoral Cutaneous nerve block


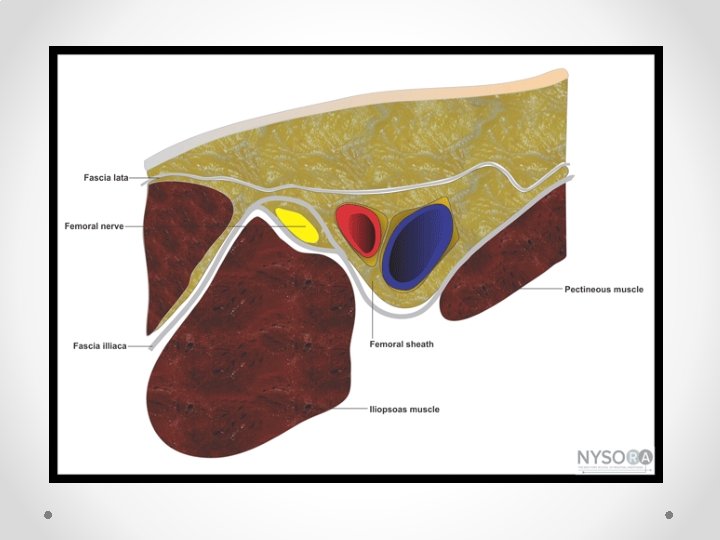
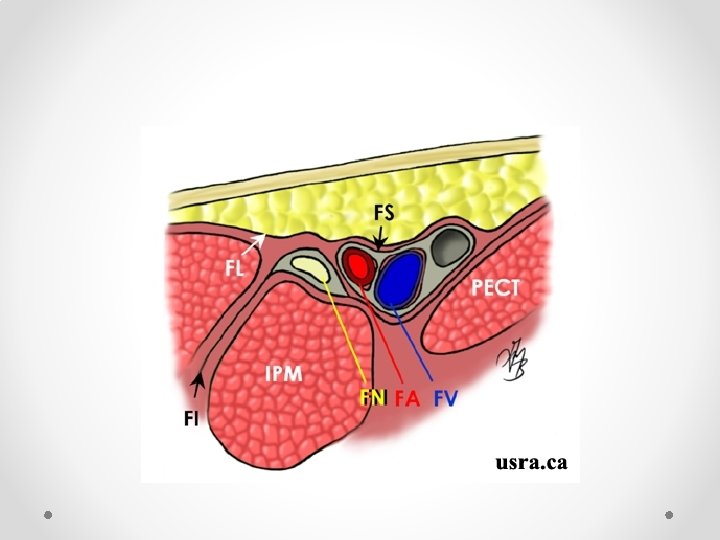
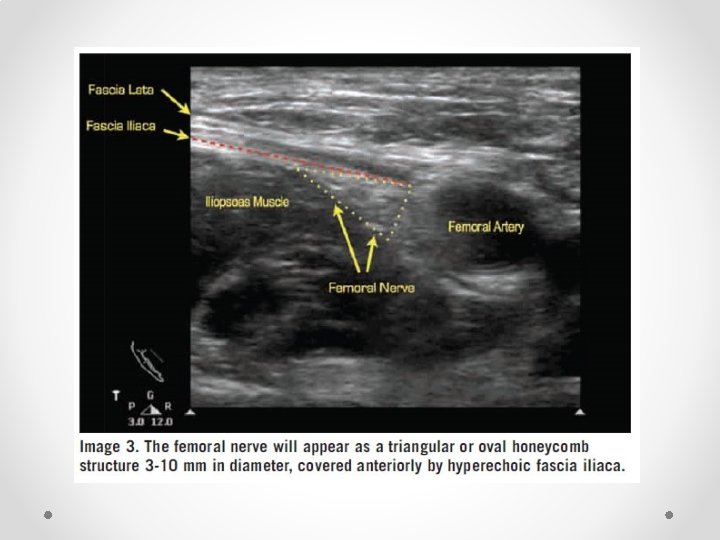
Femoral Nerve block • Not commonly done for chronic pain • Fairly well known block so only short mention of some reminders • Book first on list, use lignocaine as quads weakness means falls risk • Note fascial planes: o Nerve is NOT in same plane as femoral vessels o Nerve lies deep to fascia iliaca, while vessels lie superficial o Nerve is often difficult to see on ultrasound, while artery is easy to see • Therefore aim for needle tip to be lateral and deep relative to the artery to be in the correct plane

Ilioinguinal Block: US probe position

Ilioinguinal block


Block Safety • Data from anaesthetic literature demonstrates very good safety profile • Incidence of temporary nerve injury in region of 0. 1 -1% (more for proximal blocks and upper limb blocks). Small peripheral nerves (eg LFCN, ACNES) are particularly low risk • Incidence of permanent nerve injury (>6 months) approx 1: 10 000 • Seizures approx 1: 10 000

Summary • Ultrasound allows direct visualisation of target nerves, as well as of structures to avoid (eg vessels) • Peripheral blocks are a very low risk strategy which can sometimes pay off with significant results • Particularly useful in patients who can not tolerate medications (eg elderly).
- Slides: 49