Ultrasound Guided Central Venous Cannulation CVC Shirley Lee
 Shirley Lee MD CAEP 2008")


























- Slides: 29
Ultrasound Guided Central Venous Cannulation (CVC) Shirley Lee MD CAEP 2008
Why Ultrasound guidance? • Traditionally, CVC mechanical complications occur up to 15% • Insertion unsuccessful up to 12% • Becoming standard of care Mc. Gee and Gould, NEJM 2003; 348: 1123 -1133 Merrer, De Johnghe, Golliot, et al. JAMA. 286: 700 -7, 2001
CVC Complications • Pneumothorax, arterial puncture, hematoma, malposition, increased skin punctures with bleeding complications, delay and failure to catheterize, thoracic duct injury (left sided approach), air embolism, arrhythmias, and death • Delayed complications: infection and thrombosis
Advantages • Safer • Markedly decreased pneumothorax rate • Real-time visualization of target • See needle enter target vein, avoiding adjacent arteries, nerves
Evidence • In ER: Prospective, randomized trial of 130 patients • Complication rate: 4. 6% vs. 16. 9% • Success rate: 93. 9% vs. 78. 5% • Time not significantly different Leung, Duffy, Finckh. Ann Emerg Med 2006; 48(5): 540 -7
Evidence • ICU – Prospective, randomized trial of 900 • Success: 100% vs. 94% • Carotid puncture 1% vs. 10% • Pneumothorax 0% vs. 2. 4% • Hemothorax 0% vs. 1. 7% • Reduced time and number of attempts with US
Jugular and Subclavian anatomy
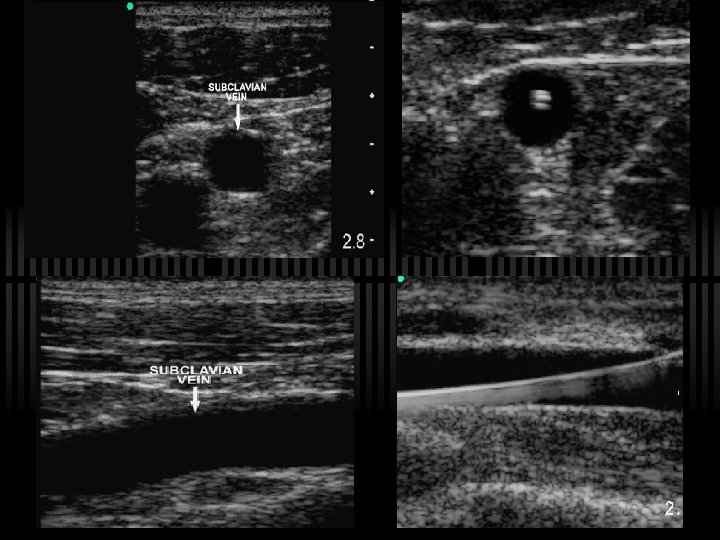
Compression confirms patency
Subclavian vein Transverse Sagittal
Common indications for CVC • Hemodynamic monitoring • Administration of drugs likely to induce phlebitis • Temporary cardiac pacemaker • Hemodialysis • Lack of peripheral venous access
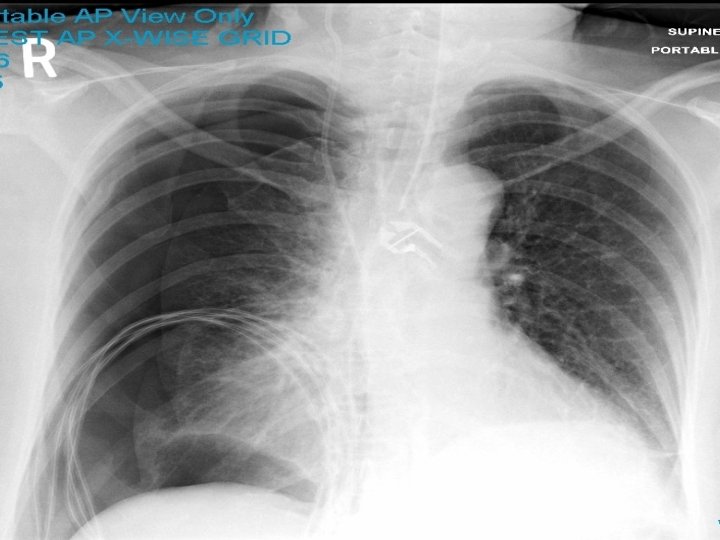
Technique • 5 -10 MHz probe - locate vein, ensure patency, then puncture blindly – but no safer than landmark technique • Real-time visualization of needle tip helps prevent pneumothorax, arterial puncture • Still need X-ray to document tip position, as catheter can still go wrong direction
Technique • Use either transverse or longitudinal orientation of ultrasound beam to needle path • Transverse supposedly easier for novice • Advantage of longitudinal: see needle through entire course • With either, you will NOT see needle tip if out of plane • Can use needle guides to help
Predictors of difficult cannulation • • Emergency Placement Obesity Coagulopathy Intubated Hypotensive/Hypovolemic Edematous patient Known previous difficult cannulation
Static vs Dynamic technique Static technique: • Using 2 -3 ultrasound planes, mark with felt pen Dynamic technique: • • 1 vs 2 person technique Use image as guide Observe needle throughout procedure, as it penetrates vessel Watch tip!
Venous access – easiest to more challenging 1 st CHOICE: Internal/External Jugular 2 nd CHOICE: Femoral – easy 3 rd CHOICE: Subclavian/Axillary – harder due to location, more difficult to visualize while you puncture 4 th CHOICE: Cephalic/Basilic/Antecubital –
Jugular Vein • Large, easy to see, good choice • Trendelenberg, head contralaterally turned 30 degrees • Put probe transversely across vein, just superior to clavicle btn two SCM heads, just superior to clavicle • Bring needle in from laterally above probe (in same plane as transducer), aiming just slightly down to toes ~ 20 -45 degrees (Posterior approach) • Watch needle well away from vein, indenting vein wall, and pop through…and know where carotid is! • Beware of anatomical variants:
Subclavian Vein ü More challenging to see needle and vein at puncture site ü Jugular much easier, less risk of venous stenosis, thrombosis, catheter fracture from pinch off syndrome ü Place probe inferior to most lateral aspect of clavicle ü Puncture axillary-subclavian junction close to clavicle
Femoral vein • Also easy • Orient transducer longitudinally, along course of vein, bring needle in from below, parallel to transducer and vein • Valsalva often helps distend vein, bigger target • Externally rotate leg to move artery more lateral
U/S CVC Pitfalls 1. Failure to identify the vein correctly 2. Failure to locate the needle in tissue
Tips • Awake patient - Check position. If patient has moved after you have landmarked, this results in a change in anatomical position of the vein • Centre vein in middle of the screen • Lighten probe pressure, as may be collapsing vein • Insert needle at sharper angle (45 - 60 degrees), to properly intersect with the vein directly under transducer
7 Steps to Success: 1. Use adequate gel 2. Confirm orientation of probe - conventionally probe head pointing to RIGHT (rub edge with finger, look at screen) 3. Do preliminary US - find patent target vein 4. Mark site (static vs direct technique) 5. Consider local anesthetic 6. Sterilize skin, sterile probe, sterile technique! 7. Advance the needle!
Sterile preparation of US transducer • Apply non-sterile gel to probe • Slip sterile sleeve over transducer, smooth all air bubbles away from scanning surface to prevent artifact • Secure sleeve with rubber band • Alternate: large sterile glove, with fingers folded over, palmar surface of glove is scan surface. • Sterile gel applies outer surface of glove/sterile sleeve
General Tips on CVC insertion ü Be aware that more than 3 failed attempts to cannulate the vein can result in a 6 fold increase in mechanical complication. (Mc. Gee) ü Aids to distinguish arterial vs. venous cannulation ü A pressure transducer can be attached to the needle cannulating the vessel to confirm the presence of venous waveforms and pressure ü Blood gases from the needle in the vessel can be measured and compared with known arterial sample
Summary • US guided procedures have a number of clinical utilities in the ED • US can improve the safety of specific procedures and success rate • Initially, can be more time consuming due to learning curve, but with practice, patience and good hand-eye coordination improve efficiency and efficacy of patient care
References • • Abboud PAC and Kendall JL. Ultrasound guidance for vascular access. Emergency Clinics of North America. 22(3): 749 -773, 2004 Leung, Duffy and Finckh. Ann Emerg Med 2006; 48(5): 540 -7 Mc. Gee DC and Gould MK. Preventing complications of central venous catheterization. NEJM. 348(12): 1123 -33, 2003 Miller AH, Roth BA, Mills TJ et al. Ultrasound guidance versus the landmark technique for the placement of central venous catheters in the emergency department. Academic Emergency Medicine. 9(8) : 800 -805, 2002.
Procedure Video Reference • http: //content. nejm. org
References ü ü National Institute for Clinical Excellence. NICE technology appraisal guidance No. 49: guidance on the use of ultrasound locating devices for placing central venous catheters. London: NICE, September 2002. www. nice. org. uk/pdf/ultrasound_49_GUIDANCE. pdf (accessed 21 Apr 2004) The National Quality Forum. Safe Practices for Better Health Care. A consensus report. Washington, D. C. 2003. www. qualityforum. org (accessed 27 Jan 2005).