UBC Ophthalmology Interest Group Seminar Series 1 18

UBC Ophthalmology Interest Group Seminar Series 1. 18. 2012 ACUTE VISUAL LOSS

ANATOMY REVIEW 24 mm

Photo courtesy: Heather O’Donnell, PGY 2, UBC

PRIMARY CARE APPROACH � History � Onset ie. minutes vs days, following trauma? � Transient vs permanent � Mono vs binocular � Associated symptoms eg. pain, swelling, floaters � Other medical conditions and eye history � Medications

� Eye Exam � Visual acuity � Equivalent to vitals for the eye

VISUAL ACUITY TESTING

� Eye Exam � Visual acuity � Equivalent � Pupils, to vitals for the eye RAPD � Another ‘vitals’, from eye/neuro/trauma point of view � Confrontational visual field � Extraocular movement � Tonometry � External examination � Slit lamp: lids, conjunctiva, AC � Dilated examination, fundoscopy

CASE 1 � Previously well 75 F presents to ED for sudden R eye pain and blurry vision while watching TV at night � c/o “halo” around lights � Symptoms not resolved � Hx: cataract in both eye, mild HTN � No medications

CASE 1 � OD Photo courtesy: A. Doan, MD, University of Iowa CF, OS 20/25 � R pupil fixed 4 mm � Rock hard globe � Corneal edema � Conj injections � Opposite eye looks normal � Nausea, vomit x 1

IMPRESSION AND PLAN? � A. Urgent head CT r/o mass lesion in brain causing high ICP � B. Acute bacterial conjunctivitis, pt needs abx eye drops � C. Chemical keratitis, rinse eye in sterile water for 10 min immediately � D. Acute angle closure glaucoma, consult ophthalmology STAT

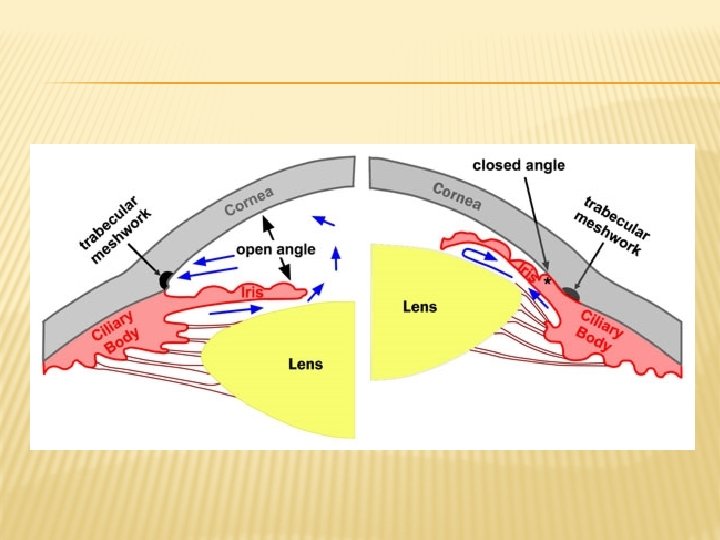
ACUTE ANGLE CLOSURE GLAUCOMA � Results from aqueous outflow obstruction by iris, rise in IOP, ischemia and permanent glaucomatous damage: emergency! � IOP = 42 mm. Hg (normal 12 -20 mm. Hg) � Acetazolamide and timolol were given initially, followed by pilocarpine 1 hour later. � IOP decreased to 19 mm. Hg � Laser peripheral iridotomy arranged the next day is the definitive treatment

LASER PERIPHERAL IRIDOTOMY � Photo courtesy: A. Doan, MD, University of Iowa

CASE 2 � 50 M highly myopic pt sees GP for c/o new onset of “flashing lights and floaters” � Blurry vision but no pain � Otherwise healthy Rev Ophthalmol, 2006, 6: 15

CASE 2 � OD 20/80, OS 20/20 � Pupils, anterior segment normal � Vitreous: tobacco dust � IOP: OD 10 mm. Hg, OS 13 mm. Hg Rev Ophthalmol, 2006, 6: 15

RETINAL DETACHMENT � Rhegmatogenous most common, start as a tear, fluid build up beneath neuroretina separates it from retinal pigment epithelium � High myopia is a risk factor � In office: avoid pressure on globe, protect the eye � Immediate ophthalmological consult required � Surgery is definitive treatment, often urgent

CASE 3 � 75 F Photo courtesy: AAO 2011 with sudden painless loss of vision OD yesterday comes to GP office � A “grey spot” in her vision, grown over 10 min � Hx incl. CAD, HTN, TIA � Denies eye problems

CASE 3 � OD Photo courtesy: AAO 2011 CF, OS 20/30 � R pupil sluggish 3 mm RAPD � EOM full � Cornea, AC grossly normal � IOP 10 mm. Hg B/L � Cranial nerves intact

MANAGEMENT � A. Assure pt that her vision is unsalvageable, she needs to start Plavix to prevent a stroke � B. Send pt to emergency department STAT � C. Compress and release the eye right now � D. You don’t know what this is, so you make a regular referral to ophthalmologist in 2 -3 weeks

CRAO � Central retinal artery occlusion often secondary to embolus in a vasculopathic patient � Ophthalmological emergency � Immediate restoration of retinal blood flow is necessary to save sight � Even with compress, sight is often not salvageable. � Need to evaluate etiology

CASE 4 � 85 F comes to GP for sudden vision loss today � 2 months of transient double vision � She has been feeling fatigued with muscle and joint aches for the last 6 months � New headache in her R temple particularly when she combs her hair � Her jaw is painful when she’s eating

BMJ 2011, 343 d 4783

CASE 4 � OD LP, OS 20/40 � R pupil 3 mm RAPD � EOM full � VF: wide spread loss � Anterior segment normal � ESR from last week: 80 mm/h Dx: A. Temporal arteritis B. Amaurosis fugax C. Multiple sclerosis D. Compressive optic neuropathy

NEXT STEP? � A. Urgent neurology referral as stroke is imminent � B. Start patient on high dose steroids empirically because benefits outweigh risks � C. Ophthalmology referral for a temporal artery biopsy to confirm diagnosis � D. Urgent MRI of brain as it’s most sensitive and specific for confirming a central lesion

TEMPORAL ARTERITIS � Aka giant cell arteritis. Another classic ophthalmological emergency � Suspect in older women with new headache, vision loss, and systemic sx � Elevated ESR/CRP helps to rule in dx � Must initiate high dose steroids immediately followed by temporal artery biopsy

SUMMARY � Approach: Hx, Va, Pupils, out to in, front to back � Acute vision loss is often a sign of serious ocular disease process: � Acute angle closure glaucoma � Retinal detachment � Central retinal artery occlusion � Temporal arteritis � Urgent ophthalmological referral is needed (timeframe usually minutes to hours) � Immediate action is also required; time is

QUESTIONS ? � Acknowledgement � Case editor: Steven Schendel, PGY-4 UBC � Contact �R Tom Liu, UBC Med 2013 � rztom. liu@gmail. com
- Slides: 28