Types of Fractures Clinical Manifestations PAIN LOSS OF






 • Hypovolemic or traumatic shock resulting from hemorrhage (both visible and nonvisible")
 • The onset of symptoms is rapid, usually occurring within")


 • minimal")


 • Compartment syndrome is a complication that develops when tissue perfusion")

, thromboembolism, and pulmonary embolus (PE)")








- Slides: 45
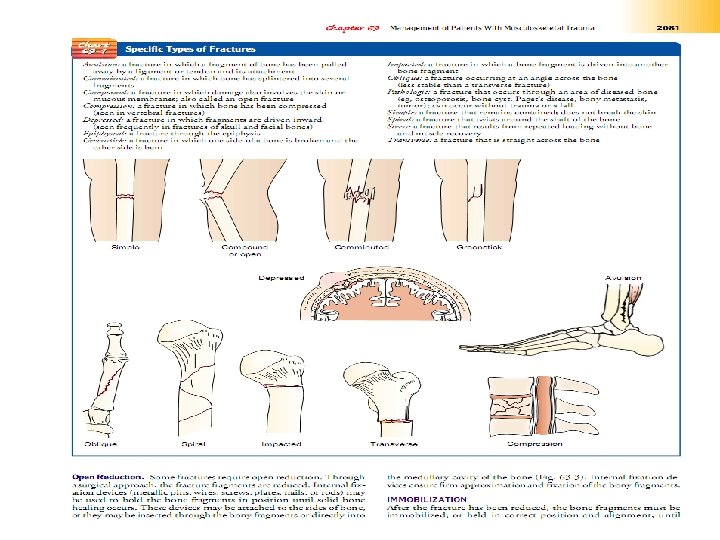
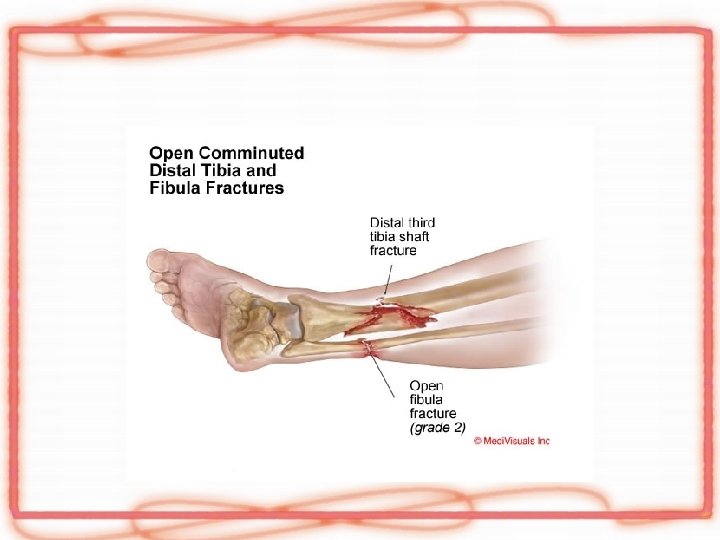
Types of Fractures
Clinical Manifestations PAIN LOSS OF FUNCTION DEFORMITY SHORTENING CREPITUS NURSING ALERT Testing for crepitus can produce further tissue ! damage and should be avoided. • SWELLING AND DISCOLORATION • • •
Factors That Affect Fracture Healing Factors That Enhance Fracture Healing • Immobilization of fracture fragments • Maximum bone fragment contact • Sufficient blood supply • Proper nutrition • Hormones: growth hormone, thyroid, calcitonin, vitamin D, anabolic steroids • • Electric potential across fracture • • •
Factors That Inhibit Fracture Healing • • • • Extensive local trauma • Bone loss • Inadequate immobilization • Space or tissue between bone fragments • Infection • Local malignancy • Metabolic bone disease (eg, Paget’s disease) • Irradiated bone (radiation necrosis) • Avascular necrosis • Intra-articular fracture (synovial fluid contains fibrolysins, which lyse the initial clot and retard clot formation) • Age (elderly persons heal more slowly) • Corticosteroids (inhibit the repair rate)
Complications of fractures • • • early and delayed. Early complications include shock fat embolism compartment syndrome deep vein thrombosis thromboembolism (pulmonary embolism) disseminated intravascular coagulopathy infection.
• • • Delayed complications include delayed union and nonunion avascular necrosis of bone reaction to internal fixation devices complex regional pain syndrome
SHOCK (EARLY) • Hypovolemic or traumatic shock resulting from hemorrhage (both visible and nonvisible blood loss) Treatment of shock Consists: • • restoring blood volume and circulation relieving the patient’s pain providing adequate splinting protecting the patient from further injury and other complications.
FAT EMBOLISM SYNDROME (EARLY) • The onset of symptoms is rapid, usually occurring within 24 to 72 hours, but may occur up to a week after injury.
Clinical Manifestations • • • hypoxia tachypnea tachycardia pyrexia dyspnea crackles wheezes precordial chest pain cough large amounts of thick white sputum
• Occlusion of a large number of small vessels causes the pulmonary pressure to rise. • Edema and hemorrhages in the alveoli impair oxygen transport, leading to hypoxia. • Arterial blood gas values show the partial pressure of oxygen (Pa. O 2) to be less than 60 mm Hg, with an early respiratory alkalosis and later respiratory acidosis. • The chest x-ray shows a typical “snowstorm” infiltrate. Eventually, acute pulmonary edema, acute respiratory distress syndrome, and heart failure develop. • Cerebral disturbances (due to hypoxia and the lodging of fat emboli in the brain) are manifested by mental status changes varying from headache, mild agitation, and confusion to delirium and coma
Prevention and Management • Immediate immobilization of fractures (including early surgical fixation) • minimal fracture manipulation • adequate support for fractured bones during turning and positioning • maintenance of fluid and electrolyte balance are measures that may reduce the incidence of fat emboli. The nurse monitors high-risk patients (adults between 20 and 30 years of age with long bone, pelvic, or multiple fractures or crush injuries, and elderly patients with femur fractures) to identify this problem. • Prompt initiation of respiratory support is essential.
Prevention and Management • The objectives of management are to support the respiratory system, to prevent respiratory and metabolic acidosis, and to correct homeostatic disturbances. Respiratory failure is the most common cause of death. Respiratory support is provided with oxygen given in high concentrations. Controlled-volume ventilation with positive end-expiratory pressure may be used to prevent or treat pulmonary edema. Corticosteroids may be administered to treat the inflammatory lung reaction and to control cerebral edema.
Prevention and Management • Vasoactive medications to support cardiovascular function are administered to prevent hypotension, shock, and interstitial Pulmonary edema. Accurate fluid intake and output records facilitate adequate fluid replacement therapy. Morphine may be prescribed for pain and anxiety for the patient who is on a ventilator. • The patient’s response to therapy is closely monitored. • Because fat emboli are a major cause of death for patients with fractures, the nurse must recognize early indications of fat embolism syndrome and report them promptly to the physician. • Respiratory support must be instituted early.
COMPARTMENT SYNDROME (EARLY) • Compartment syndrome is a complication that develops when tissue perfusion in the muscles is less than that required for tissue viability. The patient complains of deep, throbbing, unrelenting pain, which is not controlled by opioids.
• • • 5 P Pain Paresthesia Paralysis Palor pulseless
OTHER EARLY COMPLICATIONS • • Deep vein thrombosis (DVT), thromboembolism, and pulmonary embolus (PE) are associated with reduced skeletal muscle contractions and bed rest. Patients with fractures of the lower extremities and pelvis are at high risk for thromboembolism. Pulmonary emboli may cause death several days to weeks after injury. Disseminated intravascular coagulopathy (DIC) includes a group of bleeding disorders with diverse causes, including massive tissue trauma. Manifestations of DIC include ecchymoses, unexpected bleeding after surgery, and bleeding from the mucous membranes, venipuncture sites, and gastrointestinal and urinary tracts. All open fractures are considered contaminated. Surgical internal fixation of fractures carries a risk for infection. The nurse must monitor for and teach the patient to monitor for signs of infection, including tenderness, pain, redness, swelling, local warmth, elevated temperature, and purulent drainage. Infections must be treated promptly. Antibiotic therapy must be appropriate and adequate for prevention and treatment of infection
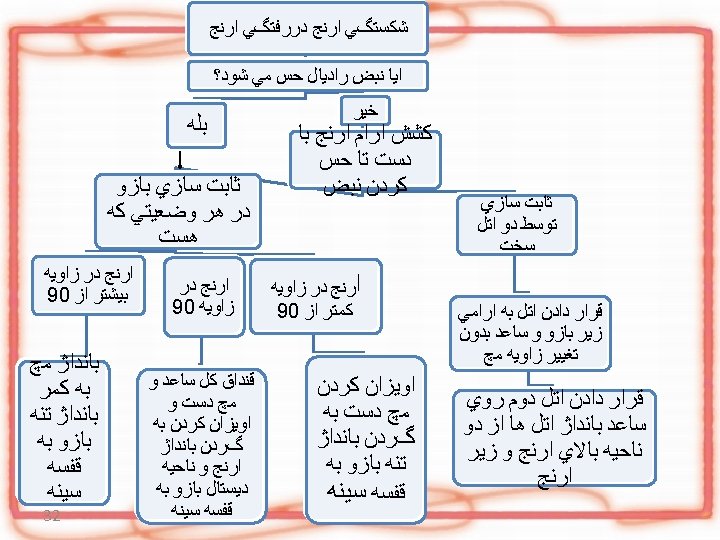
CLAVICLE
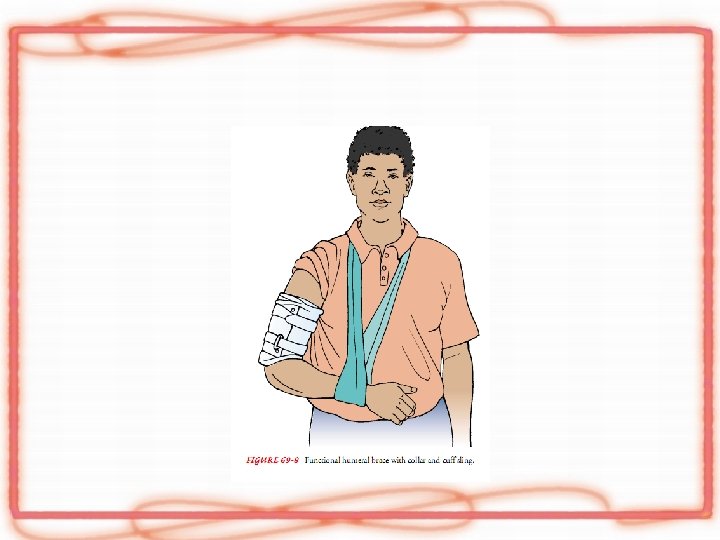
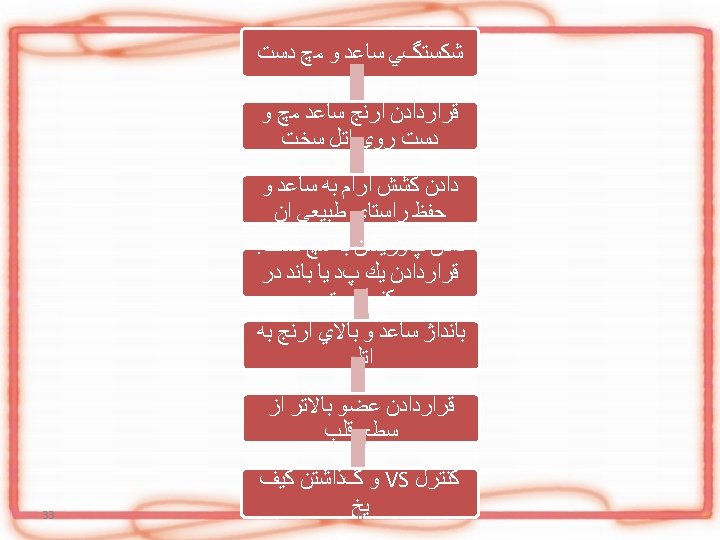
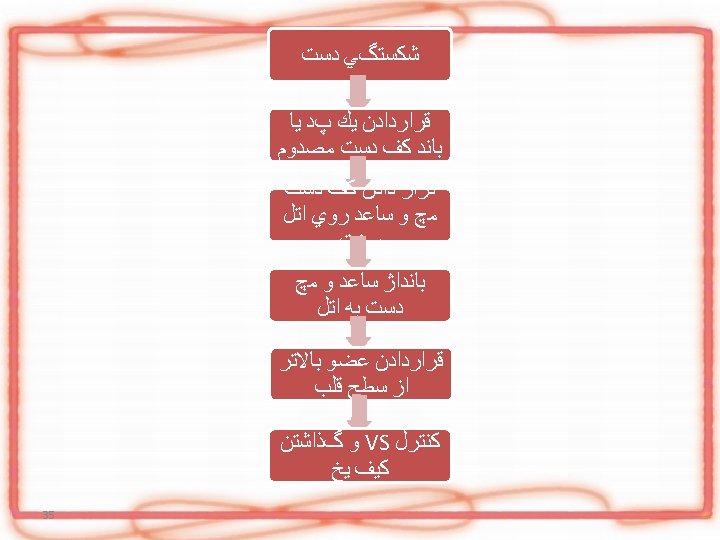
HUMERAL
34 88/9/22
36 88/9/22
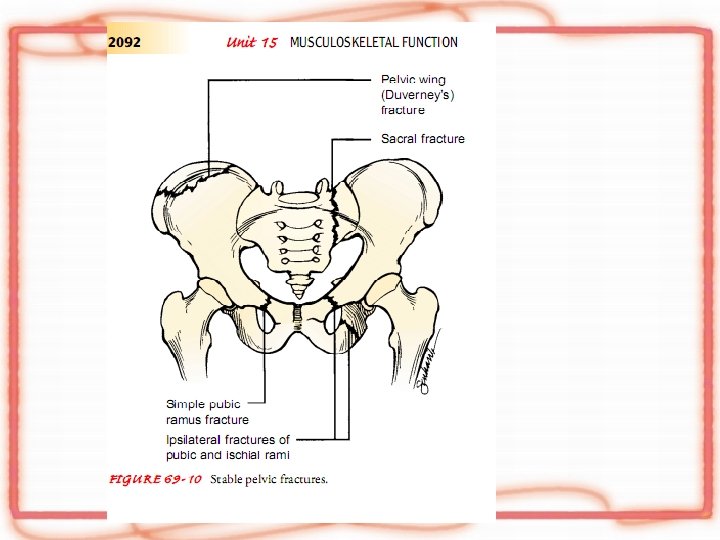
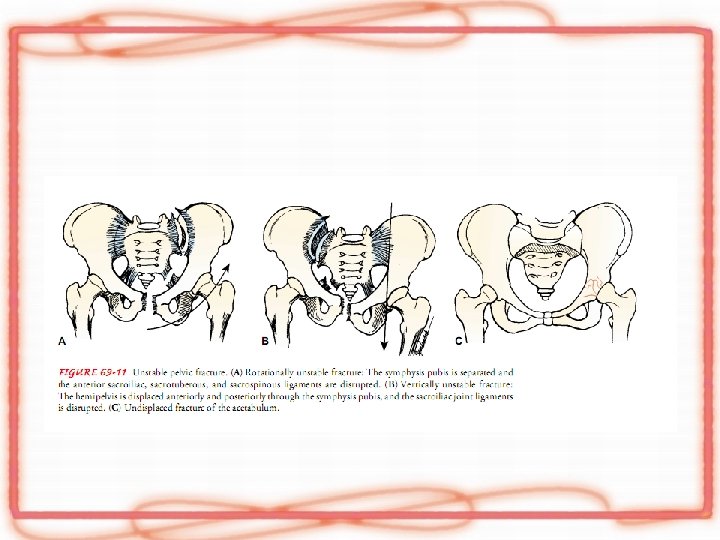
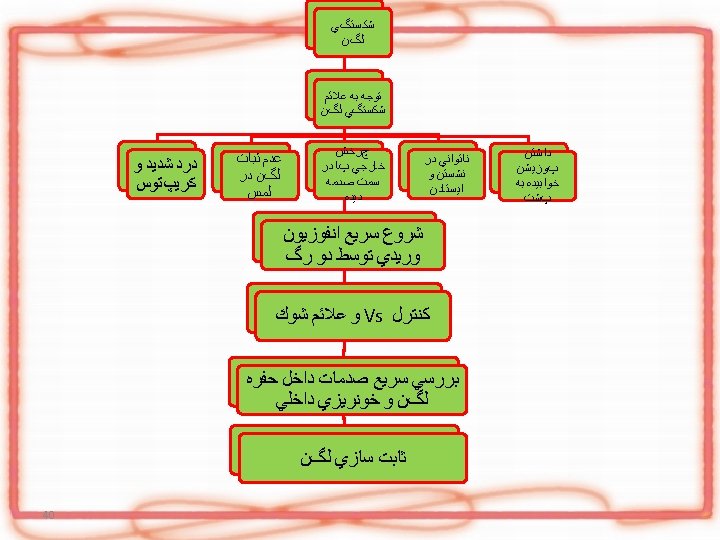
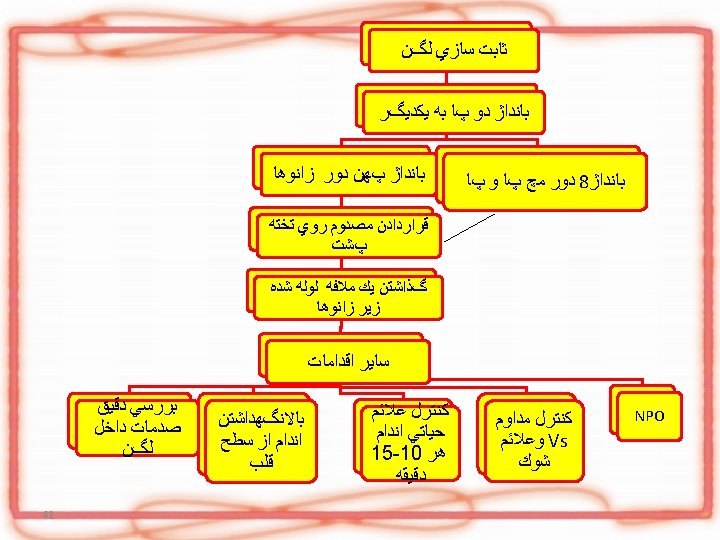
pelvic
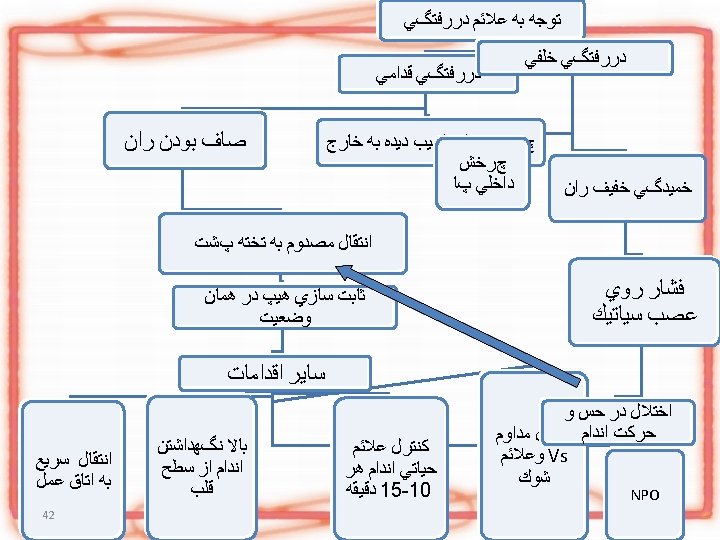
Femur