Type and etiology of CNS infection Type of
 infection")


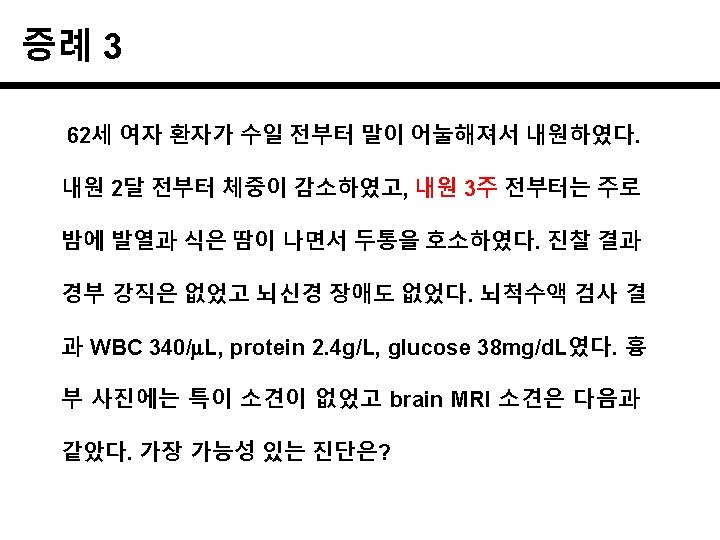
 protein 550 mg/L, glucose 20 mg/L")
 Acute meningitis Subacute~chronic")
,")

 diplococci: S. pneumoniae http: //www. cdc. gov/meningitis/lab-manual/chpt 06 -culture-id. html")
 diplococci: N. meningitis http: //www. cdc. gov/meningitis/lab-manual/chpt 06 -culture-id. html")
 rods: H. influenzae http: //www. cdc. gov/meningitis/lab-manual/chpt 06 -culture-id. html")





;")


 v CSF culture: 6 weeks later, M.")






- Slides: 32
Type and etiology of CNS infection Type of CNS Acute (“ 5 days”) infection Meningitis ** Bacteria (S. pneumoniae) ** Virus (Enterovirus, HSV 2) Encephalitis Viruses (HSV-1) Brain abscess Subacute~chronic (“> 5 days”) ** Mycobacterium tuberculosis Cryptococcus neoformans Bacteria (streptococci + anaerobes) Harrison’s Principles of Internal Medicine, 18 e. chapter 381
Meningeal irritation sign
Management of bacterial meningitis “급성 발열과 두통 ” 요추천자 바로 못 할 때는 “혈액 배양” 하고 바로 항균제 치료 시작 Tunkel AR, et al. Clin Infect Dis 2004; 39: 1267 -84
CSF tapping WBC 750/m. L (poly 90%) protein 550 mg/L, glucose 20 mg/L
CSF finding by type of meningitis Pressure (mm. H 2 O) Acute meningitis Subacute~chronic meningitis Normal Bacteria Virus Tuberculosis Cryptococcus 90 -180 N- WBC/mm 3 0 -5 > 1, 000 5 -1, 000 25 -500 % PMNs 0 -15 90 < 50* 10 -1, 000 (평균 50) < 50 Protein (mg/d. L) 20 -50 100 -500 100 -200 20 -500 Glucose (mg/d. L) 40 -70 < 40 N** (< 40 in 3/4) (< 30) 0. 6 < 0. 4 0. 6 CSF/serum glucose Gram stain, culture N- (50 -100) PCR * Lymphocyte가 우세하지만, 초기에는 PMN 80%까지 가능 ** Mumps, HSV, CMV 중 1/4에서 감소 AFB stain TB-PCR Mycobacteri al culture Indian ink Cryptococcal latex agglutination test
S. pneumoniae meningitis의 항균제 CSF, blood: S. pneumoniea 동정 PCN MIC 0. 03 (S), Ceftriaxone MIC 0. 5 (S) Penicillin MIC Standard therapy 0. 06 g/m. L (S) Penicillin 0. 06 -1. 0 g/m. L (I) Cefotaxime or ceftriaxone ≥ 2. 0 g/m. L (R) Vancomycin plus (Cefotaxime or ceftriaxone) Tunkel AR, et al. Clin Infect Dis 2004; 39: 1267 -84
경험적 항균제 선택의 기준이 되는 것은? 1. CSF profiles compatible bacterial meningitis 2. CSF Gram stain & culture / blood culture 3. latex agglutination test 4. Age and predisposing conditions
CSF gram stain Gram(-) diplococci: S. pneumoniae http: //www. cdc. gov/meningitis/lab-manual/chpt 06 -culture-id. html
CSF gram stain Gram(-) diplococci: N. meningitis http: //www. cdc. gov/meningitis/lab-manual/chpt 06 -culture-id. html
CSF gram stain Gram(-) rods: H. influenzae http: //www. cdc. gov/meningitis/lab-manual/chpt 06 -culture-id. html
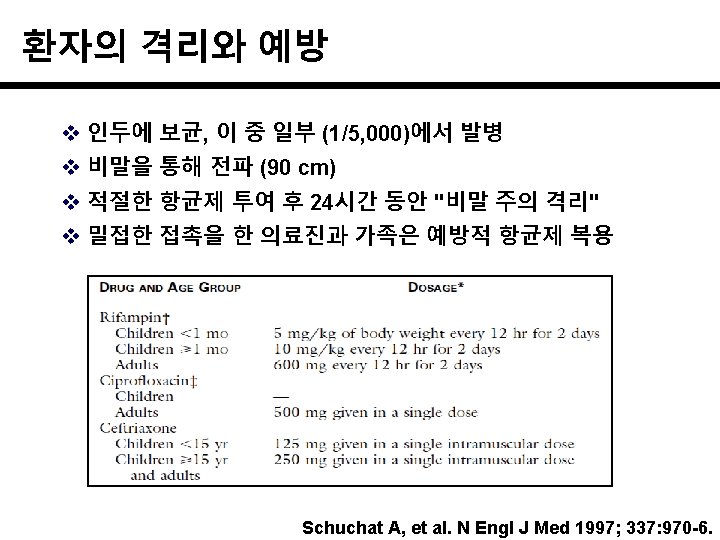
나이별 주요 원인 균 Ceftriaxone + vancomycin Ampicillin Schuchat A, et al. N Engl J Med 1997; 337: 970 -6.
Tunkel AR, et al. Clin Infect Dis 2004; 39: 1267 -84
얼마나 오래 항균제를 투여하나? Tunkel AR, et al. Clin Infect Dis 2004; 39: 1267 -84
Outcomes Swartz MN. N Engl J Med 2004; 351: 1826 -8
Purpura fulminans
Meningococcal meningitis v 13 serogroups; A/B/C/Y/W 135 - nearly all diseases v A (C); third-world countries v B & C; industrialized (90% in US) v Endemic rates are low but epidemics ! v meningitis, septicemia, septic shock with MOF v Mortality is still > 10% (septicemia 40%) v No other infection so quickly kills ! 사망자 1/2은 첫 증상 후 24시간 내 사망 사망자 1/3은 입원 후 6시간 내 사망 생존자의 11~19%는 후유증이 남음
왜 신병에서 발생하나? v Age of high risk; < 4 & 15 ~ 24 years old v Diverse geographic areas & strains v Crowded living conditions v In US Army, vaccination since 1971 v Dormitory of US College in 1998 ~ 99 2. 2 / 100, 000 / yr vs. 1. 4 of same age group
미군에서의 예방접종효과 C C/A/Y/W Maiden MC. Philos Trans R Soc Lond B Biol Sci 2013; 368: 20120147
v Basal meninges v CSF AFB (-) v CSF culture: 6 weeks later, M. tuberculosis contrast-enhanced T 1 -weighted MRI
결핵성 수막염의 병인 1. inhalation 3. lymphatics thoracic duct 2. multiply 4. General circulation 5. metastatic foci
결핵성 수막염의 병인 v primary infection Hematogenous spread Rupture of subependymal tubercles spread to subarachnoid space basilar portion of brain tuberculous meningitis
결핵성 수막염의 임상적 발현 v Subacute to chronic course v Fever, headache, night sweat, weight loss, malaise, lethargy v Infarct, SOL, hydrocephalus headache, vomiting, confusion, seizure v Cranial nerve involvement IV (trochlear) > II, III, VIII
결핵성 수막염의 진찰소견 v Chest X-ray; pulmonary tuberculosis ? v Stiff neck, cranial nerve defects v Fundoscopic examination: choroidal tubercle
결핵성 수막염의 진단 v 확진이 매우 어렵다 - 의심해야 진단할 수 있다. v CSF 소견 fungal, partially treated bacterial meningitis와 비슷 gross; clear or slightly opaque overnight stand; small wisp-like pellicle WBC; 100 -500/ L (PMN to MN) protein; elevated glucose; < 45 -50 mg/dl (< 1/2 serum level) v CSF AFB smear (<20%) v CSF culture (50 -80%) v PCR sensitivity (~50%)
결핵성 수막염의 치료 v Prompt Anti-TB medication : 12 months cf. osteoarticular TB: 6~9 months v Steroid adjunctive therapy