Type 1 Diabetes In Adults Dr Mitra Niafar

Type 1 Diabetes In Adults Dr Mitra Niafar Department of Endocrinology Tabriz University of Medical sciences

Agenda Introduction Prevalence Misdiagnosis Differential Diagnosing Diabetes In Adults– Type 1, LADA, or Type 2? • Management of Type 1 Diabetes in Older Adults • •

Introduction • The term diabetes mellitus describes several diseases of abnormal carbohydrate metabolism that are characterized by hyperglycemia. • It is associated with a relative or absolute impairment in insulin secretion, along with varying degrees of peripheral resistance to the action of insulin. Diaz-Valencia et al. BMC Public Health (2015) 15: 255

Definition • Type 1 diabetes is a disease in which autoimmune destruction of pancreatic βcells leads to insulin deficiency. • Controlling blood glucose with an acceptable range is a major goal of therapy. Point Care. 2017 March ; 16(1): 37– 40.

Management • Regular and life-long insulin administration is necessary to prevent: • Hyperglycemia • Metabolic decompensation • Life-threatening diabetic ketoacidosis (DKA) Diabetes Metab J 2018; 42: 3 -18

Diabetes: A global emergency Number of people with diabetes worldwide and per region in 2017 and 2045 (20 -79 years) The IDF Diabetes Atlas 8 th Edition. 2017
, there were approximately")
Worldwide prevalence of DM According to the International Diabetes Federation (IDF), there were approximately 425 million people living with diabetes worldwide in 2017, out of which 5% to 10% are estimated to have T 1 DM.
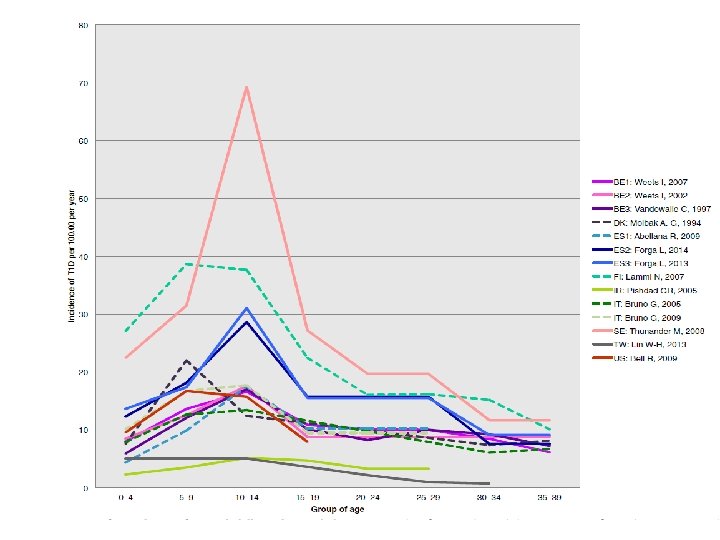

Comparison of male and female T 1 D adult incidences • The mean male-to-female ratio in our review was 1. 47 (95% CI for mean 1. 33 -1. 60, SD = 0. 49, n = 54, p = < 0. 0001). Diaz-Valencia et al. BMC Public Health (2015) 15: 255
")
Type 1 Diabetes Mellitus in Adults • Although type 1 diabetes (T 1 D) can affect patients of all ages, most epidemiological studies of T 1 D focus on disease forms with clinical diagnosis during childhood and adolescence. • Clinically, adult T 1 D is difficult to discriminate from certain forms of Type 2 Diabetes (T 2 D) and from Latent Autoimmune Diabetes in Adults (LADA). Diaz-Valencia et al. BMC Public Health (2015) 15: 255

Differential Diagnosis • Many of those with type 1 diabetes after the age of 30 are thought to have type 2 diabetes at first, and not initially treated with insulin to control blood sugar levels. • Previous published research found that, on average, it took a year for those with type 1 diabetes who had been misdiagnosed with type 2 to be put on insulin.

Misdiagnosis Among the adults with type 1 diabetes to have been misdiagnosed is Theresa May, the Prime Minister, who was initially told by doctors she had type 2 diabetes and given tablets which did not control her blood sugar.

Lancet Diabetes Endocrinol 2018; 6: 122– 29

Findings • 3· 5% of white European individuals in UK Biobank had developed diabetes in the first six decades of life. • 13 250 (3· 5%) of 379 511 white European individuals in UK Biobank had developed diabetes in the first six decades of life. 1286 had type 1 diabetes. • 537 (42%) were in individuals diagnosed when aged 31– 60 years, representing 4% (537/12 233) of all diabetes cases diagnosed after age 30 years.

Findings The clinical characteristics of the group diagnosed with type 1 diabetes when aged 31– 60 years were similar to the clinical characteristics of the group diagnosed with type 1 diabetes when aged 30 years or younger. Lancet Diabetes Endocrinol 2018; 6: 122– 29

Clinical characteristics differences between type 1 and type 2 diabetes mellitus in adults • They had a lower BMI 27· 4 kg/m² vs 32· 4 kg/m² • Were more likely to use insulin in the first year after diagnosis 89% vs 6% • Were more likely to have diabetic ketoacidosis 11% vs 0· 3% Lancet Diabetes Endocrinol 2018; 6: 122– 29

Incidence of genetically defined type 1 and type 2 diabetes in the first six decades of life

Current Diabetes Classification Ø Note the OVERLAP Ø Diagnosis is Often IMPRECISE

Heterogeneity of Diabetes Metab J 2018; 42: 451 -464

Visualization of the Overlap IMMUNITY AGE GENES BMI INSULIN THERAPY T 1 DM In children Strong +++ child HLA++ low Intermediate Immediate T 1 DM In adults ++ adult HLA+ normal Immediate LADA + adult HLA normal Variable T 2 DM weak adult ? high Infrequent Adapted from Leslie et al. Diabetes Metab Res Rev. 2008 Oct; 24(7): 511 -9

Characteristics Frequently Overlap T 1 D Typical Age of Onset All Ages % of all Diabetes Typical BMI Ethnicity Progression to insulin Dependence Insulin Resistance Presence of Autoantibodies T cell reponses to islet proteins Insulin/ C-peptides Level at diagnosis Ketoacidosis Insulin Secretion Islet Inflammation HLA Link TCF 7 L 2 Link ‘LADA’ Usually Age >30 10% Late Treatment Adults MODY Usually Age <25 10% 75% 5% Mostly Overweight or Obese Mostly normal All Depends on MODY Fast (Days/Week) Latent (Months/Years) Slow (Years) type Depends on MODY Mostly no; ~10% , yes Some Yes type Yes (ICA, IA 2, GAD 65, Yes (mostly GAD 65), IAA) Some not No No Mostly Normal or Thin Overweight All Yes Undectable or extermely low Yes Low/null Chronic Inflammation High None Yes No No Low Yes, many not all Varies Chronic Inflammation Low Greater than T 2 DM Normal to High Rare Varies Chronic Inflammation None ? 5% Normal Rare Varies None PTPN 22; INS; CTLA 4; Other Genes Involved CCR 5; FOXP 3; PTPN 22; INS HNF 1 A; IL 2 RA; IL 6; ITPR 3; OAS 1; SUMO 4 Early Treatment T 2 D PPARG; JAZF 1; HNF 4 A; GCK; HNF 1 A; KCNJ 11; NOTCH 2; IPF 1; HNF 1 B; WFS 1; IGF 2 BP 2; FTO; NEUROD 1 SLC 30 A 8; HHEX Insulin required, Non-Insulin or insulin, Non-Insulin, diet & exercise helpful diet & increased activity Gene Specific Insulin, pills, diet, Insulin, diet, exercise Gene Specific

Characteristics Frequently Overlap T 1 D Typical Age of Onset All Ages % of all Diabetes ‘LADA’ T 2 D Usually Age >30 Adults Usually Age <25 Obese All Mostly normal All Depends on MODY type 10% 75% T 1 D ‘LADA’ T 2 D Mostly Normal or Mostly Overweight or Typical BMI Ethnicity Progression to insulin Dependence Mostly Normal or Thin Overweight All Insulin Resistance Presence of Autoantibodies T cell reponses to islet proteins Insulin/ C-peptides Level at diagnosis Ketoacidosis Insulin Secretion Islet Inflammation HLA Link TCF 7 L 2 Link Mostly no; ~10% , yes Some Yes (ICA, IA 2, GAD 65, Yes (mostly GAD 65), IAA) Some not No Insulin Secretion Low/null Fast (Days/Week) Varies T 1 D Early Treatment Late Treatment No T 2 D MODY No Yes, many not all Varies Chronic Inflammation Low Greater than T 2 DM None No Chronic Normal to High. Inflammation Normal Inflammation PTPN 22; INS; CTLA 4; Other Genes Involved CCR 5; FOXP 3; PTPN 22; INS HNF 1 A; IL 2 RA; IL 6; ITPR 3; OAS 1; SUMO 4 TCF 7 L 2 Link Varies ‘LADA’ Yes Chronic Low Inflammation Yes Undectable or extermely low Yes Low/null Chronic Inflammation High None Rare Varies Chronic Inflammation None ? 5% ‘LADA’ PPARG; JAZF 1; None Rare Varies None T 2 D MODY HNF 4 A; GCK; HNF 1 A; KCNJ 11; NOTCH 2; IPF 1; HNF 1 B; WFS 1; IGF 2 BP 2; FTO; NEUROD 1 SLC 30 A 8; HHEX Greater than T 2 DM 5% MODY Varies Latent (Months/Years) Slow (Years) T 1 D Islet Inflammation MODY ? 5% Insulin required, Non-Insulin or insulin, Non-Insulin, diet & exercise helpful diet & increased activity Gene Specific Insulin, pills, diet, Insulin, diet, exercise Gene Specific None

‘Definitions of LADA’ A. The Immunology of Diabetes Society –LADA, and Action LADA 1. 30 years of age 2. Positive for at least one of the four antibodies commonly found in T 1 D 3. Not treated with insulin within the first 6 months after diagnosis Implies: antibody positive adults, that may be on insulin, but may not be insulin dependent B. ADA recognizes LADA as a variation of T 1 DM 1. Also called: Ø Type 1. 5 Ø ‘Slowly’ progressive Type 1 D Ø Latent-onset Type 1 D Implies: insulin-dependent antibody-positive adults
 Compared to Type 2")
Etiology and Pathogenesis of Latent Autoimmune Diabetes in Adults (LADA) Compared to Type 2 Diabetes Frontiers in Physiology. March 2019 Volume 10 , Article 320

Etiology and Pathogenesis Despite the autoimmune nature of LADA and clear genetic overlap with type 1 diabetes, studies on lifestyle and LADA risk indicate that factors such as overweight and physical inactivity that are associated with insulin resistance and type 2 diabetes may also promote LADA. Frontiers in Physiology. March 2019 Volume 10 , Article 320

Relative risk for LADA and type 2 diabetes in relation to lifestyle factors Frontiers in Physiology. March 2019 Volume 10 , Article 320

Etiology of LADA, model based on current knowledge Frontiers in Physiology March 2019 | Volume 10 | Article 320

Diabetes Metab J 2018; 42: 451 -464

Summary • Studies conducted to date indicate that LADA, similar to type 2 diabetes, results from an imbalance between insulin sensitivity and insulin secretion. • The relative contribution of insulin deficiency to disease progression is greater in LADA. Frontiers in Physiology March 2019 | Volume 10 | Article 320

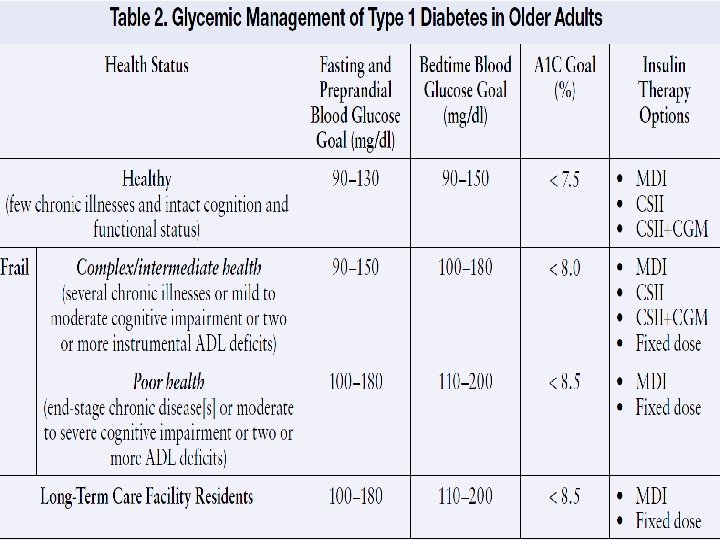
Managing Type 1 Diabetes in Older Adults Older adults with complex or intermediate health status have: • • • Multiple chronic illnesses Have mild to moderate cognitive impairment Dependency in activities of daily living Susceptible to hypoglycemia Complex insulin regimens may become difficult for them to follow Diabetes Spectrum Volume 27, Number 1, 2014

Take Home Message Ø Type 1 diabetes is not predominantly a 'disease of childhood‘ Ø Adults are as likely to develop type 1 diabetes as children, with more than 40 per cent of type 1 diabetes cases occurring after the age of 30. Ø Not all cases of late onset diabetes are type 2. Ø An individualized approach to managing type 1 diabetes becomes crucial in this population, with consideration of an A 1 C goal of < 8. 0%

Dr Mitra Niafar Professor Department of Endocrinology Tabriz University of Medical sciences E-mail: dr_niafar@yahoo. com
- Slides: 34