Twelfth NASA International Continuing Health Education Series Bioterrorism

Twelfth NASA International Continuing Health Education Series: Bioterrorism Washington, DC August 22, 2003

‘I Think I Have Anthrax…’: Responding to Bioterror in the National Capital Region Dan Hanfling, MD, FACEP Director, Emergency Management and Disaster Medicine Inova Health System Medical Director, Inova Air. Care Falls Church, VA

Seminar Objectives • Understand the catastrophic threat posed by bioterrorism • Review detailed case presentations of two inhalation anthrax patients • Describe key lessons learned from anthrax clinical presentations • Re-evaluate CDC diagnostic criteria • Discuss implications for health and medical facility disaster preparedness

Creating Enemies “Super empowered Angry Man” versus Superpower“ lot of people dead” NOT “…a lot of people watching” … Thomas L. Friedman, The Lexus and the Olive Tree, 1999
 • Huddle • Line of Scrimmage • Football")
Models of Warfare • Football (American) • Huddle • Line of Scrimmage • Football (Rest of the World) • Continuous play • No lines of demarcation IMPLICATION: Defend against multiple attacks in multiple cities within short periods of one another

What threat poses the geatest risk?
 is a technical challenge •")
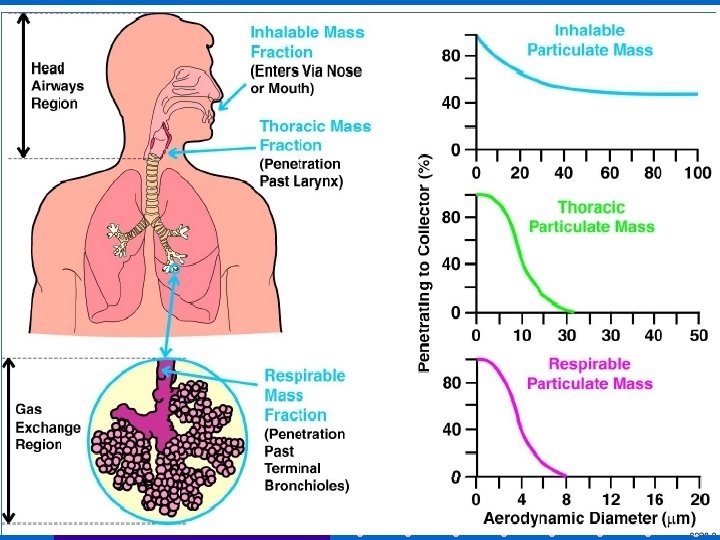
“RELOAD” • Making ‘weaponized’ anthrax (1 -5 micron range) is a technical challenge • Once accomplished, a much lesser challenge to make 1 kg or 100 kg • a particular attribute that lends itself to repeated attacks • effective as a tool of political terrorism [disabling government by diverting resources and undermining confidence of citizens in their government]

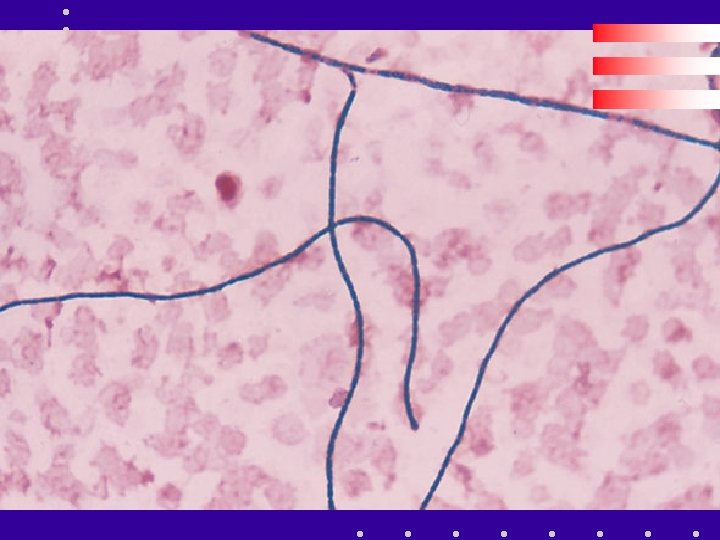
Pathophysiology of Inhalation Anthrax • Deposition of sufficient number of anthrax spores [8 -10 thousand] into alveolar space • 1 to 5 micron size spores ingested by macrophages • spores then transported to mediastinal LN’s • germination of spores to B anthracis occurs within 1 -3 days and as late as 60 days

Pathophysiology of Inhalation Anthrax • Anthrax toxins are released from LN’s • protective antigen • lethal factor • edema factor • Protective antigen and Lethal factor combine to form Lethal toxin • Results in hemorrhagic mediastinitis and edema; bloody effusions • Hematogenous spread of bacteria
 More than “bad meat” Less than one gram of anthrax")
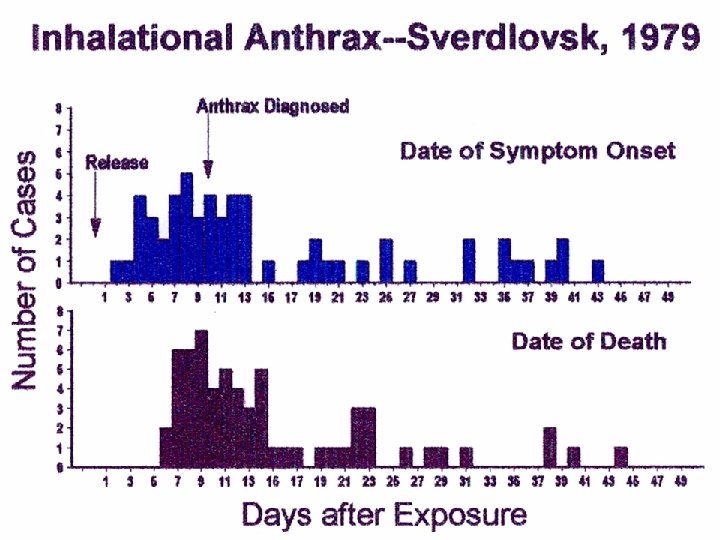
Sverdlosk Anthrax Release (1979) More than “bad meat” Less than one gram of anthrax spores released from bioweapons facility leading to 96 human cases of anthrax – last case 43 days after the spore release – 77 pulmonary cases – 66 deaths – 11 survivors – Case Fatality rate of 87% – Average length of hospitalization: • 3 weeks for survivors • 2 -3 days for fatalities
 • October 12 • • • October 15")
NCR Anthrax Attacks Timeline (October 2001) • October 12 • • • October 15 October 17 October 19 • October 21 Letters Processed at Brentwood Daschle letter opened FBI mail quarantine Patient evaluated at Inova Fairfax Hospital Anthrax Dx confirmed Brentwood closed

Monday 15 October 2001

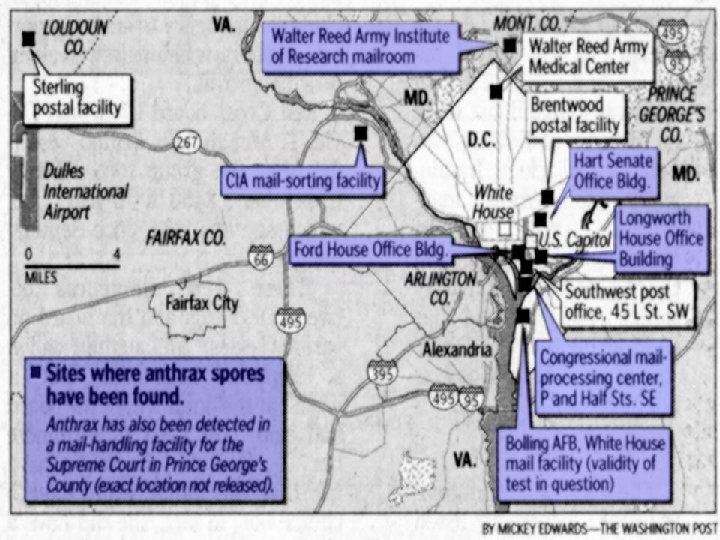
Brentwood • Postal Processing and Distribution Center • 500, 000 square feet facility • 59 million pieces of incoming mail processed between 11 October and 21 October • 2 contaminated envelopes sent from PDC Trenton, NJ • processed through high speed envelope sorting machine • cleaned at end of each shift with forced compressed air (70 lbs per square inch)

Anthrax Aerosolization • Anthrax spores released thru mail and can easily disseminate throughout buildings • spores found on all 3 floors of AMI Building (Florida) [Emerg Infect Dis, October 2002] • spores found throughout Brentwood [MMWR, December 21, 2001]

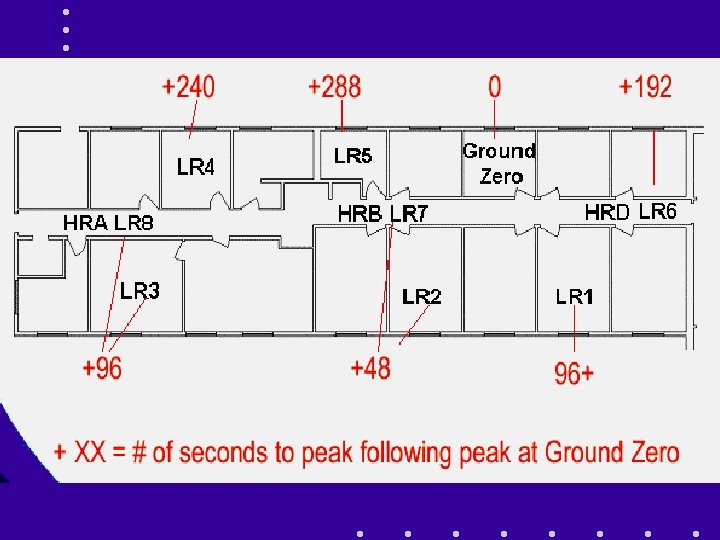
How large an inoculum? Canadian Defence Research Establishment Suffield • Risk of transmission of spores from an envelope • 0. 1 or 1. 0 g of Bacillus globigii spores released in a 10 x 18 x 10’ room • Significant numbers of spores aerosolized within seconds – >99% 2. 5 to 10 µm size – estimate of 480 to 3080 LD 50 s potentially inhaled in 10 min. – “the aerosol would quickly spread throughout the room so that other workers…. would likely inhale lethal doses”
 56 Race AA 56 AA Case 3 Case")
Case 1 Case 2 Age (yrs) 56 Race AA 56 AA Case 3 Case 4 55 AA 47 AA Date symptoms began 10/16 Date of suspected IA diagnosis 10/19 10/20 10/21 10/22 Date IA confirmed 10/21 10/22 10/23 10/26 Underlying medicalconditions No No Yes( b) Yes( c) Death No No Yes(10/21) Yes(10/22)

Inova Patient 1 October 19, 2001 • 56 year old African American male, postal worker • 3 days PTA: low grade fever, chills, cough, DOE, malaise, pleuritic CP • ED Chief Complaint: “I think I have anthrax. ” • T 37. 5 HR 110 RR 18 BP 157/75 Sa. O 2 98%(RA) • 7. 5 WBC • CXR: minimally widened mediastinum, bilat hilar masses, small R pleural effusion Mayer T, Bersoff-Matcha S, Murphy C, Hanfling D, et. al.

Inova Patient 1 October 19, 2001 • Micro: Bacillus anthracis G+ rods grown from blood culture at 11 hrs (confirmed by CDC PCR assay) • Treatment: • IV Cipro 400 mg q 8 hrs [first line recommendation, Inglesby, et. al. ] • IV Rifampin 300 mg q 12 hrs [G+ coverage; intracellular mechanism] • IV Clindamycin 900 mg q 8 hrs [known antitoxin effect in streptococcal disease] Mayer T, Bersoff-Matcha S, Murphy C, Hanfling D, et. al.

Case 1: Initial radiograph

Case 1: Initial CT Enlarged lymph nodes

Case 1: Initial CT Mediastinal edema

Case 1: Initial CT Peripheral Air-space disease

Inova Patient 2 October 20, 2001 • 56 year old African American male, postal worker • 3 days PTA: progressively worsening HA, nausea, chills, night sweats; no fever; no respiratory sx • ED Chief Complaint: Severe Headache • T 37. 6 HR 127 RR 20 BP 133/87 Sa. O 2 94%(RA) • 9. 7 WBC • Head CT normal • CXR: wide mediastinum, bilat hilar masses, R pleural effusion Mayer T, Bersoff-Matcha S, Murphy C, Hanfling D, et. al.

Inova Patient 2 October 19, 2001 • Lumbar puncture: 20 RBC, 4 WBC, glu 92, Gram stain neg, Culture no growth • Micro: Bacillus anthracis grown from blood culture at 15 hours (confirmed by CDC PCR) • Treatment: • IV Cipro 400 mg q 8 hrs • IV Rifampin 300 mg q 12 hrs IV Clindamycin 900 mg q 8 hrs Mayer T, Bersoff-Matcha S, Murphy C, Hanfling D, et. al.

Previously Existing Literature on Inhalation Anthrax • Early diagnosis “exceedingly difficult” (absent clearly defined exposure history) • Illness characterized by 2 stage clinical course • early nonspecific respiratory symptoms • 24 -72 hrs abrupt onset fever, dyspnea, shock • death 80 -90% of patients Inglesby T, et. al. JAMA 1999 281: 1735 -1745.

Previously Existing Literature on Inhalation Anthrax • Radiographic presence of wide mediastinum considered pathognomonic, but late finding “. . . treatment at this stage would be unlikely to alter the outcome of the illness. ” Inglesby T, et. al. JAMA 281: 1735 -1745.

Inova Experience Lessons Learned First, clinical symptoms of inhalational anthrax include sweats (often described as drenching) and nausea and vomiting (which may indicate involvement of the gastrointestinal tract at an earlier stage than was previously appreciated), with each symptom presenting in over half of patients.

Inova Experience Lessons Learned Second, among patients who presented in the first, prodromal phase of the illness, none were described as appearing severely ill. Indeed the difficulty of distinguishing influenzalike illness (ILI) from inhalational anthrax was a difficult aspect of patient management during this outbreak.

Inova Experience - Lessons Learned Third, prior to this outbreak, it was thought that it would be exceedingly difficult to identify and successfully treat patients in the prodromal phase of the disease, at least until a known index case of inhalational anthrax had been identified. Further, it was thought that once radiographic findings of the disease were present on chest radiographs the high mortality rates previously quoted would pertain.

Inova Experience Lessons Learned Finally, early identification and aggressive treatment of these patients (including treatment with multiple antibiotics and supportive intensive care unit care) resulted in a survival rate of 55% versus the 10 -20% survival rates in previous series.

Challenging the CDC Guidelines • Mean number of symptoms • survivors 8. 5 symptoms • deceased 5. 5 symptoms • Fever (T > 37. 8) 7 out of 11 cases • Tachycardia 10 out of 11 cases [mean 116, range 79 -152] • Blood Culture median time 18 hr growth Mayer T, Morrison A, Bersoff-Match S, Hanfling

Challenging the CDC Guidelines • Abnormal CXR 10 out of 11 cases [4 initially interpreted as normal] • Mean number of days from onset of symptoms until treatment • survivors 4. 7 days • deceased 5. 8 days • Patients surviving inhalation anthrax 6 out of 11 cases [55%] Mayer T, Morrison A, Bersoff-Match S, Hanfling

Challenging the CDC Guidelines • Current CDC Guidelines identify 1 out of 11 cases for appropriate screening and treatment for inhalation anthrax • primarily because of reliance on epidemiologic confirmation of exposure Mayer T, Morrison A, Bersoff-Match S, Hanfling

Challenging the CDC Guidelines • Revised Guidelines would identify 8 out of 11 cases of inhalation anthrax Clinical presentation consistent with inhalation anthrax (tachycardia, fever and > 5 symptoms) OR epidemiologic confirmation Mayer T, Morrison A, Bersoff-Match S, Hanfling

Reliance on Epidemiologic Plus Clinical Factors • The current CDC algorithm requires either a known “history of exposure or occupational/environmental risk” in addition to a two to five day illness consistent with inhalational anthrax. • However, all ten patients who failed to be identified by the guidelines lacked a clearly known exposure or known occupational/environmental risk at the time of their initial clinical presentation.

• Tachycardia as a Cardinal Sign The only clinical sign included in the current CDC guidelines is fever. • seven of 11 patients had fever, but the mean presenting temperature was only 38. 0ºC • While previous reports and commentary by Mayer, et al, and Lane and Fauci have noted the importance of tachycardia out of proportion to the clinical symptoms in these patients, tachycardia is not currently listed as a presenting sign in the CDC guidelines.

Reliance on Clinical Observation Prior to Confirmation of Exposure • Current guidelines indicate that patients who do not have both a documented history of either exposure or occupational/environmental risk and a 2 -5 day illness consistent with inhalational anthrax should be observed closely, with antimicrobial prophylaxis provided only if exposure is confirmed.

Time to Treatment • Important to note that four patients were evaluated by healthcare workers and were originally discharged. • The two patients who were not treated with antibiotics died. • The two patients who were originally discharged who subsequently lived were placed on ciprofloxacin or levofloxacin and had blood cultures obtained at the time of the first visit.

Time to Treatment • These cases support the concept that the opportunity for successful treatment of inhalational anthrax lies in a narrow therapeutic window between the first and second phases of the disease. • By extension, early post-exposure chemoprophylaxis may actually constitute early therapy and is to be viewed as a vital component of appropriate care.
- Slides: 45