Tumours of Nasopharynx Dr Mubeena ANATOMY OF NASOPHARYNX

Tumours of Nasopharynx Dr Mubeena

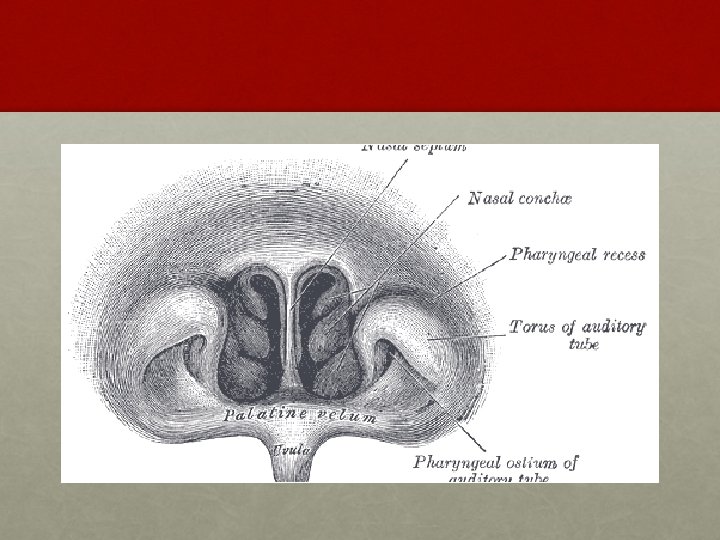
ANATOMY OF NASOPHARYNX • It opens anteriorly into the nasal cavity.

Benign tumors of nasopharynx

Juvenile nasopharyngeal angiofibroma

introduction • Rare, benign • Locally destructive fibrovascular tumour

Epidemiology • Males • Teenage, young adult • Hamartomatous nidus of vascular tissue which get activated to form angiofibroma when male sex hormone is released. • Extremely rare in female/ patient older than 25
:")
Origin • Posterolateral nasal wall at sphenopalatine foramen (Operative Techniques in Otolaryngology 1999; 10(2): 101 -106. )

pathology • Vascular and fibrous stroma • Vessels – endothelium lined spaces – no elastic or muscle coat

Spread

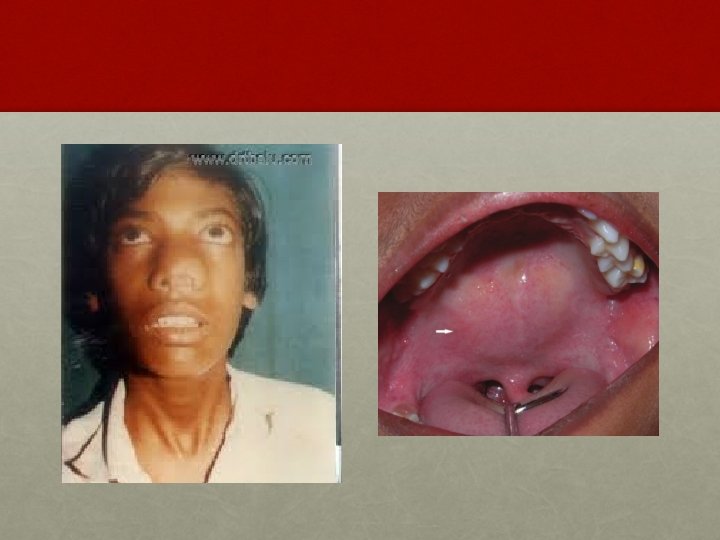
CLINICAL FEATURES: § Profuse and recurrent epistaxis. § Progressive nasal obstruction and hyponasal voice. § Conductive hear loss and middle ear effusion. § Extension of tumor in different directions produces symptoms like facial swelling, proptosis, diplopia, broadening of nasal bridge, palatal buldge and cranial nerve palsies.


INVESTIGATION: • Contrast enhanced CT scan of nose and PNS • Holman Miller sign/ Antral sign • MRI – soft tissue extent
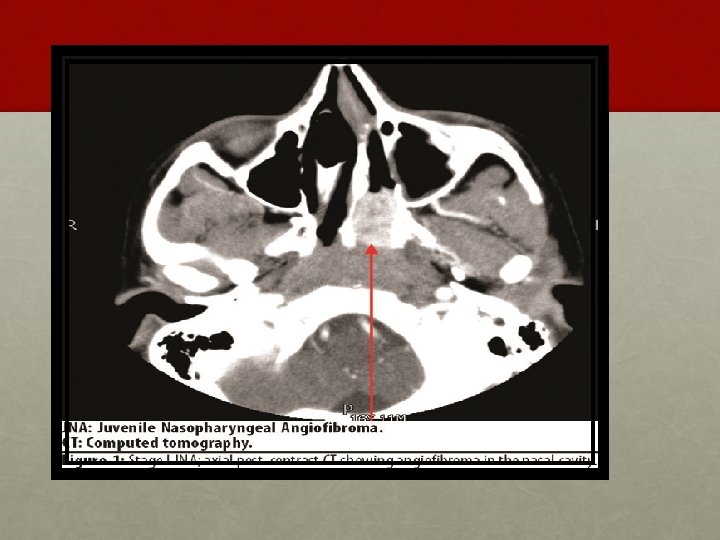

• Holman miller sign

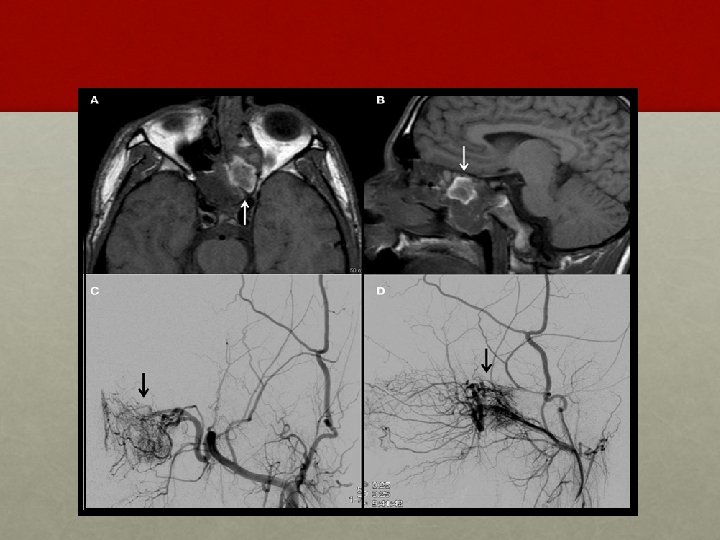
• ANGIOGRAPHY: • Carotid or four vessel angiography - vascular nature of the tumour, its feeding vessels and extension of the tumour. • In addition during angiography embolization of the feeding vessel with gelfoam can be done pre-operatively to shrink the tumour and reduce bleeding during surgery. • BIOPSY: controversial

Open Approach • Transpalatal • Transmaxillary • Maxillary swing • Midfacial degloving

Endoscopic • Shift towards endoscopic approach in last 10 years • Mostly for early disease

Endoscopic Technique

§ RADIOTHERAPY: § A dose of 3000 to 3500 c. Gy in 15 -18 fractions is delivered in 3 weeks. Tumour regresses slowly in about a year sometimes even upto 3 years. § CHEMOTHERAPY: § Recurrent and residual lesions - doxorubicin, vincristine, and dacarbazine in combination. § HORMONAL: Diethylstilboestrol and flutamide.

OTHER BENIGN TUMORS • TERATOMA • PLEOMORPHIC ADENOMA • CHORDOMA • HAMARTOMA • CHORISTOMA • PARAGANGLIOMA

Malignant tumors of nasopharynx

Nasopharyngeal carcinoma

Epidemiology • Chinese native > Chinese immigrant > North American native • Both genetic and environmental factors • India – uncommon except North East drtbalu 26

Aetiology 1. Genetic HLA histocompatibility loci possible markers 2. Viruses EBV Viral Capsid Antigen & Early Antigen 3. Environmental Nitrosamines - salted fish Others - polycyclic hydrocarbons, air pollution, tobacco smoking, smoke from burning wood drtbalu 27

Age & sex Distribution • The age incidence of NPC is different from other cancers. • It begins to rise at the end of IInd decade reaches a peak at IVth decade then stays at a plateau. • Bimodal age distribution. • Male : Female drtbalu – 3: 1 28

Classification • WHO classes übased on light microscopy findings • 3 histological types ütype I – Keratinizing SCC (25%) ütype II – Nonkeratinizing Differentiated Carcinoma (12%) ütype III – Nonkeratinizing Undifferentiated Carcinoma ( 63%) 29

Pathology • Grossly the tumour presents in 3 forms üProliferative growth causing nasal obstruction üUlcerative causing epistaxis üInfiltrative which causes cranial nerve involvement 30

pathology • Squamous cell CA – 85% • Lymphomas – 10% • Rhabdomyosarcoma, malignant mixed salivary gland tumor – 5%

spread

34
 • tendency for early lymphatic spread • commonest palpable node –")
Cervical Lymphadenopathy (60%) • tendency for early lymphatic spread • commonest palpable node – jugulodiagastric • contralateral lymph nodes metastasis (nasopharynx is midline structure) 35

Aural Symptoms • NPC leads to eustachian tube occlusion ü sensation of a blocked ear ü impaired hearing ü tinnitus ü u/l serous otitis media 36

Epistaxis and Nasorespiratory Symptoms • blood stained nasal discharge • profuse epistaxis • nasal obstruction • Hyponasal speech 37

Neurological Palsies • Most frequently involved are: ü VI - Lateral rectus palsy - Diplopia & squint ü III, IV, VI - are commonly affected together (opthalmoplegia) ü V – Facial pain & paraesthesia ü IX, X & XI - Jugular Foramen Syndrome (involvement of the IX, X, and XI CN) • Isolated single C. N. palsy common with nerves V & VI • Horner’s syndrome 38

investigations • Diagnostic nasal examination

Ct scan with contrast

investigations • Biopsy from the lesion

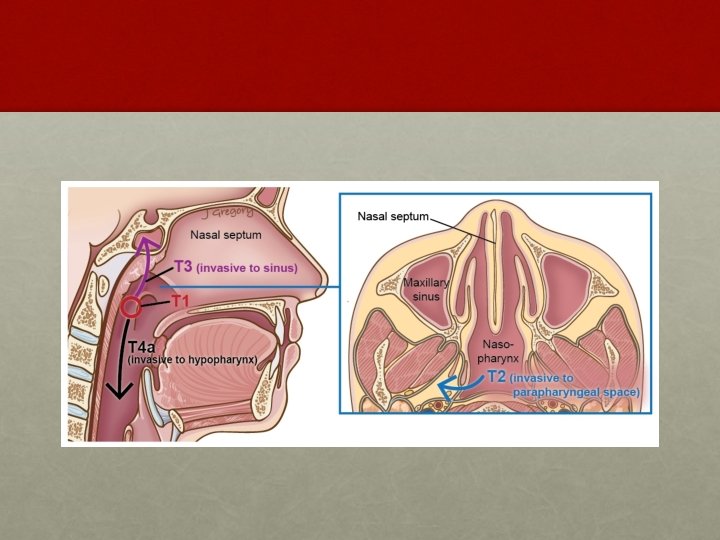
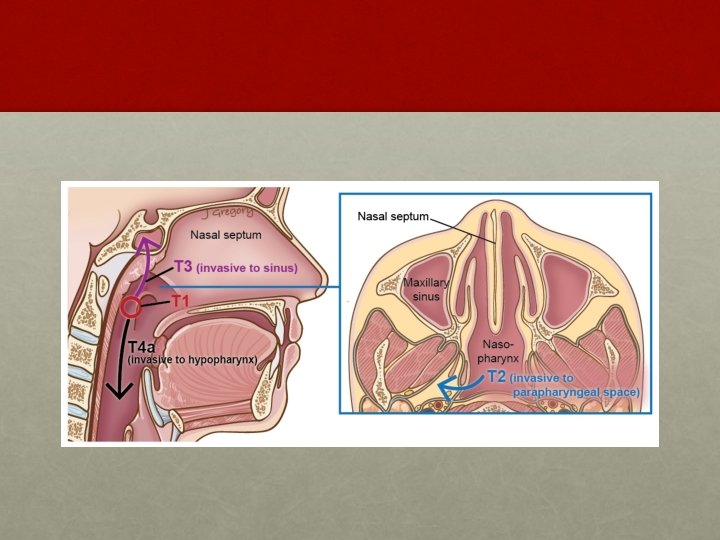
AJCC system: T staging • T 1: • Tumor confined to the nasopharynx • T 2: • Tumor extends to soft tissues • T 2 a : Extends to the oropharynx or the nasal fossa • T 2 b : With parapharyngeal extension • T 3: • Tumor invades bony structures and/or paranasal sinuses • T 4: • Tumor with intracranial extension and/or involvement of cranial nerves, infratemporal fossa, hypopharynx, orbit, or masticator space Department of Radiotherapy, PGIMER, Chandigarh

• N 0: AJCC system: N staging • No regional lymph node metastasis • N 1: • Unilateral metastasis in lymph node(s), < 6 cm in greatest dimension, above the supraclavicular fossa • N 2: • Bilateral metastasis in lymph node(s), < 6 cm in greatest dimension, above the supraclavicular fossa • N 3: • • N 3 a: Metastasis in a lymph node(s) >6 cm N 3 b: Extension to the supraclavicular fossa PGIMER, Chandigarh Ho’s Triangle

treatment • External Beam Radiotherapy üprimary mode of management of NPC – 6000 - 7000 c. Gy üat the primary site and in the neck ümainly because of tumor's high degree of sensitivity to radiation as well as the anatomical constraints for surgical access
, during (concurrent), or following (adjuvant) radiation")
Treatment • Chemotherapy ücan be delivered before (neoadjuvant), during (concurrent), or following (adjuvant) radiation therapy üactive chemotherapeutic - cisplatin, 5 fluorouracil (5 -FU) 46

treatment • Surgery: • Residual / recurrent primary tumour • Radical neck dissection for persistent disease

Other malignant tumors • Lymphomas • Rhabdomyosarcoma • Plasmacytoma • Chordoma • Adenoid cystic carcinoma • Melanoma

Thank you
- Slides: 49