TUMOURS OF NASAL CAVITY PARANASAL SINUSES Col Shoaib

TUMOURS OF NASAL CAVITY & PARANASAL SINUSES Col Shoaib Ahmed Consultant ENT Head & Neck Surgeon MBBS (Honours) FCPS(Pakistan) FRCS(Glasgow)

Review of Anatomy • Paranasal sinuses are air filled cavities that communicate with the nasal cavity • There are close anatomical relations with orbit & skull base • Cranial nerves 1 st, 2 nd, 3 rd , 4 th , 5 th and 6 th are in close vicinity

Unique Features of Sinonasal Tumours • Relatively rare of head & neck tumours • Present late Large air filled sinuses with no vital structure in immediate vicinity → remain clinically silent Highly non specific early symptoms – (rhinorrhea & nasal obstruction) → receive scant attention • Wide variety of pathological lesions • Extension to anatomically critical areas Generally advanced disease with poor clinical outcome

Classification • BENIGN • Epithelial Inverted papilloma Non epithelial Fibroma Chondroma Hemangioma Nerve sheath tumour

Classification contd. • MALIGNANT • Epithelial Squamous cell carcinoma Adenoid cystic carcinoma Mucoepidermoid carcinoma Olfactory neuroblastoma / Esthesioneuroblastoma Non epithelial Sarcomas Lymphoma Giant cell tumour

Environmental Factors associated with sinonasal malignancy • • • Wood dust Nickel Hydrocarbons Chromium Organic oils Isopropyl oil

Clinical Features • EARLY • Nasal obstruction • Rhinorrhea • • • LATE Epistaxis Proptosis Facial pain / swelling Cranial nerve dysfunction Trismus

How to identify early on ? • Can be readily mimicked by common respiratory conditions (e. g. Sinusitis ) ↓ • Unilaterality of symptoms & signs • Persistent & progressive symptoms • No improvement with antibiotics / anti histamines • Unilateral facial pain / numbness / fullness • Short span of symptoms suggests a malignant tumour

Clinical Examination • Thorough ENT head & neck examination ↓ Trismus Orbit Neurological exam (cranial nerves 1 st to 6 th) Cervical lymph nodes
 •")
Diagnosis • Clinical • Imaging (X rays, CT , MRI , PET ) • Biopsy Always done after imaging (highly vascular lesion, or intra cranial) Generally under LA

Radiological Imaging Plain X rays have lesser value ! 45 degrees Occipitomental projection – “X ray PNS”

Plain X- rays - Findings • Unilateral findings • Opaque sinus • Gross bone destruction

CT scans • • Initial investigation of choice Shows bony details Areas of bone destruction Extension into adjacent areas

Normal CT scan Frontal sinus Ethmoid sinuses

CT scan • Unilateral sinonasal mass • Bony erosion of lateral nasal wall and skull base

Inverted papilloma

Olfactory neuroblastoma in a 14 year old

MRI • Better soft tissue detail • Useful to detect intracranial extension • Able to distinguish nasal secretions from tumour • Indicates extension into dural venous sinuses
 • Routine evaluation for recurrent disease after primary tumour")
Positron Emission Tomography (PET scan) • Routine evaluation for recurrent disease after primary tumour • Mainly used for squamous cell carcinoma • Very expensive modality

TREATMENT OPTIONS • • Surgery Radiotherapy Combined surgery & radiotherapy Chemotherapy Palliation Lymphomas

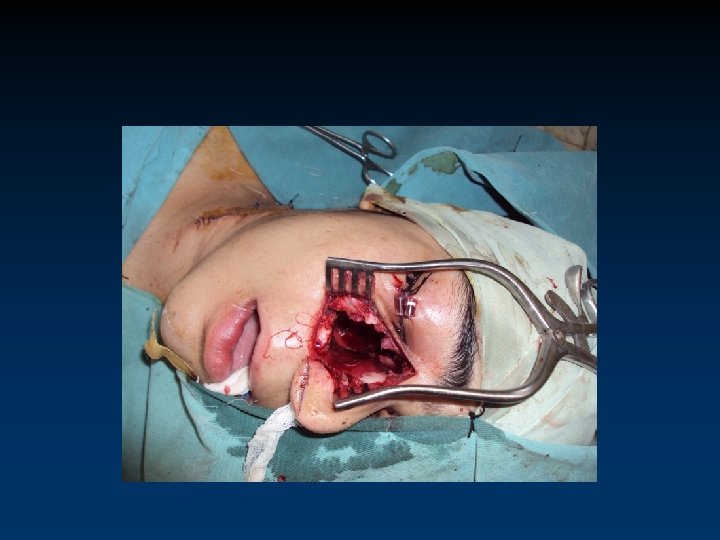
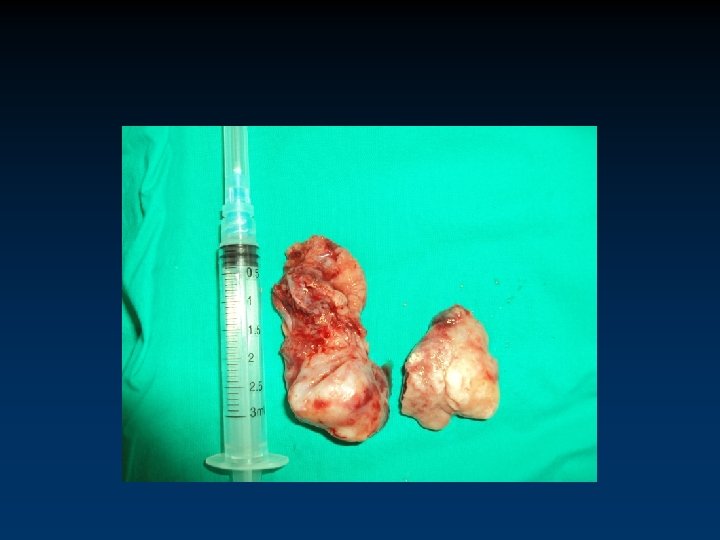
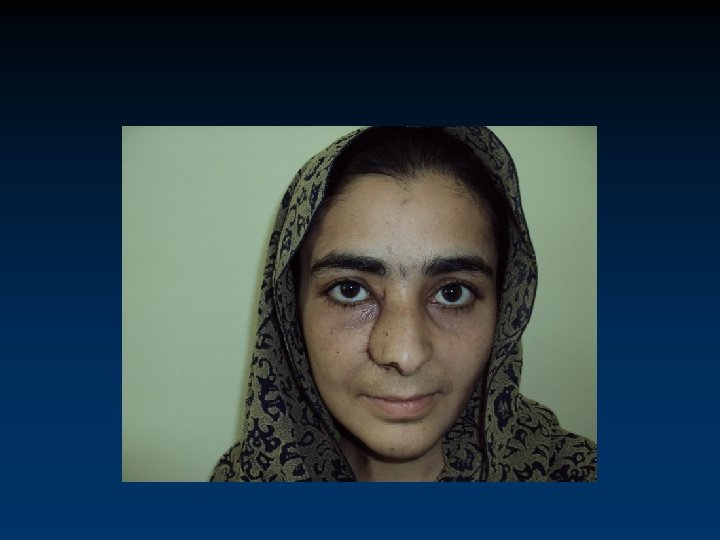
Olfactory Neuroblastoma in a young lady



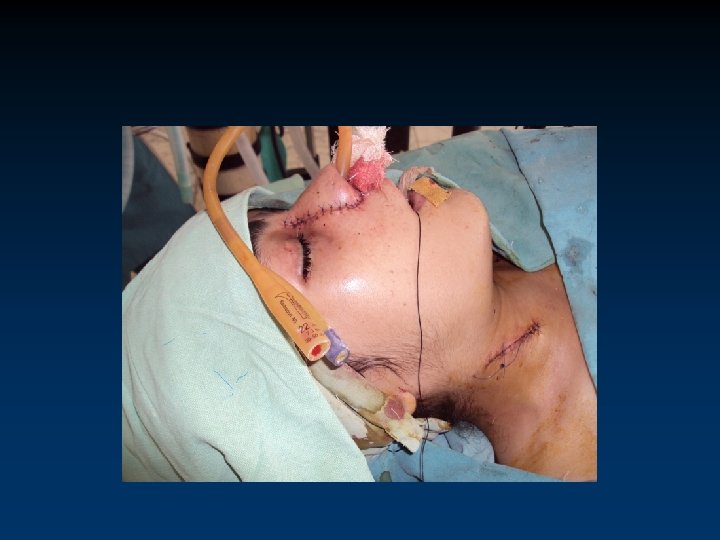

CONCLUSION • These are rare tumours with poor survival & are generally advanced at presentation • Comprise of several histologic types with varying biological behaviour • Early diagnosis requires being alert for any persistent unilateral symptoms • Diagnosis is based on CT, MRI and biopsy • For cure, extensive mutilating surgery followed by reconstruction is often required

DEPARTMENT OF ENT HEAD & NECK SURGERY COMBINED MILITARY HOSPITAL RAWALPINDI

Any Questions ?
- Slides: 31