TUBERCULOSIS PROF MANDIRA SHARMA DEPTT OF PATHOLOGY Chronic

TUBERCULOSIS PROF MANDIRA SHARMA DEPTT OF PATHOLOGY

Chronic inflammation � 1 -These organisms often evoke an immune reaction called delayed-type hypersensitivity � 2 - The inflammatory response sometimes takes a specific pattern called a granulomatous reaction. � � 3 -unregulated immune responses against microbes, as in Inflammatory bowel disease. � 4 -Immune responses against common environmental substances allergic diseases, such as bronchial asthma.

Chronic inflammation � 5 - Prolonged exposure to potentially toxic agents, either exogenous or endogenous. exogenous agent is particulate silica, � a non degradable material that, when inhaled for prolonged periods, results in an inflammatory lung disease called silicosis. � because they are characterized by repeated bouts of inflammation. � Fibrosis may dominate the late stage

MORPHOLOGIC FEATURES �chronic inflammation is characterized by: Infiltration with mononuclear cells � include macrophages, � lymphocytes � and plasma cells

MORPHOLOGIC FEATURES � • Tissue destruction, induced by the persistent offending agent or by the inflammatory cells � • Attempts at healing by connective tissue replacement of damaged tissue, accomplished by proliferation of small blood vessels (angiogenesis) , fibrosis

GRANULOMA �A Granuloma is a focus of chronic inflammation consisting of a microscopic aggregation of macrophages that are transformed into epitheliod-like cells, surrounded by a collar of mononuclear leukocytes, principally lymphocytes and occasionally plasma cells.

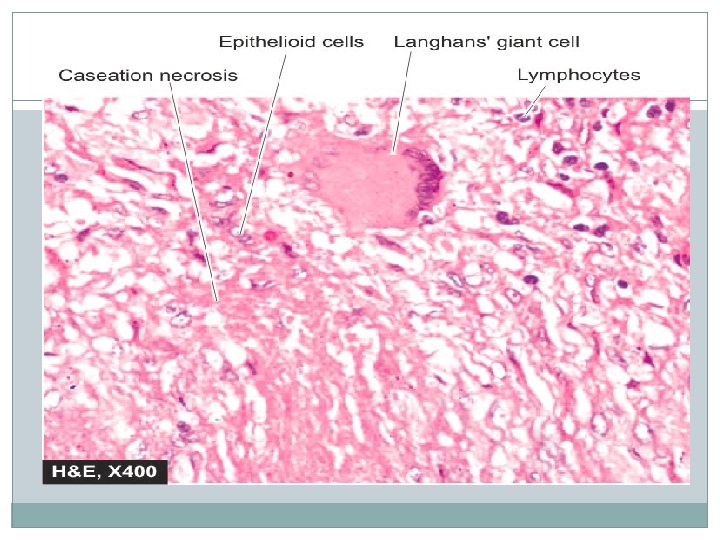
GRANULOMA � In the hematoxylin and eosin–stained tissue sections, �the epithelioid cells have a pale pink granular cytoplasm with indistinct cell boundaries, � often appearing to merge into one another. � The nucleus is less dense than that of a lymphocyte, is oval or elongated

GRANULOMA �Older granulomas develop an enclosing rim of fibroblasts and connective tissue. epithelioid cells fuse to form giant cells in the periphery or sometimes in the center of granulomas. �These giant cells may attain diameters of 40 to 50 μ m. � They have a large mass of cytoplasm containing 20 or more small nuclei arranged either peripherally (Langhans-type giant cell) � or haphazardly foreign body–type giant cell

Causes are. . � sarcoidosis, �lymphogranuloma inguinale, � leprosy � brucellosis � syphilis, � some mycotic infections � berylliosis � reactions of irritant lipids, .

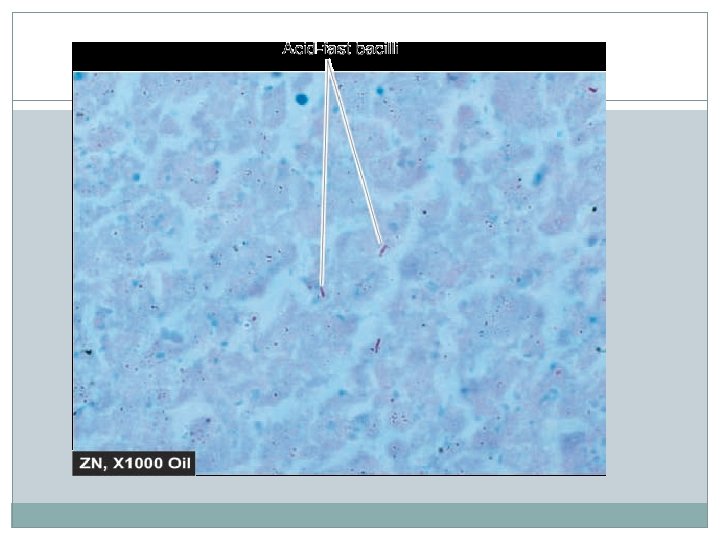
Tubercular granuloma �Mycobacterium are slender, �aerobic rods � that grow in straight or branching chains. �Mycobacteria have a unique waxy cell wall composed of mycolic acid, � which makes them acid fast, �meaning they will retain stains even on treatment with a mixture of acid and alcohol � Mycobacteria are weakly Gram positive.

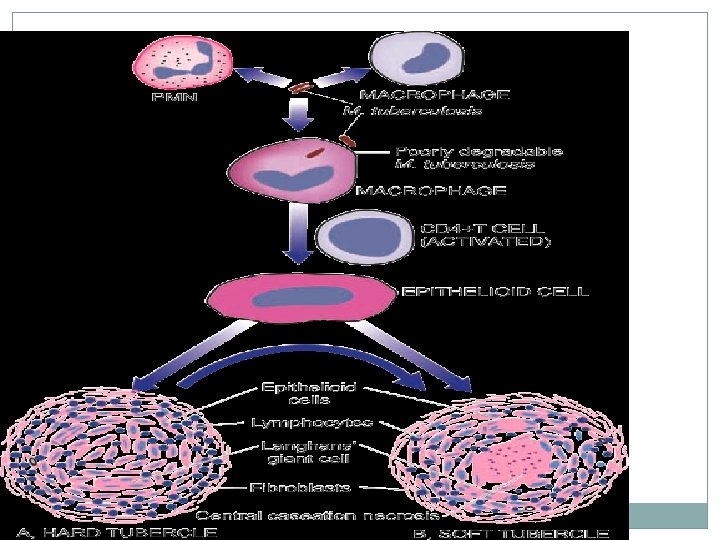
Tubercular Granuloma �They are formed as a result of T Lymphocytes response against the capsular protein of tubercle bacilli. Thus a delayed hypersensitivity response. �The activated T lymphocytes release cytokines which activates macrophages and transformed them to epithelioid cells. �Necrosis produced due to combination of hypoxia and free radical injury.

macrophages engulf foreign protein antigen process it present peptides to antigen-specific T lymphocytes causing their activation The responding T cells produce cytokines IL-2, which activates other T cells

IFN-γ �IFN-γ, � which is important in activating macrophages and transform them into epithelioid cells and multinucleate giant cells

TTuberculosis �Tuberculosis is a chronic, communicable disease in which the lungs are the prime target, although any organ may be infected. �The disease is mainly caused by M. tuberculosis hominis , but also occasionally by M. tuberculosis bovis. �The characteristic lesion is a spherical granuloma with central caseous necrosis. M. tuberculosis is an obligate aerobe, a slender, beaded, nonmotile, acidfast bacillus

Tuberculosis -Pathogenesis �The course of tuberculosis depends on age and immune competence, as well as the total burden of organisms. �Some patients have only an asymptomatic infection, whereas in others, tuberculosis is a destructive, disseminated disease. � one must distinguish between infection and active tuberculosis. �Active tuberculosis denotes the subset of tuberculous infections manifested by destructive and symptomatic disease

Mode of Infection �Droplet Infection: � Tubercular Bacilli are present in all droplet of cough or sneezes of a tubercular patient. � A person inhaling these air borne droplets gets infected. �This infects the lungs and forms primary focus( Ghons focus)in the lung from where it spreads to others regions.

Mode of Infection �Milk Borne Infection: � Ingestion of milk from diseased cow which has not been pasteurised or properly boiled can cause tuberculosis in humans. This form of spread involves intestine and causes primary tuberculosis of intestine. �intestinal tuberculosis occurs due to spread of tubercle bacilli through swallowing of infected sputum from pulmonary tuberculosis (secondary). �The ability of tubercle bacilli to infect depends on its ability to escape macrophage killing ,

Primary Tuberculosis is a First Exposure to the Tubercle Bacillus Pathogenesis and Pathology: �Inhaled M. tuberculosis is deposited in alveoli. The organisms are phagocytosed by alveolar macrophages but resist killing; �cell wall lipids of M. tuberculosis apparently block fusion of phagosomes and lysosomes, allowing the bacilli to proliferate within macrophages.

and Pathology: Pathogenesis �Development of activated lymphocytes responsive to M. tuberculosis antigen produces a type IV hypersensitivity response to the organism, � which results in the emergence of activated macrophages that can ingest and destroy the bacilli. The process requires 3 to 6 weeks to come into play.

The activated T cells kills the bacillus in three ways �Activated T helper cells (CD 4+ cells)activate macrophages through production of interferon The activated macrophages produce. O 3 and HNO 3 which kills the bacilli. In the process get modified to epithelioid cells �Activated suppressor T cells CD 8+ cells lyse the bacilli ingested macrophages and kills the bacilli.

The activated T cells kills the bacillus in three Pathogenesisways �T cells which are both CD 4 and CD 8 negative, lyse the bacilli ingested macrophages but fail to kill the bacilli. �The micro bacteria get killed in the acidic media lacking oxygen present outside the macrophages

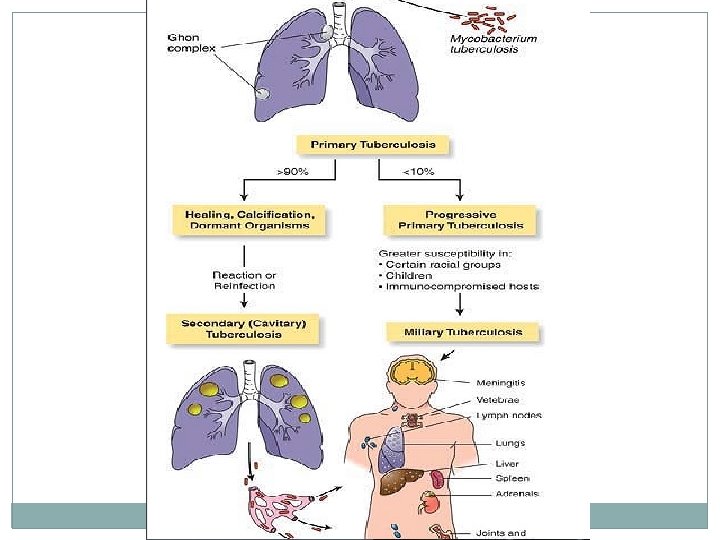
Primary Tuberculosis �If an infected person is immunologically competent, a vigorous granulomatous reaction is produced. � Microscopically, the classic lesion of tuberculosis is a caseous granuloma, a lesion that has a soft, semisolid core surrounded by epithelioid macrophages, Langhans giant cells, lymphocytes, and peripheral fibrous tissue. �Caseous necrosis is so strongly associated with tuberculosis. �The lung lesion of primary tuberculosis is known as a Ghon focus

Primary Tuberculosis �Initially, it is a small, ill-defined area of inflammatory consolidation, which then drains to hilar lymph nodes. �The combination of a peripheral focus and involved mediastinal or hilar lymph nodes is called the Ghons complex. � In more than 90% of normal adults, tuberculosis infection is self-limited. � In both lungs and lymph nodes, the Ghons complex heals, undergoing shrinkage, fibrous scarring, and calcification, the latter visible radiographically.

Primary complex or GHON’S complex � 1. Pulmonary component : solitary lesion located in the periphery � 2. The lymphatic's draining the lung lesion contain phagocytes containing bacilli � 3. Lymph node component. This consists of enlarged hilar and tracheo -bronchial lymph nodes in the area drained. The affected lymph nodes are matted and show caseation necrosis

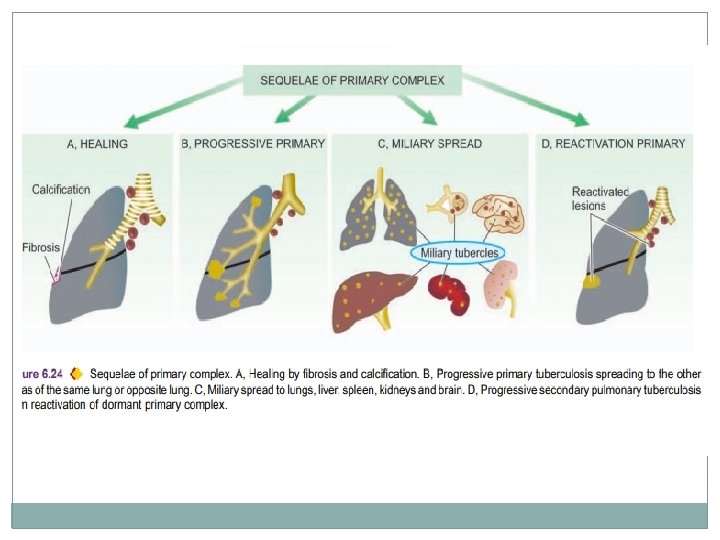
FATE OF PRIMARY TUBERCULOSIS. �The lesions of primary tuberculosis of lung commonly do not progress but instead heal by fibrosis, and in time undergo calcification and even ossification. � 2. In some cases, the primary focus in the lung continues to grow and the caseous material is disseminated through bronchi to the other part of the lung. This is called progressive primary tuberculosis.

FATE OF PRIMARY TUBERCULOSIS �At times, bacilli may enter the circulation through erosion in a blood vessel and spread to various tissues and organs. This is called primary miliary tuberculosis. � In certain circumstances like in lowered resistance and increased hypersensitivity of the host, the healed lesions of primary tuberculosis may get reactivated. The bacilli lying dormant in a cellular caseous material are activated and cause progressive secondary tuberculosis.

Progressive primary Tuberculosis �Progressive primary Tuberculosis is one were the immune response fails to control the tubercle bacilli � The Ghons focus enlarges and may even erode into the bronchial tree. � Affected hilar and mediastinal lymph nodes also enlarge. In some instances, the infected lymph nodes erode into an airway to spread organisms throughout the lungs.

Pathogenesis � previously unexposed, � immuno-competent person Cell mediated immunity gives resistance to the bacteria and also results in development of hypersensitivity to mycobacterial antigens. caseating granulomas and cavitation, are the result of the hypersensitivity
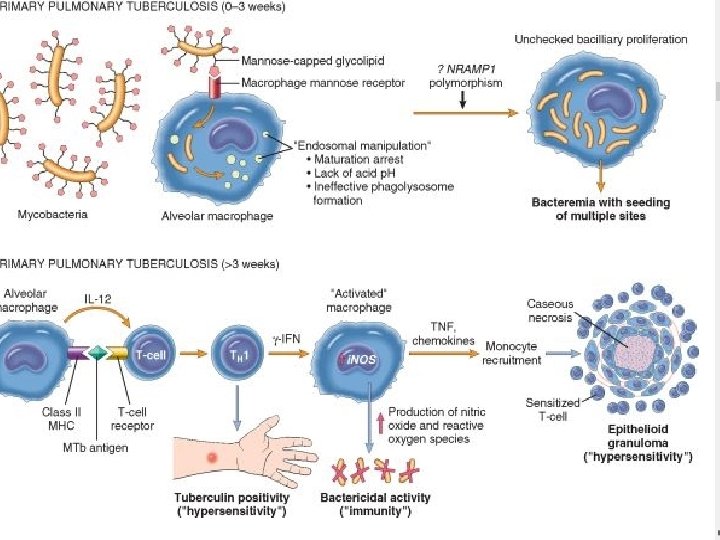

Granuloma � M. tuberculosis enters macrophages by endocytosis mediated by several macrophage receptors � inside the macrophage, � M. tuberculosis organisms replicate within the phagosome � M. tuberculosis blocks phagolysosome formation by inhabiting Ca 2+ signals
 in the non sensitized individual, �bacteria proliferate in")
Granuloma � primary tuberculosis (<3 weeks) in the non sensitized individual, �bacteria proliferate in the pulmonary alveolar macrophages and airspaces, �resulting in bacteremia and seeding of multiple sites.
 activates macrophages to")
Granulomas � 3 weeks after infection a T-helper 1 (TH 1) activates macrophages to become bactericidal. �Differentiation of TH 1 cells depends on IL-12, �TH 1 cells, produce IFN-γ.

Granulomas �INF-γ stimulates �formation of the phagolysosome in macrophages, � also stimulates expression of inducible nitric oxide synthase, � which produces nitric oxide, capable of destroying several mycobacterial constituents, from cell wall to DNA.

Secondary tuberculosis �Small numbers of organisms may remain viable for years. � Later, if immune mechanisms wane or fail, resting bacilli may proliferate and break out, causing serious secondary tuberculosis. �Secondary tuberculosis produce more damage to the lungs compared to primary tuberculosis.

Pathogenesis of secondary Tuberculosis �Any location may be involved, but the lungs are by far the most common site for secondary tuberculosis. �the bacilli proliferate and elicit an inflammatory response, causing localized consolidation � T-cell-mediated immune responses leads to tissue necrosis and production of tuberculosis cavities � These cavities contain necrotic material teeming with mycobacteria and are surrounded by a granulomatous response.
")
The pulmonary lesions may be complicated by a variety of secondary effects: � (1) scarring and calcification; �(2) spread to other areas; �(3) pleural fibrosis and adhesions; �(4) rupture of a caseous lesion, spilling bacilli into the pleural cavity; �(5) erosion into a bronchus, which seeds bronchioles, bronchi, and trachea; and �(6) implantation of bacilli in the larynx, causing hoarseness and pain on swallowing.

FATE OF SECONDARY PULMONARY TUBERCULOSIS � 1. The lesions may heal with fibrous scarring and calcification. � 2. The lesions may coalesce together to form larger area of tuberculous pneumonia and produce progressive secondary pulmonary tuberculosis. � i) Fibrocaseous tuberculosis �ii) Tuberculous caseous pneumonia � iii) Miliary tuberculosis.

Miliary tuberculosis � This is lympho-haematogenous spread of tuberculous infection from primary focus or later stages of tuberculosis. � The spread may occur to systemic organs or isolated organ. �The spread is either by entry of infection into pulmonary vein producing disseminated or isolated organ lesion in different extrapulmonary sites (e. g. liver, spleen, kidney, brain and bone marrow)
, yellowish, firm areas")
Miliary tuberculosis �The miliary lesions are millet seed-sized (1 mm diameter), yellowish, firm areas without grossly visible caseation necrosis. �Microscopically, the lesions show the structure of tubercles with minute areas of caseation necrosis

Clinical Features and Diagnosis of Tuberculosis � 1. Referable to lungs—such as productive cough, may be with haemoptysis, pleural effusion, dyspnoea, orthopnoea etc. � Chest X-ray may show typical apical changes like pleural effusion, nodularity, and miliary or diffuse infiltrates in the lung parenchyma. � 2. Systemic features—such as fever, night sweats, fatigue, loss of weight and appetite.

Clinical Features and Diagnosis of Tuberculosis �The diagnosis is made by the following tests: � i) Positive Mantoux skin test. �ii) Positive sputum for AFB � iii) Complete haemogram (lymphocytosis and raised ERR). �iv) Chest X-ray �v) Fine needle aspiration cytology of an enlarged peripheral lymph node. �Vi) Mycobacterial culture �Vii) PCR
 Purified protein derivative of tubercle bacilli is")
Purified protein derivative �Skin Test (mantoux. Test) Purified protein derivative of tubercle bacilli is injected intradermally into the volar surface of forearm Diameter of induration is measured in millimeters after 48 -72 hrs. �Positive reaction is defined as more than 10 mm diameter.

Positive reaction are seen in �Patients infected with M. Tuberculosis but not having active disease. �BCG vaccinated persons �Persons sensitized by non tubercular mycobacteria

False Negative Mantoux test �Immune Suppressed patients �Patients with overwhelming tuberculosis �Thus the test is of limited value as it has low sensitivity and specificity. �However it is most widely used screening test.

Causes of death in pulmonary tuberculosis are usually -pulmonary insufficiency, -pulmonary hemorrhage, - sepsis due to disseminated miliary tuberculosis, - cor pulmonale -secondary amyloidosis.
 Tubercular granuloma- Pathogenesis, morphology and specific features � 2)Short Notes on")
Questions � 1) Tubercular granuloma- Pathogenesis, morphology and specific features � 2)Short Notes on Ghon’s complex � 3) fate of primary tuberculosis � 4)Pathogenesis and fate of secondary tuberculosis � 5) Lab diagnosis of Tuberculosis ?
- Slides: 52