Tuberculosis and the Immune Reconstitution Inflammatory Syndrome IRIS
 Bob Colebunders")
Tuberculosis and the Immune Reconstitution Inflammatory Syndrome (IRIS) Bob Colebunders
 • Immune restoration disease (IRD) • Paradoxical")
Names • Immune reconstitution inflammatory syndrome (IRIS) • Immune restoration disease (IRD) • Paradoxical reactions

Pathogenesis • Increased lymphoproliferative response to mycobacterium antigens in vitro • Restoration of cutaneous response to Tuberculin • Increased [Il-6], activation markers (CD 38) • Associated with TNFA-308*1, IL 6 -174*G
 – Wendel")
Incidence TB/IRIS Europe and USA – Narita et al 36% (Miami, 1998) – Wendel et al 11% (Baltimore 2001) – Breen et al 29% (London, 2004) – Breton et al 43% (Paris, 2004)

Incidence TB/IRIS Africa – Breton et al: 41% – No cases in TB/DOT study in South Africa (20 patients only) India – Kumarasamy et al: IRIS of 15. 2 cases per 100 patientyears – Patel et al: TB IRIS more often in patients with active TB at the start of HAART than in those without active TB at the start of HAART (11 [8. 73] vs. 3 [2. 32%], respectively; p = 0. 0489).

Risk factors for TB/IRIS • Starting ARV’s within 6 weeks of TB treatment • Disseminated, extra-pulmonary disease • Low base line CD 4 count • Rise in CD 4 % • Fall in viral load • High bacillary burden?

Types of TB IRIS • Patient unknown to have TB at the start of HAART • Patient on TB treatment before or at the start of HAART

Timing of IRIS – Mean of 15 days after starting HAART – Up to months (years) – Syndrome lasts for 10 -40+ days

TB IRIS

TB IRIS

TB IRIS

TB IRIS

TB IRIS



TB IRIS

Prognosis – Breton et al: 16 cases of TB/IRIS: 5 ‘severe’ complications • Splenic rupture • Compressive lymphadenopathy • Ureteric obstruction – Narita et al: The study found a 6 -fold increased risk of subsequent TB relapse in patients who experienced IRIS during early TB treatment.

MRI: TB abscess spinal cord

Cryptococcal meningitis treated with HAART, bilateral blindness: fundoscopy: bilateral papiloedema: IRIS?

Differential diagnosis • Side effects of the antiretroviral treatment • Drug fever • TB infection not responding to standard anti -TB treatment • Other concomitant infection • Failure of HAART (late IRIS)

Proposed criteria for the diagnosis of IRIS in HIV patients on antiretroviral therapy French et al

Major criteria • Atypical presentation of ‘opportunistic infections or tumours’ in patients responding to antiretroviral therapy • Decrease in plasma HIV RNA level by 1 log 10 copies/m. L

Minor criteria • Increased blood CD 4 T-cell count after HAART • Increase in an immune response specific to the relevant pathogen, e. g. DTH response to mycobacterial antigens • Spontaneous resolution of disease without specific antimicrobial therapy or tumour chemotherapy with continuation of anti-retroviral therapy antiretroviral therapy

“Suspected TB IRIS”: a TB patient who after starting HAART develops either • New persistent fevers (temperature >38. 6°C) which last for more than 1 week without an identifiable source (e. g. , urine and sputa testing, and other procedures when clinically indicated) or reason (e. g. an allergic reaction) • or marked worsening or emergence of intrathoracic lymphadenopathy, pulmonary infiltrates • or worsening or emergence of cervical adenopathies/abscesses, or worsening of other tuberculous lesions or manifestations, such as cutaneous peritoneal or central nervous system (CNS) inflammatory pathology.

“Suspected TB IRIS”: a patient who after starting HAART develops TB characterised by the formation of • • Large adenopathies Abscesses Miliary TB with large nodules Cavity formation

“Confirmed” TB IRIS Same definition as suspected TB IRIS but • multi drug resistant TB excluded and • a satisfactory virological response to ART

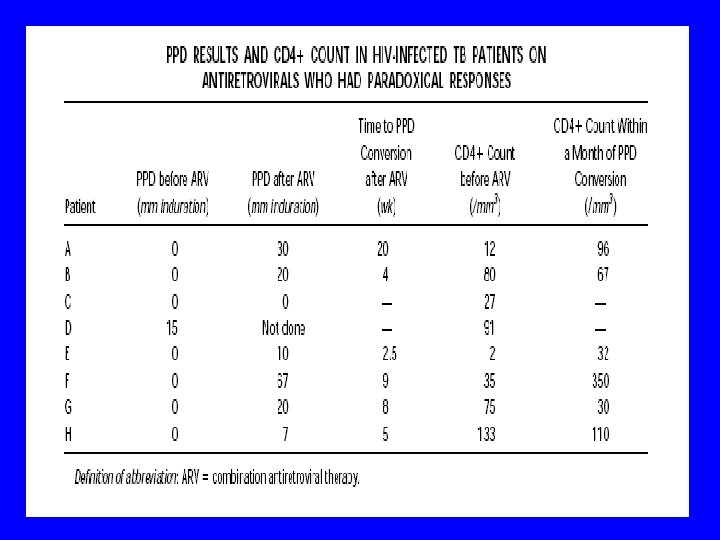
Diagnostic investigations • AFB may be be present or absent • Viable organisms despite TB treatment since > 2 months may suggest treatment failure • Tuberculin skin testing – 88% of IRIS negative – 33% of non-IRIS negative

Recommendations to prevent TB IRIS • Exclude TB before starting antiretroviral therapy • Treat first the TB and start antiretroviral treatment only once the patient has clinically improved, is tolerating very well his TB treatment • Increase awareness about TB IRIS

Treatment recommendations • TB treatment should be continued • Exclude treatment failure – Ensure adequate treatment – Ensure adherence to ATT – Consider drug resistance

Treatment recommendations • Drainage • Adding prednisolone/NSAIDS may be beneficial • Continue HAART in most cases • Consider stopping ARV’s if life threatening?

Research questions? • Propose definition of IRIS • Validate clinical definition of IRIS • Incidence of TB IRIS in different populations? • Predictors/risk factors for IRIS? • Morbidity and mortality (cause of early deaths? ) • What are the potential long term consequences?

How to diagnose TB IRIS? • What are the clinical manifestations of TB IRIS in adults and children? • Are there immunological markers or other simple laboratory parameters that could help to diagnose TB IRIS? • How useful is it to perform a tuberculin skin test prior to the start of ARVs and to repeat it when there is a suspicion of IRIS?
?")
What is the pathophysiology of TB IRIS (early and late forms of IRIS)?
? , NSAIDs? thalidomide? … Aspiration of")
How to treat TB IRIS? Corticosteroids (dose, duration)? , NSAIDs? thalidomide? … Aspiration of abscesses? Should HAART be stopped? When? Should the management of early and late TB IRIS be different?

How to prevent/avoid IRIS? • When is the optimal moment HAART should be started in a HIV/TB co infected patient? • TB prophylaxis to avoid IRIS? • Corticosteriod therapy able to prevent the development of TB IRIS?

Operational issues • How to diagnose TB IRIS clinically at the primary health level? • When should a health care worker at the primary health care level refer a patient or call for advice?

Research methods • Cohort studies • Randomised clinical trials
- Slides: 38