Tromboz ve DIC Prof Dr Tiraje Celkan kanama

Tromboz ve DIC Prof. Dr. Tiraje Celkan

kanama Tromboz

pıhtılaşma antikoagülanlar Prokoagülanlar kanama Prokoagülanlar antikoagülanlar

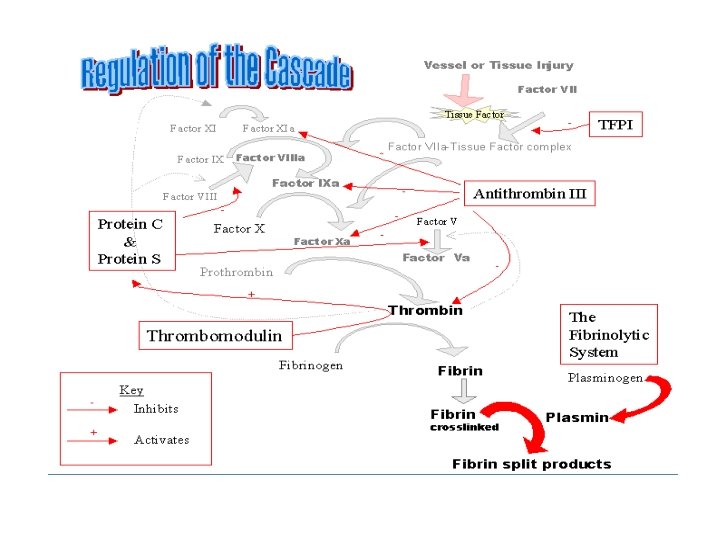
Pıhtılaşma sistemi intrensek Ekstrensek Ortak yol Thrombin Fibrinojen Fibrin trombositler pıhtı TF Kollajen Damar duvarı
. 2. Kan akımında yavaşlama (Staz). 3.")
Virchow Triadı 1. Damar duvarında zedelenme (endotel lezyonu). 2. Kan akımında yavaşlama (Staz). 3. Kanın bileşimindeki değişiklikler. HİPERKOAGULABİLİTE PRE-TROMBOTİK DURUM Rudolf Virchow - 1856

Epidemiyoloji • Insidens – 0. 7 – 1. 9 /100000 çocuk – 0. 51 / 10000 yenidoğan • 1 -2/ 1000 erişkin • her 100 kişiden 2 -5 i hayatında en az bir kere tromboz

Erişkin – çocuk trombozu • Erişkinlere göre daha nadir • Erişkinlerdeki trombozların %40’ının nedeni ? ? ? % 80 nedeni belirli • Çocuklarda hipertansiyon, diabet, sigara gibi nedenler daha az • Erişkin alt ekstremite, • Çocuk alt-üst eks.

Çocuklarda tromboz • en sık yenidoğan ve ergenlik döneminde

Tromboz nedenleri • edinsel ve kalıtsal.

• Çocukluk çağı trombozları hemen hepsi MULTİFAKTÖRYELDİR.

Trombofili Hazırlayıcı faktörler enfeksiyon

Etyolojide • Çocukluk çağı trombozların %76’sında medikal nedenler özellikle enfeksiyon ve kateter • Ancak %25 -56’sında kalıtsal neden

Enfeksiyonda Artanlar • • v. Wf artar Faktör VIII artar PAI-1 artar C 4 bp artar

Enfeksiyonda Azalanlar • Alb. Azalır • Pr. C azalır • Pr. S azalır

En sık nedenler • • AT eksikliği PC, PS eksikliği Faktör V Leiden Protrombin 20210 A mutasyonu Hiperhomosisteinemi Fak 8 yüksekliği Antifosfolipid Ak

Risk Bozukluk Toplum sıklığı % Trombozlu hastada sıklık % APC direnci F VIII yüksekliği 3 -8 11 20 25 Protrombin 20210 hiperhomosistein AT eksikliği Pr C Pr S 1 -2 5 -10 0, 02 0, 1 6 10 -25 1 3 1 -2







VENA KAVA SUPERİOR TROMBOZU BEHÇET HASTALIĞI

tanı • ÖNCE DÜŞÜN

Tromboz • Vücudun her bölgesinde damarlanma var • Her hastalık saptandığında ayırıcı tanıda akıla gelmeli

Tanı koyan hekim • % 74 hemato-onko • %11 yd • %7 yoğun bakım

amaç • Erken dönemde saptamak

tanı • Görüntüleme yöntemleri • Kan tetkikleri
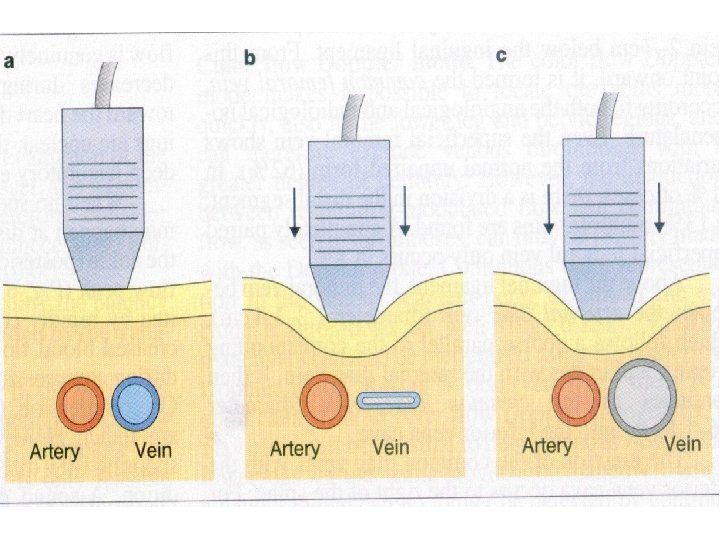
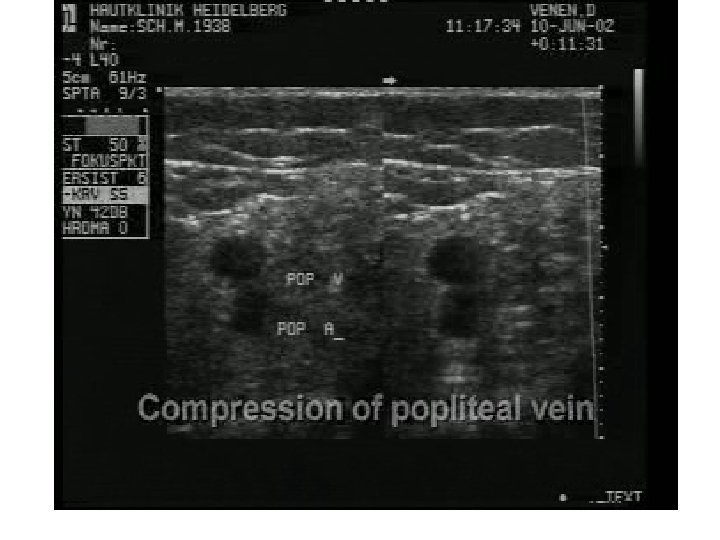
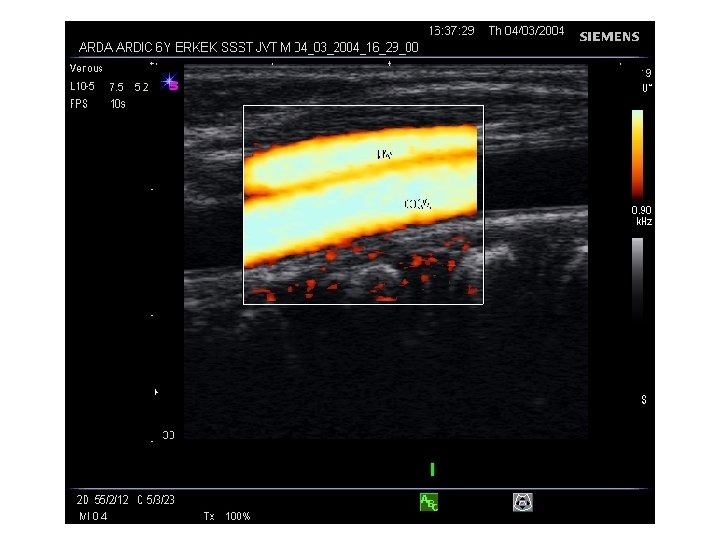
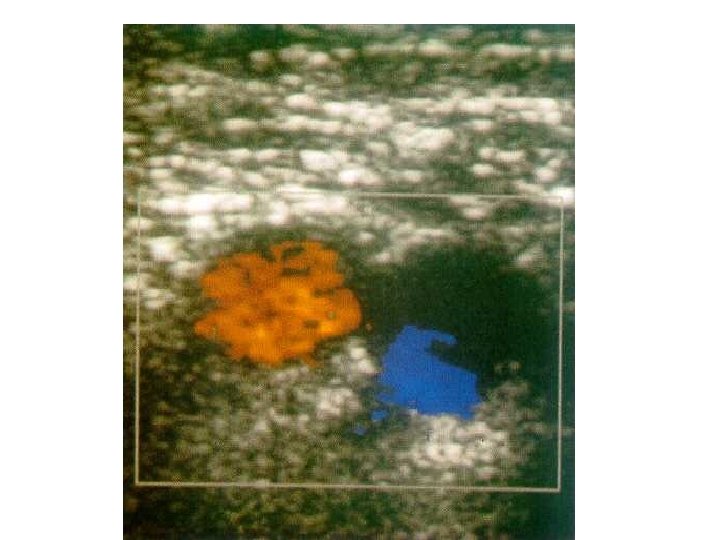
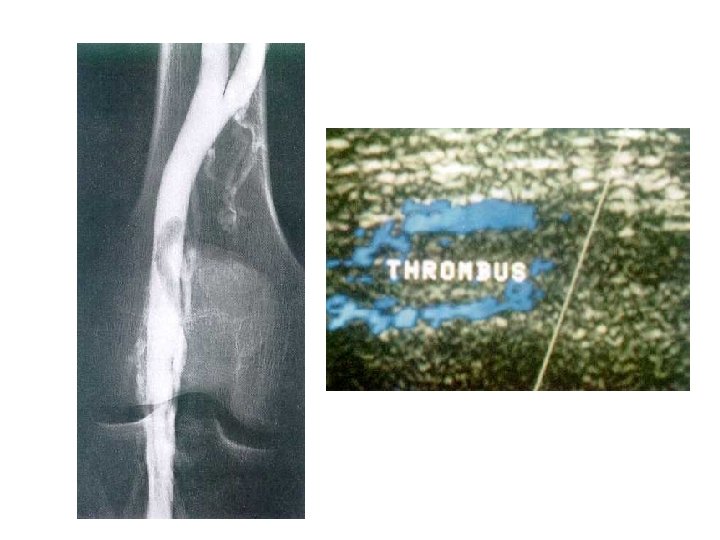

TE yeri tanı İdeal tanı a. Geçerli uygulama üst DVT venografi intratorasic: venog. boyun d. : ultrason alt DVT venografi US; venog. PE Pulm. angio ? V/Q scan, spiral BT sağ atrial TE ekokardiografi arteriel anjiografi klinik b. , doppler, isk. art. inme anjiografi MRA, MR

Testler • 1. Basamak testler – – – – Tam kan sayımı, per. yayma, akş, lipidler APCR , FVL Protrombin 20210 gen araştırması 12 saatlik açlık homosistein düzeyi AT, PRC, PRS ve serbest PRS düzeyleri FVIII aktivitesi Lupus antiloagülanları ve antikardiyolipin ak Hb elektroforezi, orak h. anemi
 Plasminojen aktivitesi Fibrinojen PNH FXII,")
2. Basamak testler: – – – – Lipoprotein (a) Plasminojen aktivitesi Fibrinojen PNH FXII, XI, IX, VII, v. WF spontan tromb. agreg. Heparin kofakt. -II t-PA – – DFYI Trombomodulin MTHFR ? Öglobin lizis zamanı

D-dimer Fibrinin plazminle parçalanması ile oluşan FYÜ olayın fibrin oluşumuna kadar gerçekleştiğine işaret akut trombozda D-dimer artmalıdır D-dimer yüksek değilse tromboz tanısı şüphelidir kanama, postop, malinite ve sepsiste D-dimer artar. Tromboza özgü değil ama (-) se tanıdan uzaklaş (negatif prediktif ) • <normalde 0, 5 altında olmalı • • •

D-dimer FIBRIN POLİMER D E D D D E D E D D D-DIMER E D D D FIBRIN yıkım ürünleri

tromboz nedeni • En sık F VIII yüksekliği, FVL ve antikardiolipin

Arteriyel • Lpa ve homosisteinemi

VENÖZ TROMBOEMBOLISM tedavi • • Heparin-düşük moleküler ağırlıklı Trombolitik-doku plasminojen aktivatörü trombolizis Oral antikoagülan-warfarin Direkt trombin inhibitörü Direkt Faktör Xa inhibitörü Indirekt Faktör Xa inhibitörü

ANTIKOAGÜLAN HEPARIN-ANTITROMBIN Faktör XIIa Faktör XIa LMWH Faktör IXa Faktör Xa Anti Xa düzeyi TROMBIN (IIa) PTT WARFARIN Faktör VII Faktör IX Faktör X PROTROMBIN (II) PT/INR

Tedavi süresi ? ? • Eğer risk Faktörleri bertaraf edilirse 3 aylık tedavi yeterli (6 -12 hafta) • Eğer risk Faktörleri devam ediyorsa 3 aylık tedavi 6 aya uzatılmalı • Genetik faktör ve hazırlayıcı neden varlığı 46 ay • Kesin ? ? • Hastaya bağlı • Oluşumunu engelllemek daha önemli

DIC DEATH is COMING • Kazanılmış bir sendrom • Olay pıhtılaşma ile başlar • morbidite ve mortalite damar içi thrombozun yaygınlığına bağlıdır • Bir çok nedeni var WWW. Coumadin. com

DIC iki mekanizma • sitokin ağının aktivasyonu ve bunun sonucunda koagulasyon sisteminin uyarılması (sepsis ve majör travmalar • Prokoagulan maddelerin kan akımına karışması (örneğin kanser ve obstetrik vakalar)

DIC patogenezi

Hemostaz • Damar Endoteli • Reoloji damar kan akım mekanizmaları • Trombositler • Koagulasyon kaskadı • Antikoagülan sistem • Fibrinolitik Sistem WWW. Coumadin. com

PLT XI TF VII IX XIa VIIa/TF TFPI VIII IXa VIIIa X V Xa Va PLT Protrombin Trombin Fibrinojen Fibrin

p. Z TF VII XIIa IX XIa VIIa/TF TFPI VIII IXa VIIIa X PS APC AT Heparin Xa V Va PLT Plazminojen Protrombin t. PA-i PLT PC XII PLT XI Trombin TAFİ Trombomodulin Fibrinojen Fibrin t. PA Plazmin FDP

DIC Koagülasyonun aktivasyonu • Kazanılmış damar içi problemi • Başlatıcı olay aktif koagülasyon sistemi Damar içinde fibrin birikmesi Küçük ve orta boy damarlarda tıkanma Organ yetmezliği Trombosit ve pıhtılaşama faktörlerinde azalma kanama ölüm

Trombotik olaylar Altta yatan hastalık Kanama Hemostatik sistem aktivasyonu Trombosit ve KF tüketimi Fibrinemi Mikrodolaşımda trombüs Fibrinolizin inhibisyonu Fibrinin parçalanamaması Organ yetmezliği Fibrinolizin aktivasyonu FYÜ oluşumu Kanamaya yatkınlık
 • AT-III düzeyinde düşüklük • Sürekli trombin oluşumuna")
DF + FVIIa FIXa + (FVIII) • AT-III düzeyinde düşüklük • Sürekli trombin oluşumuna bağlı tüketim • Aktive nötrofillerden salınan elastaza bağlı yıkım • AT sentezinin bozulması • Protein C sisteminde bozulma • Endotelde trombomodulin sunumunda azalma • PC sentezinde bozulma • Serbest PS düzeyinde azalma • TFPI yetersizliği • TFPI düzeyi normal FXa + (FV) Trombin Fibrinojen trombin oluşumu (DF aracılığı ile) Fibrin Antikoagülan sistemde yetersizlik Fibrin oluşumu Küçük ve orta çaplı damarlarda trombüs
 FXa + (FV) Plazminojen aktivatörleri Plazmin Trombin")
DF + FVIIa PAI-1 FIXa + (FVIII) FXa + (FV) Plazminojen aktivatörleri Plazmin Trombin Fibrinojen trombin oluşumu (DF aracılığı ile) Fibrin AT-III düzeyinde düşüklük Protein C sisteminde bozulma TFPI yetersizliği Fibrin Antikoagülan sistemde yetersizlik Fibrin oluşumu Küçük ve orta çaplı damarlarda trombüs FYÜ Fibrinolitik sistemin baskılanması (PAI-1 ile) Fibrin uzaklaştırılmasında yetersizlik

İnflamasyon- Koagulasyon İlişkisi Proinflamatuar sitokinler Plazminojen/ PAI-1 inh. CRP Doku faktör Fibrinoliz inhibisyonu PNL Trombomodülin inhibisyonu Elastaz AT-III / C 1 inhibitör azalması DİK Protein C azalması

Hemostatik Denge PAI-1 Antiplasmin Doku faktörü* Pıhtılaşma faktörleri Prokoagülan Prot. S Prot. C TFPI Fibrinolitik sis. ATIII Antikoagülan

DIC • Kabaca 2 evre • 1. evrede artmış trombin…. trombüs • 2. evrede artmış plazmin ……kanama

Patofizyoloji • Koagülasyonun aktifleşmesi • Fizyolojik antikoagülan sistemin devre dışı kalması • Bozuk fibrinoliz • Aktifleşen sitokinler

Patofizyoloji • Koagülasyonun aktifleşmesi – Doku faktörü/ faktör VIIa trombin oluşmasına neden olur…. . ekstrensek mekanizma çalışmaya başlar • Daha sonra 9 ve 10. faktörleri aktifleştirir – Doku faktörü • Endotel hücreler • monosit • Ekstravasküler: – Akciğer – Böbrek – Epitel hücrelerinde bulunur.

Patofizyoloji • Fizyolojik antikoagülan sistemin bozulması – Azalmış antithrombin III düzeyi – protein C-protein S sisteminde azalmış aktivite – (TFPI) doku faktör yolağında doku faktörünün inaktive edilmesinde sorun

Patofizyoloji • Bozuk fibrinoliz – Koagülasyonun en aktif olduğu sırada plazminojen aktivatör inhibitör tip 1 de artma sonucunda

Normalde • Trombin. . endotel. . . . TM+ trombin. . Pr. C aktifleştirir. . aktive FVIII inaktive edilir • TM+ trombin. . . . fibrin oluşumunu engeller

Sepsiste Sitokinler Koagülasyonun aktivasyonu Antikoagülan sis. baskılanması Fibrinolitik sis. baskılanması IL-6 TNF

sepsis • Endotel hasarı. . trombin • FX ve FVII hücre memb. ( PAR proteaz aktivated reseptör) Bağlanıp hücre içi sinyal • Hücrede p C resep artar. . Kanda p C azalır • Hücre pıhtılaşma fak. Bağlar. . . lökosit kemotaksisi artar • sitokin salınımı artar • NO ve serbest O radikalleri artar

Sepsis • • • Endotel hasar TM azalınca P C aktifleşmez Pr C kanda azalır Fibrinoliz azalır Trombüs artar APC FV, FVIII protrombinaz ve tenaz komplekslerini inhibe eder

DIC le ilişkili durumlar • Malign hastalıklar – Lösemi – Metastatik hastalık • Kardiovasküler – Kalp durmasından sonra – Akut MI – Prostatik kalp kapakçık varlığı • Hipotermi/Hipertermi • akciğer – ARDS/RDS – Pulmonary embolism • • Ağır asidoz Ağır anoreksi Kollagen vasküler hast Anafilaksi

DIC nedenleri • Infesiyöz/Sepsis – Bakteriyal • Gm - / Gm + – Viral • CMV • Varisella • Hepatitis – Fungal • Intravaskülar hemoliz • Akut kc hast • Doku hasarı – – travma cerrahi Doku nekrozu Kafa travması • Obstetrik – – Amniotik sıvı embolisi Plasental abrupyon Eklamsi Ölü fetus
 Gastrointestinal (hematemez, melena,")
Klinik • Kanama Hastaların %70 -90’nında vardır. Deri (peteşi, ekimoz, hematom) Gastrointestinal (hematemez, melena, rektoraji) Ürogenital (hematüri, vajinal kanama) Pulmoner (hemoptizi, pulmoner hemoraji) Katater giriş yerleri ve cerrahi girişim bölgeleri • Tromboembolik komplikasyonlar Hastalarda %10 -40 gibi daha düşük oranlardadır Özellikle maligniteli hastalarda sık görülür Doku ve organların disfonksiyonuna yol açar

Erkenden iskemik bulgular DIC kliniği Kanama en önemli Geç bulgu

DIC kliniği

DIC bulguları • Eritrositlerde Parçalanmalar • Şistositler • Trombositlerde azalma

Laboratuar • DIC’de kompleks fizyopatolojisinden ve alta yatan hastalıkların çeşitliliğinden dolayı değişken Laboratuar bulgularını etkileyen faktörler • Koagülasyon sistemini aktive eden stimulusun süre ve yoğunluğu • Doğal koagülasyon inhibitörlerinin durumu • Fibrinolitik sistem aktivasyonu • Karaciğer fonksiyonlarının düzeyi • Kemik iliği trombosit üretim kapasitesi • Makrofaj sisteminin aktivasyonu

Laboratuar • TARAMA TESTLERİ Trombosit Sayısı Protrombin Zamanı a. PTT Trombin Zamanı Fibrinojen Düzeyi Kolay, basit ve her yerde yapılan testler Hemostatik kompenentlerin durumu hakkında değerli bilgiler verir.

Laboratuar • TROMBİN OLUŞUMUNU GÖSTEREN TESTLER D-dimer Fibrin Monomerleri Fibrinopeptid A Protrombin fragment 1 -2 Trombin-Antitrombin kompleksi Bu testler daha kompleks Rutin laboratuarlarda kullanılmaz DIC tanısında spesifiteleri yüksek

Laboratuar Trombositopeni • DIC için sabit bir bulgudur. • İnisyal değerlerin hızlı bir şekilde azalması DIC için çok sensitivdir. • Başlangıçta trombositopenin derinliği alta yatan hastalığa bağlı olarak değişir (APL, sepsis, KChastalığı ) • Trombositopeni dışında trombosit fonksiyon bozukluğuda kanamalara katkıda bulunur. PT, a. PTT ve TT • Her üç testinde uzaması koagülasyon faktörlerinin ciddi tüketimini gösterir. • Replasman tedavisinin yönlendirilmesinde çok yararlıdırlar. • Kronik DIC’de kullanımları sınırlıdır.

Laboratuar Fibrinojen • DIC’li olguların %50’sinde düzeyleri azalır. • Akut faz reaktanı olması dolayısıyla infeksiyon, cerrahi girişim ve gebelik gibi durumlarda normal veya yüksek değerlerde bulunabilir. • KC hastalığında fibrinojen düzeyleri dikkatli değerlendirilmelidir. • %100 mg altına inen kötü prognoz işaretidir. FYÜ • DIC’de % 85 -100 olguda artar. • Plazminin fibrin(ojen) üzerine etkisi ile oluşan X, Y, D, E fragmantlarını gösterir. • Duyarlılığı yüksek olmasına rağmen özgüllüğü düşüktür. • Kanamalarda, cerrahi girişimlerde, kr. karaciğer hastalığında, AMI’de, PE’de renal yetersizlikte ve arteryal ve venöz tromboz ve tromboembolik olaylarda düzeyi artar.

Laboratuar D-Dimer • Çapraz bağlı fibrin monemerlerinin plazmin tarafından parçalanması ile oluşur • Uygun klinik bulguların varlığında DIC tanısı koymak için günlük pratikte en değerli test • 2000 ng/ml üstündeki değerler DIC için spesifik • Cerrahi sonrası, VTE, PE ve kanama varlığında 2000 ng/ml altında değerler görülebilir.

DIC tanısı koymak için en az olması gereken kriterler Ø Alta yatan hastalığın saptanması Ø Klinik olarak belirgin kanama, tromboz veya her ikisininde olması Ø Tarama testlerinden bir veya birkaçının positiv olması Ø Trombin oluşumunun en az bir testle gösterilmesi
 •")
Laboratuar • Trombositopeni – <100, 000 veya hızlı düşüyorsa – Uzamış (PT, APTT) • FYÜ veya D-dimer varlığı • Koagülasyon inhibitörlerinin azalması – AT III, protein C • Koagülasyon faktörlerinin azalması – F V, VIII, X, XIII • Fibrinojen düzeyi herzaman tanıda yardımcı olmayabilir

Ayırıcı tanı • • • Karaciğer yetersizliği Vitamin K eksikliği Karaciğer hastalıkları TTP Fibrinojenin konjenital bozuklukları HELLP sendromu

tedavi • Tetikleyici faktörü durdurmak – Kanıtlanmış tek tedavi • Destek tedavisi • Spesifik bir tedavi yok – Plazma ve trombosit süsp – Antikoagülanlar – Fizyolojik koagülasyon inhibitörleri

Plazma tedavisi • Endikasyonlar – Aktif kanama – İnvazif girişim yapılacaksa – Kanama komplikasyonları bekleniyorsa • Profilaktik TDP tedavisinin yararı gösterilmemiş • Yangına benzinle gitmek ? ? ? ? • TDP: – Pıhtılaşma faktörleri , fibrinojen, inhibitörler – Doz : 10 -15 ml/kg

Trombosit süspansiyonu • Endikasyonlar – Aktif kanama – İnvazif girişim yapılacaksa Kanama komplikasyonları bekleniyorsa – Doz: 1 unit/10 kg

Eritrosit süspansiyonu • Oksijen gereksiniminde – Kanamaya ikincil – Hemoliz varsa
 Heparin")
Koagülasyon Inhibitör Tedavisi • • Antithrombin III Protein C konsantratı (TFPI) Heparin

Antitrombin III • Koagülasyonun en önemli inhibitörü – Düzey DIC de azalır. – Antikoagülan ve antiinflammatuar etkili • Tedavide amaç AT III düzeyini normalin üzerine çıkarmak (>125 -150%). – Deneysel çalışmalarda DIC te septik şoku engelleme ve tedavi amaçlı – DIC süre, skor ve organ fonksiyonlarında düzelme – Kesin bir fayda klinik çalışmalarda gösterilememiş

Protein C – Thrombin/Trombomodulin birleşmesi ile aktifleşir – Antikoagülan ve fibrinolitik aktivite. – Vitamin K ve Protein S kofaktörü • Faktör Va, VIIIa inhibe eder • PAI-1 DIC de kullanımı deneysel – Sepsise ikincil gelişen DIC te mortalite ve morbiditeyi azaltıyor

TFPI • • TF endotel ve makrofajda TFPI trombin oluşumunu engeller TF inhibe edilmesi antikoagülan etkili R TFPI umut verici

Heparin • Kullanımı tartışmalı • Farklı sonuçlar • Fibrin depolanan veya tromboz olan hastalarda endike • Kanayan veya SSS tutulumu olanlarda tehlikeli • Doz ve kullanım şekli değişik • Etki için AT III düzeyi normal olmalı

Antifibrinolitik Tedavi • DIC te nadiren kullanım – – – Fibrinoliz trombüsü dolaşımdan temizlemede etkili Kullanımı fatal yaygın tromboza neden olabilir Tedavi amaçlı ancak : Diğer tedavilere yanıt vermeyen kanamada Laboratuar olarak artan bir fibrinoliz varsa İntravasküler koagülasyonun azaldığı bulgusu varsa • İlaç: tranexamic asid, EACA
")
Sepsis ve koagülasyonla ilişkili yeni tedaviler • • • Sentetik TFPI ( Tifacogin ) APC ( Drotecogin ) Recombinant TM AT 3 ( Atenativ ve Kybernin) C 1 inhibitörü : C 1 PK, ve FXII inhibitörü

Özet • DIC sistemik intravasküler koagulasyon • Koagulasyonla başlayıp vasküler trombozla devam eden bir süreç • İnflamasyonla koagülasyon ilişkili. • Morbidite ve mortalite riski yüksek • En önemli tedavi tetikleyen nedeni tedavi etmek
- Slides: 93