Triage Instructor Name Title Unit Triage from the






















 INPUT (Patients to be sorted) Disease Process Modifiers")






, AT")






















: – NUMBERS AND CAPABILITIES OF EVACUATION")









 – Quickly choose a casualty collection point")
 – Collect all ambulatory patients at CCP")
 – Put one of the “walking wounded”")
 – Initially treat ONLY readily correctable airway")
 – Have non-medical bystanders and uninjured or")
 – Move rapidly from one patient to")
 – Transportation Considerations / Decisions • Do")

 – Notify higher HQ and other")


 – Airway • Generally either must")
 – Circulation • Exsanguinating hemorrhage – External – usually")
 – Disability • Closed head injury with deteriorating mental")
 – All injuries that require surgery")
 – Minor soft tissue wounds not")




- Slides: 84
Triage Instructor Name: Title: Unit:
Triage – from the French sort • In casualty management sorting of a large number of injured personnel is the 1 st stage in establishing order • Triage sets the stage for treatment and eventuates in transport of the injured
Triage is not to be considered with finality • Triage categories change based upon – Number of injured – Available resources – Nature and extent of injuries(s) – State of hostile threat
Things change • Number of patients • Extent of resources • Condition of patient – Gets better – Gets worse – Transport arrives
If you have only 1 patient • That patient is Pri 1 Immediate regardless of anything else • There is no real need for triage • Once this number increases, the need for triage arises
Categories • Immediate – Threat to life/limb • A lightly injured is immediate if he can be returned to duty with immediate simple management
Urgent • Patient is at risk if treatment or transportation is delayed unreasonably
Delayed • No risk to life or consequence if more definitive care is not rendered quickly
Expectant • Regardless of the level of care rendered, patient is likely to expire • Tough call to make for unit personnel
START – triage technique • Simple treat/triage and rapid transport • All of you within the sound of my voice – Move towards me – Doesn’t work well in no/low light or excess noise
Military Triage Instructor Name: Title: Unit: COL Cliff Cloonan Assistant Professor Military & Emergency Medicine Department
Triage • Objectives – Upon completion of this block of instruction the student will be able to:
Oklahoma City Federal Building Bombing
Oklahoma City Federal Building Bombing
Triage • Definition – – “To Sort” – From the French word, “trier” – Has been defined as “doing the greatest good for the greatest number” BUT triage is simply a sorting PROCESS that when applied creates a situation that allows for “doing the greatest good for the greatest number”
Triage • What are the OBJECTIVES of doing Triage? – Rapid sorting of the more serious patients from those less serious to facilitate the rapid care of the more serious patients – When problems exceed resources, triage should facilitate “doing the greatest good for the greatest number” – Bring order to chaos thus facilitating the care of all patients
Triage • What is the PROCESS? – Sorting into categories for evacuation and treatment • What are the DECISIONS? – How will the patients be sorted – who goes in which category? – What will be done to/with the patients when sorted? • What factors AFFECT/CHANGE the decisions? – Resources – Circumstances
Triage “Normal” Triage in an ED Sorting Patients TRIAGE - A CONTINUUM Triage in A MASCAL Situation Special Situations • Persisting threat to providers/patients • “Reverse” Triage Situation
“Normal” Triage in an ED TRIAGE - A CONTINUUM Triage in A MASCAL Situation
Triage • “Military” Disasters Occur In Civilian Settings
Triage • And… “Civilian” disasters occur in military settings
Truck Accident on Pipeline Rd Saudi Arabia – Desert Shield
Resource Modifiers (Manpower, Equipment, Expendables, Time) INPUT (Patients to be sorted) Disease Process Modifiers (Illness, Injury, NBC, etc) Triage Situation Modifiers (Risk, Weather, MET-T, Combat Situation, etc…) OUTPUT (Sorted Patients) Immediate Delayed Evacuation Minimal Modifiers Expectant (Assets, Distance, Threat)
Triage • Military vs. Civilian – Are there differences? – Continuing risk to medical care providers • Can occur in both situations • More common in combat/military triage – Resource limited • Can occur in both situations • More common in combat/military triage – “Reverse” Triage Situation • Care provided first to those who when treated can be quickly returned to duty • Usually only in a military situation but could occur in a civilian MASCAL situation (when “Group” survival is at stake)
Civil War Casualty Collection Point
Civil War Casualty Collection Poin and Treatment Station
Vietnam – Mass Heat Casualties
MASCAL Exercise
TRIAGE - A DYNAMIC NOT A STATIC PROCESS
WITHIN THE MILITARY ECHELONED MEDICAL CARE SYSTEM, TRIAGE OF CASUALTIES OCCURS (OR SHOULD), AT A MINIMUM, AT EVERY ECHELON
MILITARY TRIAGE OFTEN INCLUDES, BUT IS MORE THAN, MEDICAL PRIORITIZATION
APPROPRIATE MEDICAL PRIORITIZATION AND TREATMENT OF INJURIES IN A SINGLE PATIENT IS THE GOAL OF ADVANCED TRAUMA LIFE SUPPORT TRAINING
What is the Priority Injury? What is the Triage Category? What is the Evac Priority? RPG Wound Right Knee - Somalia
What is the Priority Injury? What is the Triage Category? What is the Evacuation Priority? Burn Victim - Kosovo
Burn Victim - Kosovo
SURGICAL PRIORITIZATION, WHICH, PRIMARILY INVOLVES A DETERMINATION OF OPERATIVE PRIORITY, IS NOT TRIAGE
Triage • Surgical Prioritization Involves – Recognizing • Which patients require surgery to save life/limb/sight – Knowing • Numbers of OR’s, doctors, nurses, expendables, blood (Resources) each operation requires • Resources (manpower, equip, expendables, blood etc) required to provide post-op care • How long each operation will take (Time as a resource) • The resources that each operation will consume (Must consider manpower as a consumable resource) • Probability of successful surgery
Triage • The Goal of Surgical Prioritization – Selection of cases with the highest probability of success that consume the least amount of resources. – Make a decision - - and go with it! • Once a MASCAL situation has been declared don’t wait for the situation to evolve further before making a decision. • Making decisions is more important than what decisions are made. – Respect the Triage Decision
Grenade Fragment Wound – Perforating Bowel -ICRC Hospital Afghanistan
Transverse Abdominal High Velocity Bullet Wound -ICRC Hospital Afghanistan
Triage • Triage Categories used in ICRC Hospitals – Category I – Priority for Surgery • Patients who need urgent surgery and who have a good chance of satisfactory recovery – Category II – No Surgery • Patients with wounds so slight that they do not need surgery AND… • Patients who are so severely injured that they are unlikely to survive – Category III – Can Wait For Surgery • Patients who need surgery but not urgently
TRIAGE IN A DISASTER IS A MULTIDISCIPLINARY PROCESS. IT IS BEST CARRIED OUT BY SOMEONE WHO IS FAMILIAR WITH: • SURGICAL, MEDICAL, AND PSYCHIATRIC EMERGENCIES • ALL THE PRE-HOSPITAL AND HOSPITALBASED MEDICAL AND LOGISTICAL RESOURCES NECESSARY TO EVACUATE AND PROVIDE CARE FOR A LARGE NUMBER OF CASUALTIES
BY DEFINITION, TRIAGE IN A DISASTER / MASCAL SITUATION MEANS THAT LESS THAN THE NORMAL STANDARD OF CARE WILL BE PROVIDED FOR MANY PATIENTS.
EXAMPLE: FAILURE TO PROVIDE COMPLETE CONTROL OF THE CERVICAL SPINE IN A PATIENT WITH MULTIPLE BLUNT TRAUMA INJURIES IS CONSIDERED MALPRACTICE
EXAMPLE COMPLETE CERVICAL SPINE IMMOBILIZATION IS VERY TIME AND RESOURCE CONSUMING. THE TIME AND RESOURCES REQUIRED TO STABILIZE A CERVICAL SPINE MAY MEAN THAT OTHERS MAY DIE.
ADHERING TO THE PRINCIPLE OF DOING THE GREATEST GOOD FOR THE GREATEST NUMBER MAY REQUIRE THAT LESS THAN FULL CERVICAL SPINE IMMOBILIZATION BE PERFORMED
REMEMBER IF IT WASN'T ALL "SCREWED" UP IT WOULDN'T BE A DISASTER
REMEMBER NOT ONLY MAY CHANGES IN A PATIENT'S MEDICAL CONDITION RESULT IN A CHANGE IN HIS / HER TRIAGE CATEGORY BUT A CHANGE IN AVAILABLE RESOURCES MAY ALSO RESULT IN A CHANGE IN TRIAGE CATEGORY
CAN YOU THINK OF A SITUATION WHERE IT WOULD EVER BE APPROPRIATE TO NEGLECT THE MANAGEMENT OF THE MOST SERIOUSLY WOUNDED IN ORDER TO TREAT THOSE WITH MORE MINOR INJURIES?
REMEMBER A TRIAGE SITUATION IS NOT DETERMINED BY A SET NUMBER OF PATIENTS BUT RATHER BY A MISMATCH OF RESOURCE REQUIREMENTS WITH RESOURCE AVAILABILITY. A TRIAGE SITUATION MAY EXIST WHEN THERE ARE ONLY TWO PATIENTS
THE DECISION TO NOT RESUSCITATE A CRITICALLY INJURED PATIENT WHEN THERE ARE RESOURCES AVAILABLE TO DO SO IS NOT THE SAME AS PLACING A PATIENT IN THE EXPECTANT CATEGORY IN A DISASTER SITUATION
Triage • MILITARY TRIAGE DECISIONS ARE INFLUENCED BY: – NUMBERS OF PATIENTS AND THEIR MEDICAL PROBLEMS – NUMBERS OF EXPENDABLE AND NONEXPENDABLE MEDICAL SUPPLIES AND CAPABILITIES OF MEDICAL TREATMENT FACILITIES – NUMBERS AND CAPABILITIES OF MEDICAL PERSONNEL
Triage • MILITARY TRIAGE DECISIONS ARE INFLUENCED BY(CONT): – NUMBERS AND CAPABILITIES OF EVACUATION ASSETS – TACTICAL SITUATION – WEATHER – OTHER
TERMINOLOGY CIVILIAN USE OF THE WORD "TRIAGE" IS OFTEN NOT THE SAME AS THE MILITARY USE OF TRIAGE
IN A MULTI-CASUALTY INCIDENT WHERE THERE ADEQUATE RESOURCES THE GOAL IS TO RAPIDLY AND EFFICIENTLY IDENTIFY PATIENT NEEDS AND THEN TO MATCH THE RESOURCES WITH THE PATIENTS WHO REQUIRE THEM
IN A DISASTER SITUATION WHERE THERE ARE LIMITED RESOURCES THE GOAL IS TO IDENTIFY PATIENT NEEDS AND THEN TO DISTRIBUTE THE RESOURCES IN A MANNER THAT PROVIDES THE BEST CARE FOR THE MOST POSSIBLE PATIENTS
PROBLEMS WITH STANDARD TRIAGE TAGS
DON'T CONFUSE TRIAGE CATEGORIES WITH EVACUATION PRIORITIES
Triage • EVACUATION PRIORITIES – PRIORITY I – URGENT EVACUATION WITHIN 2 HOURS – PRIORITY IA - URGENT SURGICAL EVACUATION TO NEAREST SURGICAL FACILITY WITHIN 2 HOURS – PRIORITY II – PRIORITY EVACUATION WITHIN 4 HOURS – PRIORITY III – ROUTINE EVACUATION WITHIN 24 HOURS – PRIORITY IV - CONVENIENCE
MASS CASUALTY TEACHING POINTS
MASCAL • Field Response – What / Who do you send to the disaster site? • Equipment – Type – Stick with the basics » Dressings » Backboards/litter with straps » Tourniquets » Airways / suction devices – Quantity (lots) • Personnel – Type (Surgeon, EM…)(MD, Nurse, PA, EMT-P…) – Quantity
MASCAL • Actions on the scene – Safety and site security FIRST – Survey the scene • Estimate number and type of casualties quickly • Transmit brief initial report to Med Tx Facility • Request additional equipment (#/type) and personnel (#/type) as required
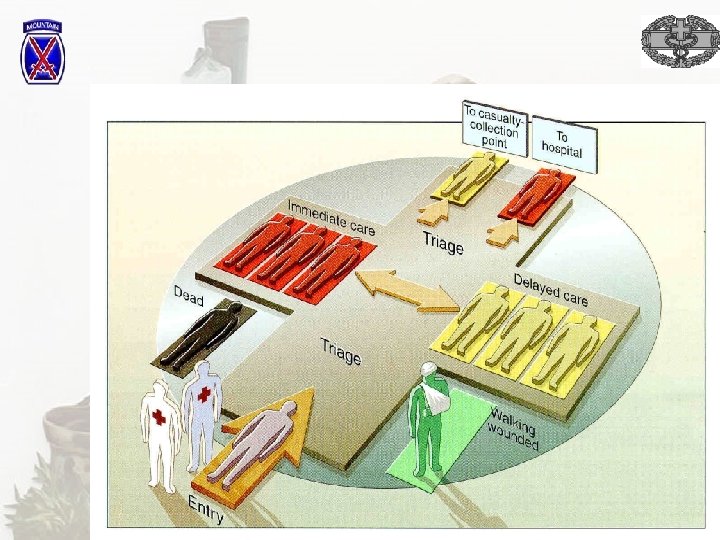
MASCAL • Actions on the scene (cont) – Quickly choose a casualty collection point based upon: • • Proximity to patients Proximity to potential helicopter landing site Safety – Distance from potential hazards, secure Geography – Large enough and appropriate for conduct of Geographic Triage) Separate sites for – – – Immediate (next to transportation) Delayed Minimal Expectant Deceased (out of sight of other victims)
MASCAL • Actions on the scene (cont) – Collect all ambulatory patients at CCP by instructing them to walk to CCP • These patients are mostly in the minimal category although some may be delayed • What they are NOT is in the Immediate / Expectant (except in some burn cases) / Dead categories
MASCAL • Actions on the scene (cont) – Put one of the “walking wounded” in charge of ambulatory patients if limited manpower at scene • Most important responsibility is to maintain accountability and keep patients from leaving CCP – If more than one medical responder divide the scene into areas of responsibility and proceed to rapidly assess / treat / triage all remaining patients who were unable to walk to the CCP
MASCAL • Actions on the scene (cont) – Initially treat ONLY readily correctable airway problems and obvious external, potentially lifethreatening, bleeding – No treatment for pulseless /apneic patients. – Place comatose patients in lateral decubitus position – then move on – Apply triage tag to identify location in CCP where patient is to be taken
MASCAL • Actions on the scene (cont) – Have non-medical bystanders and uninjured or minimally injured patients at the scene act as litter bearers (at least one experienced litter bearer / team) and move patients to CCP – Triage Officer at CCP sorts (“triages”) patients into separate geographic location based on tags • Performs rapid reassessment and changes triage category as required
MASCAL • Actions on the scene (cont) – Move rapidly from one patient to next – only identify and if possible quickly treat life threats – Identify ALL patients – Avoid becoming involved in prolonged procedures – Avoid becoming distracted by distraught, minimally injured patients – Pay attention to administrative concerns – Keep track of ALL patients (Trust me – you’ll be glad you did)
MASCAL • Actions on the scene (cont) – Transportation Considerations / Decisions • Do you put all immediate patients on the first available ambulance? • Do you send one of your health care providers if there is no medical care on the transport • To what facility do you send the ambulance? – Travel time – Level I, III trauma center? • Do you wait for a helicopter? • How secure is the route of travel?
MASCAL • Medical Treatment Facility Actions – Maintain Communication with the response team • Identify the scope of the problem • Identify the need for additional resources at the scene – – Medical Security Administrative Transportation – Ground / Air – Arrange for helicopter transportation as appropriate
MASCAL • Medical Treatment Facility Actions (cont. ) – Notify higher HQ and other medical facilities of the situation and request that they standby – Activate Medical Treatment Facility disaster response plan • Call in additional staff / keep staff in hospital at end of shift • Clear receiving area of all stable patients and set up additional beds as required • Cancel any non-emergent surgery • Clear OR’s ASAP • Prepare hospital beds – Request higher echelons preposition ambulance at your medical treatment facility.
MASCAL – Major Teaching Points • When ability to provide medical care is overwhelmed – Bringing organization to the disaster site is the most important action. • Avoid the overwhelming impulse to rush in and being to take care of first patient you come upon • Make sure that you do not become a casualty yourself
MASCAL – Major Teaching Points • Remember – All the resources that you have to deal with a disaster did not come with you to the scene • Supervising medical care and ensuring the proper evacuation order and disposition of patients may not be glamorous but it will ultimately be the most important • Keeping track of the disposition of patients may seem like a waste of manpower but its not – trust me.
Triage • Immediate (examples – not all inclusive) – Airway • Generally either must be addressed immediately at which point patient becomes either – DELAYED – DEAD • Some exceptions – Breathing • Correctable on the scene – ie. tension pneumothorax which when treated may turn patient from IMMEDIATE to DELAYED • Uncorrectable on the scene – ie. large pulmonary contusion/flail chest with hypoxia – Needs URGENT EVACUATION
Triage • Immediate (cont. ) – Circulation • Exsanguinating hemorrhage – External – usually correctable with a tourniquet and/or direct pressure at which point patient becomes DELAYED – Internal – URGENT EVACUATION • Cardiac Tamponade – Even when treated with pericardiocentesis patient remains IMMEDIATE because underlying cause is wound to the heart
Triage • Immediate (cont. ) – Disability • Closed head injury with deteriorating mental status • URGENT EVACUATION required
Triage • Delayed (examples – not all inclusive) – All injuries that require surgery but for which a delay of 4 -8 hours will not cause loss of life/limb/sight • Penetrating abdominal wounds – hemodynamically stable • All fractures requiring ORIF – hemodynamically stable • Spinal cord injury – hemodynamically stable
Triage • Minimal (example – not all inclusive) – Minor soft tissue wounds not requiring surgical intervention – Non-displaced, min. angulated, closed fractures of the upper extremities or digits
Triage • Expectant – When resources are adequate no patients are made expectant – The creation of this category presumes inadequate resources and the types of patients included in this category is largely dependent on the ratio of resources/patients – the lower the ratio, the more patients in this category. – Examples: • > 50% TBSA 2 nd and 3 rd degree burns • Unresponsive patient with an open head wound and exposed brain • Documented exposure to > 500 RADs and immediate signs of radiation sickness
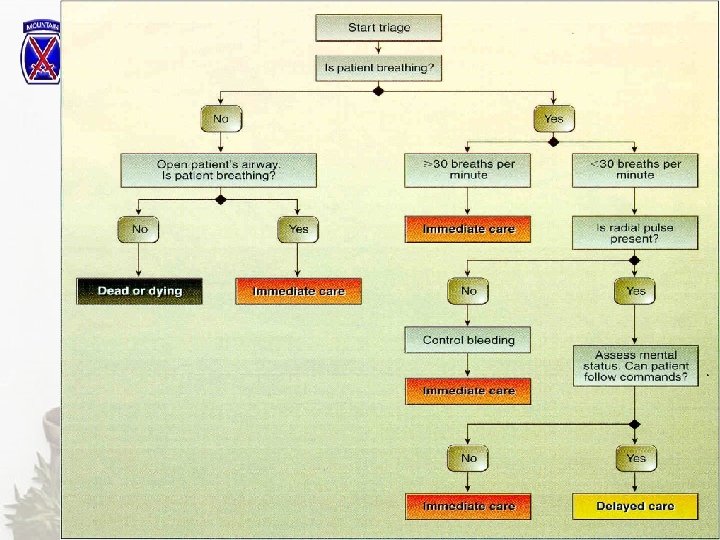
S. T. A. R. T. - Triage Classification Protocol Simple Triage And Rapid Treatment (adapted from Super, G: START instructor’s manual)
Step 1 Yes Able to Walk No Assess Ventilation Delayed Step 2 Ventilation Present No Yes Position Airway Ventilation Present? No Expectant or Dead Yes Immediate > 30/min < 30/min Immediate Assess Cap Refill
Step 3 Capillary Refill Control > 2 sec Bleeding Immediate < 2 sec Assess Mental Status Step 4 Mental Status Fails to Follow Simple Commands Follows Simple Commands Immediate Delayed